











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Since the Human Immunodeficiency Virus (HIV) was discovered in 1981, the Acquired Immunodeficiency Syndrome (AIDS) epidemic has affected the lives of thousands of people. It is estimated that, since its inception, approximately 74.9 million people have been infected with HIV worldwide and that approximately 45.1 million people are currently living with HIV, 53 % of whom are women and girls 1.
In addition, there has been a spatial expansion and an increase in the number of infected individuals through the internalization process, as well as an increase in concentration among the poorest strata (pauperization), an increase among women, and a consequent increase in vertical transmission 2.
The HIV/AIDS epidemic has been one of the greatest public health challenges in recent decades, affecting millions of people worldwide. Initially, the disease was primarily associated with men who had sex with other men and injection drug users. However, over the years, there has been a significant change in the epidemiological profile of the disease, with an alarming increase in the number of affected women 1-3.
For a long time, the incidence of HIV infections and, in particular, the development of AIDS revolved around groups referred to as "risk groups." However, today, the incidence has been steadily increasing among heterosexual individuals, with the consequent feminization of women followed by the incidence in the older age groups and an increase in resistance to antiretroviral therapies (ART) due to failure to adhere to treatment 3.
In several countries, there is still a concentrated view of infection only in minority groups that are marginalized by society in general. Я The processes of prevention, infection, treatment, and rehabilitation are complex and, despite all the advances, still require a series of combinations; among several factors is the inclusion of an understanding of social representations among the adult female population in regards to the disease 4,5.
The social representations theory is defined by Moscovici as a form of common sense knowledge that aims to understand and communicate the beliefs, images, symbols, values, and actions collectively and consciously shared in a group, society, or culture 4-6. It has become a key phenomenon in explaining cognitive processes and social interactions, guiding and organizing conduct and communication, shaping behavior and maintaining the relationship between people through communication 6.
Therefore, nursing has a crucial role in integral and humanized care, developing comprehensive care at all stages of the process, from welcoming patients to developing trust between patients and professionals. In the nursing practice, it is crucial to recognize not only physical needs but also biopsychosocial ones, which will result in excellence in care 7,8.
Understanding the unique personal and interpersonal experiences of women living with HIV/AIDS in the broader context of their sexuality will help readers, nursing teams, and other healthcare professionals to plan and implement comprehensive care measures. The aim of this study was therefore to understand the social representations of adult women living with HIV/ AIDS, available in the scientific literature.
Materials and Methods
This is a systematic review with meta-synthesis, conducted as part of the Theoretical, Historical, and Philosophical Foundations of the Nursing program at the Universidade de Pernambuco and the Universidade Estadual da Paraíba, Brazil.
Following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses - PRISMA 2020 9, the review used the qualitative meta-synthesis methodology to analyze the relevant literature. The protocol was registered on PROSPERO under the number CRD42022374651, removing the need for an ethics committee approval, which streamlines registration and ensures the reliability of the data provided 10.
The first stage used the Joanna Briggs Institute's PICo strategy for qualitative systematic reviews, where "P" stands for participants (adult women); "I" for the phenomenon of interest (what are the social representations), and "Co" for context (women with HIV/AIDS). The databases searched were Scopus, Embase, BVS, and SciELO, spanning from 2013 to 2023. The results were exported to Mendeley for duplicate removal and textual reference management.
The choice of specific descriptors such as HIV, AIDS, feminization, women, and social perception was crucial for the search to be comprehensive and precise. These terms allowed for a specific and efficient search in the databases, which ensured that the studies selected were relevant to the theme in question.
The use of the Boolean operators AND and OR was also an effective strategy for combining different descriptors and improving the search results. The combination of "HIV" AND "women" can result in specific studies on the experience of women with HIV/ AIDS, while "AIDS" AND "feminization" can broaden the search to include studies on the feminization of the epidemic in general.
The term "social perception" instead of "social representations" was a strategic decision to fill the gap in the health descriptors. This is due to the absence of the term "social representations" as a descriptor in health databases during the search period, which could have limited the search for relevant studies. Therefore, "social perception" aims to cover the perceptions and responses of individuals and groups regarding HIV/AIDS and the feminization of the epidemic. Social perception and social representation are interlinked concepts 7,8.
Social perception is how we interpret our impressions of other people and how we draw inferences regarding them, while social representation refers to how individuals and groups construct and share meanings concerning social phenomena, including diseases. These concepts influence each other and are essential for understanding social dynamics and promoting inclusion 7,8,11.
According to Jodelet, social perception is linked to social representations, which are forms of knowledge that stem from social and cultural environments. They combine affective, mental, and social elements, helping people to understand and assign meaning to the events and objects around them. Thus, the inclusion of the term "social perceptions" is relevant to correcting gaps in the literature on social representations, increasing knowledge, and supporting future research 12.
The articles were selected based on the relevance of the roles of social representations of women with HIV/AIDS in urban and/or rural contexts. The studies should only include adult women over the age of 18 in the general population and be conducted in low-, middle-, and high-income countries.
The inclusion criteria adopted were studies that covered the social representations of women in a wide range of issues related to stigmas, vulnerabilities, sexual life and protection, alcohol use, drugs, and the awareness of tests and antiretroviral treatments in their varying biopsychosocial contexts.
There were no a priori exclusions of any methodological approach, e.g., geographical and temporal location. Studies conducted in Brazil were covered whilst considering the particularities of the Brazilian sanitary context, given that, due to the social context in which the experiences were lived, the influences, choices, and preferences of the people under study were the main objective of this research.
Articles were excluded based on the following criteria: articles that evaded the theme, theses, dissertations, reviews, opinion articles, literature reviews, and books; studies that had mixed productions with men, with a definition of transgender women (transvestite, transsexual woman, aravanis, hijras, metis, etc.); young women, aged under the criminal age limit imposed by the country of study; pregnant and postpartum women were also excluded from the study due to the existing context of vulnerability in the mother-conception relationship; articles that covered interventions from different fields of knowledge and/or professionals were not included in this review.
The initial screening focused on articles on social representations or perceptions, considered synonymous with social beliefs in a broad sense. Bardin's content analysis was used to analyze the material-divided into pre-analysis, exploration of the material, and treatment of the results. The categories were defined in group meetings, with reflective and critical interpretation, based on the researchers' experience in Bardin's social representations theory 13.
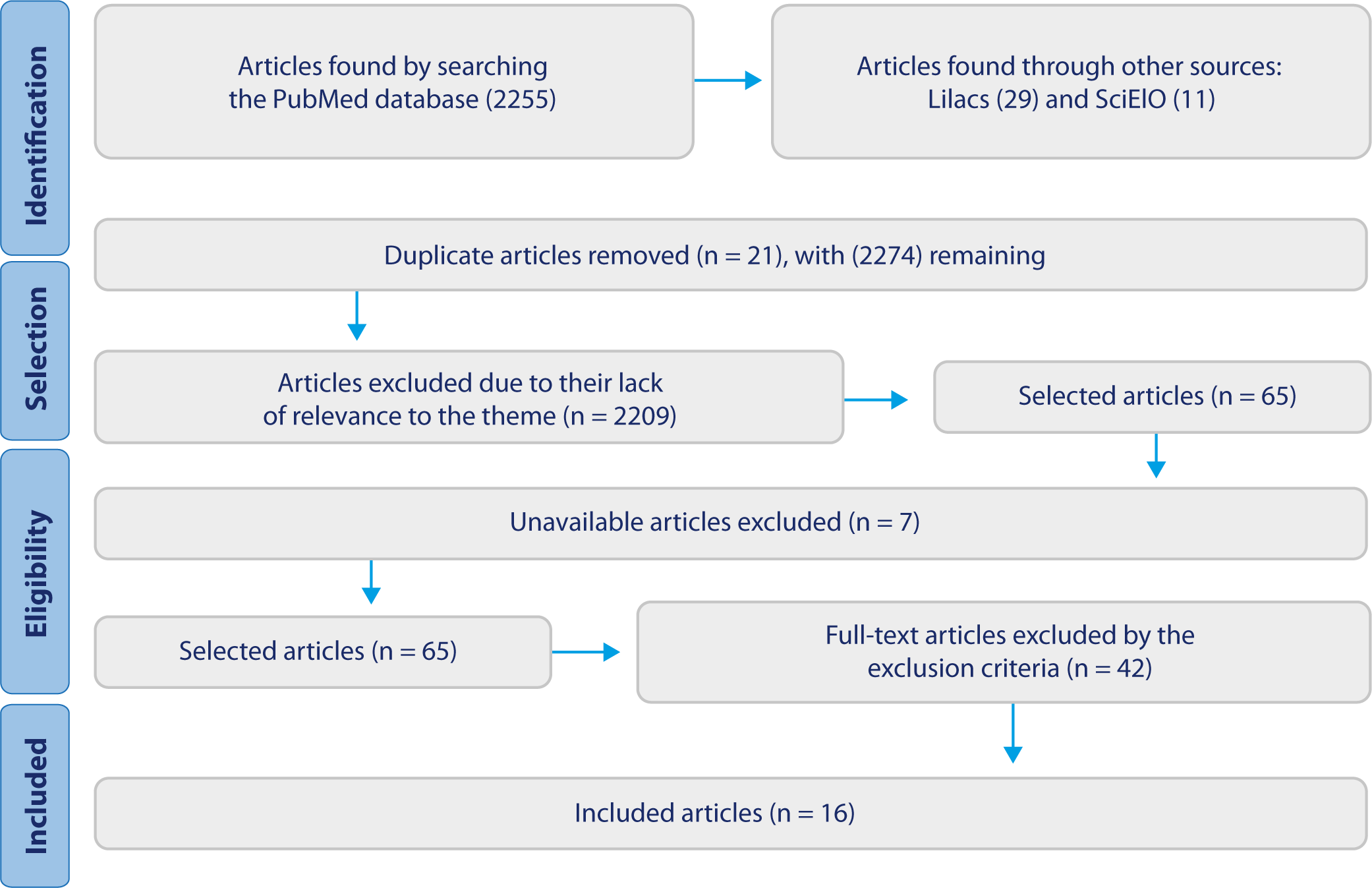
In total, 2295 articles were retrieved (2255 from PubMed, 29 from Lilacs, and 11 from SciElO). After removing duplicates and applying the inclusion criteria and analysis by title and abstract, 65 articles remained, of which 42 were excluded as they failed to meet the specific criteria after full reading of the entire material, while 7 were not available, which resulted in 16 articles that comprised this review.
Results
The studies show the feminization of HIV/AIDS is influenced by inequalities in gender, race, ethnicity, class, and moral values in varying socio-cultural contexts 6,7. Table 1 shows the categorization of the articles based on article identification, publication year and country, study objective, methods, and conclusion/outcome.
The feminization of HIV/AIDS is a complex phenomenon that reflects the deep inequalities in gender, race, ethnicity, class, and moral values present in varying socio-cultural contexts. This article aims to explore how these inequalities influence the spread of HIV/AIDS among women, highlighting the need for multifaceted approaches to fight the epidemic effectively 6,7,11.
Table 1 Characteristics of the Primary Studies included in the Meta-Synthesis, Recife, Pernambuco, 2023
Source: Prepared by the authors.
Brazil was the country most prominent in qualitative studies, with a total of 9 (56.25 %). The other countries with one study each (6.25 %) were South Africa, Mozambique, Indonesia, Chile, India, Canada, and Kenya. In terms of publication years, 2020 led the way with 25 %, followed by 2013 with 18.75 %.
The years 2017, 2018, and 2019 had 12.5 % each, while 2015, 2016, and 2022 had 6.25 % each. In these 16 studies, 1,398 women were interviewed: 12.5 % analyzed media discourses, 25 % used mixed methods, and 62.5 % were qualitative studies.
The article identified two main categories in women's experiences: sexuality, stigmas, and vulnerabilities, and preventive methods and care protocols. It reveals three main dimensions: information, image, and stance, and two socio-cognitive processes: objectification and anchoring. It highlights a complex network of beliefs and values that influence behaviors and initiatives regarding sexuality, health, and work, thus impacting prevention, treatment, and social acceptance, as shown in Table 2.
Table 2 Categories and Subcategories of the Studies, Recife, Pernambuco, 2023.
| Categories/Subcategories | Related Articles | Context of Representations | |
|---|---|---|---|
| Category 1 Sexuality as a vulnerability factor | Sexuality | A1; A2; A3; A4; A9; A10; A11; A13; A16. | HIV transmission; loss of sexual interest; violence, prostitution, and guilt. |
| Gender and stigmas | A3; A4; A6; A7; A8; A9; A10; A12; A13; A14; A15; A16. | Existentialism undermined affective relationships; sexual and reproductive rights. | |
| Vulnerabilities | A1; A3; A4; A6; A7; A9; A12; A13. | Extra-marital relationships; economic and social status; culture and tradition. | |
| Category 2 Knowledge, adherence, and representations regarding preventive methods and ART | Prevention methods | A2; A5; A10; A11; A14; A16. | Lack of knowledge regarding diagnosis; understanding of AIDS versus HIV; adherence to preservative use. |
| ART | A5; A11; A16. | Awareness of medication adherence; adverse effects of medication and treatment dropout. | |
Source: Prepared by the authors.
Consequently, it is relevant for nurses and health policymakers to incorporate this understanding into their practices and strategies. Furthermore, including women living with HIV/AIDS in g the development of policies and programs can ensure that their voices and experiences are factored in, resulting in more effective, fair, and welcoming interventions.
The high concentration of HIV/AIDS research on women in underdeveloped countries is motivated by social, cultural, and economic issues in these regions. Understanding the social representations of women with HIV/AIDS is essential to analyzing health-disease dynamics and the stigmas that impact equity in care. Public policies that disregard these social representations can fail or be harmful 13,30.
Discussion
Subcategory 1. Meanings Regarding the Sexuality of Women Living with HIV/AIDS
The women interviewed recognize that the main contamination form of HIV is through unprotected sex 11-23. However, there is a lack of knowledge concerning other forms of infection, which complicates human relations and contributes to secrecy and misinformation regarding the virus 30.
The loss of sexual interest following the discovery of an infection and the associated feelings reflect a historical illness among women. This issue is not the result of a recent epidemic, but of the delay in recognizing women as vulnerable and sexualized 10-14.
Society frequently reduces women to their traditional roles as reproducers and homemakers, subjecting them to patriarchal power. Among women, this view silences both their voices and discussions regarding sexually transmitted diseases 14-16.
The entrenchment of natural thought about women and the discovery of HIV/AIDS have led to tensions in the collective perception of the disease and female representation. In dominated societies and with reprisals against female activism, these power relations hinder changes in social awareness concerning HIV infections and the development of the disease 14,15,21.
For Jodelet, moral values and cultural norms also influence the feminization of HIV/AIDS. In several cultures, women's sexuality is surrounded by taboos and stigmas, which hinders open discussion about safe sex practices and the search for sexual and reproductive health services 31. Furthermore, in some societies, women are held responsible for HIV transmission, which further exacerbates their marginalization and vulnerability 32.
The stigma associated with HIV/AIDS can lead to social isolation and discrimination, preventing women from seeking the necessary treatment. In addition, in some societies, women are held responsible for HIV transmission, which further exacerbates their marginalization and vulnerability 33-38.
In geographical regions with lower purchasing power and social inequalities, common discourses suggest that heterosexual women in "stable" marriages have a partial or null perception of the risk of infection. This "risk-free" status associated with these marriages creates a false sense of security 21,22,32-35.
In nations with a pronounced patriarchal context, the risk of HIV and other health conditions is related to various forms of violence against women and human rights violations. Domestic violence, especially between intimate partners, is global and increases the risk of physical, psychological, and sexual health problems, including sexual infections 14-16,20.
Women, especially those from marginalized groups, face multiple forms of discrimination due to the intersectionality of gender, race, ethnicity, class, and moral values, leading to increased vulnerability to HIV and worse health outcomes 20-24.
Therefore, adopting an intersectional approach is essential when addressing the feminization of HIV/AIDS, thus recognizing and fighting the multiple forms of oppression that contribute to this epidemic.
In this sense, nursing has an important role in women's health by providing women living with HIV/AIDS with a more holistic approach, considering cultural factors, beliefs, and values. Health promotion measures should be culturally sensitive and actively involve partners, especially in healthcare appointments, to strengthen mutual support and improve adherence to health practices.
Subcategory 2. Gender Representations, stigma, and HIV/ AIDS Vulnerability
In this subcategory, the approach to the social vulnerabilities of people living with HIV is discussed in the articles. Having an HIV positive status is still strongly stigmatized, leading to social isolation and prejudice. These factors negatively influence the quality of life and coping of people living with the virus 3,15-19.
Inequalities related to HIV/AIDS in women involve multiple aspects that prove the increased vulnerability of marginalized groups. Although unequal treatment is a reality for all people living with HIV/AIDS, the literature shows that women suffer greater discrimination 14-20,36.
International literature frequently addresses the experience of stigma among men and women, but highlights that rejection is greater among women. This includes social inequalities, lower access to important and well-paid positions, and several forms of violence, such as physical, sexual, gender-based, and verbal, especially from intimate partners 25,26,36-39.
Furthermore, it concludes that women living with HIV are highly vulnerable to the negative impacts of the disease, since the 1 diagnosis entails interrelated problems, reflecting directly on rejection, isolation, and social exclusion, which renders relationships between families, the community, and the environments frequented fragile 14,20-22.
The feminization of the epidemic has been silenced and viewed as a process in which several marginalized heterosexual women started to gain space, concern, and care. These groups include sex workers, women deprived of their freedom, indigenous people, people with disabilities, and the elderly 14,20-22.
The review highlights the relationship between women and the social representations constructed by various sociocultural communities 18-23,41-43. This silencing of female voices occurs in discourses about HIV/AIDS, in line with the thoughts of Western societies. Even with distinct vulnerabilities, being a woman combined with economic, political, social, and cultural factors influences social thoughts and health strategies 35-40.
Living with HIV is marked by a lack of understanding concerning the virus and AIDS, leading to a negative self-perception of health and mental illnesses such as anxiety, depression, phobias, and embarrassment. In women, gender inequalities aggravate this situation, negatively impacting the household's income. 35-41.
In the studies 20-24, the diagnosis is surrounded by challenges, and the lack of employment or income exacerbates this situation. Working is not just having a job, but a form of empowerment, of fighting for rights and facing inequalities 38-43.
Despite the advances that have improved life expectancy and quality of life for people with HIV/AIDS, the stigma associated with the disease still negatively affects well-being and the effectiveness of therapies and prevention methods. It makes the diagnosis highly traumatic, degrading individuals and feeding harmful social processes, such as non-adherence to treatment and lack of acceptance of the condition 33,40-45.
Nurses are vital for strengthening adherence, care, and health education, especially in primary care, since in this setting nurses have more autonomy to develop inclusive public policies, with a direct impact on HIV/AIDS prevention among women.
Strategies such as educational campaigns, healthcare appointments, and the development of policies to meet women's needs are forms of encouraging and empowering them in social spaces and assuming a leading role in their health status.
Category 2. Knowledge, Adherence, and Representations of Preventive Methods and ART
HIV/AIDS among women is a public health problem that warrants attention to prevention and health promotion strategies. The feminization of the disease involves understanding the health-disease process, socio-economic-cultural relations of gender and vulnerability, and daily experiences. It is also essential to consider the progression of diagnosis and treatment over time 15,26,27.
Disease and therapy acceptance is influenced by the sociocultural context, according to the social representations theory. Adherence to treatment is a dynamic and multifactorial process that encompasses physical, psychological, social, cultural, and behavioral aspects. Negative self-perception of health, forgetting medications, physical and emotional discomfort, and a plethora of activities hinder adherence to therapy 18,47-49.
The social perception of antiretroviral medications often sustains misconceptions about the cost-benefit balance of these therapies. This is due to the perception of excessive side effects and adverse medication interactions 42-44. The stigma surrounding medication therapies often overlaps with the stigma related to negative sexual behavior in women and sexual/gender minorities 45-49.
Low adherence to ART is a threat to HIV treatment, compromising long-term effectiveness, favoring the spread of resistant viruses, and impacting public policies and the healthcare system 14-20,40-44.
In the articles selected from this review, the stigma related to HIV infection in women results in increased loneliness and low adherence to ART, with irregular adherence in 65.2% of those interviewed, increasing vulnerability to the disease and retro-contamination. It is advisable for healthcare professionals, especially nurses, to research varying scenarios to analyze behaviors and adherence to treatment to plan effective intervention measures and strategies 18,43-46.
Based on the concept of Jodelet's studies 31, when we relate social representations and adherence to treatment, it stands out that the individual, when organizing a coherent outlook for their life goal, constructs or adopts representations of the phenomenon, which constitute practical knowledge and guide their actions and behaviors in the face of the disease 48,49.
The integration of representations into healthcare practices and preventive and educational efforts made by the nursing team can reduce the adverse effects and stigma of treatment for women, especially in spaces dedicated to women's health and the treatment of sexually transmitted diseases. This facilitates social and community interactions, in addition to promoting the exchange of information and experiences in care and self-care.
Concluding Remarks
It can be concluded that the qualitative meta-synthesis of the studies enabled a brief understanding of the possible social representations worldwide, and is of greater relevance for approaching the HIV/AIDS phenomenon in women. Through a detailed exploration of the results found in the national and international literature, the various social representations of women living with HIV/AIDS were obtained in this study.
For this reason, the need for more in-depth studies on the theme became evident, especially regarding the social representation process, which is anchored in the fears, stigmas, and feelings of guilt caused by the disease and the ways of overcoming it within a social context. Among the most vulnerable groups are women, who face not only the medical complications of the disease but also a series of social and cultural barriers that can hinder access to treatment and adequate support. In this context, the nursing team has a crucial role in providing care for these women, offering support that goes beyond medical treatment and encompasses emotional, social, and cultural aspects.
This review also explores how the nursing team can help women living with HIV/AIDS by identifying and comparing social representations related to care, thereby promoting sensitive, respectful, and multi-professional care. Providing care to women with HIV/AIDS requires a multi-professional approach that includes nurses, medical doctors, psychologists, social workers, and other healthcare professionals. This integration is vital for treating physical symptoms, as well as the psychological and social impacts. Nurses have a key role in coordinating this type of care, due to their proximity to patients and their ability to offer continuous and holistic support.
In addition, these women have specific needs that the nursing team must address, such as reproductive care, emotional support, and management of comorbidities. Continuous screening and empathetic communication are essential. Furthermore, all healthcare professionals must overcome barriers such as fear of judgment and lack of financial resources to provide quality care.
For effective care, developing critical thinking and participating in continuing education and specific training is vital, thus fostering a culture of reflection and learning within academic and healthcare institutions. This involves appreciating patients' experiences and treating them with dignity and compassion. Cultural sensitivity is key, as patients may have different socio-cultural backgrounds that influence their perceptions of the disease. The nursing team must adapt their approaches to meet the cultural and individual needs of each patient.
Stigma and discrimination also negatively affect the health of women with HIV/AIDS, according to the results. The nursing team has an important role in overcoming these barriers and promoting awareness, sensitization, and inclusive care environments. The nursing team must recognize and overcome their biases. In addition, emotional and psychological support is vital when providing care to these women, and can be provided through counseling, support groups, and referrals. This type of support helps them to adhere to treatment, cope on a daily basis, and improve their quality of life.
Finally, patient education and empowerment are key elements that nurses can use to provide excellent care for vulnerable women. The nursing team can educate them on the disease, treatments, and prevention. Thus, empowerment involves developing skills and knowledge for informed health-related decisions, as well as promoting self-management, participation in care, and support in advocating for rights.

