











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
The diagnosis of childhood cancer is a particularly difficult and frightening moment in the lives of children and their families. In this context, supporting children with cancer should not only focus on the recovery of their clinical conditions, it should also be comprehensive, focusing on their well-being, quality of life, the environment around them, and the way professionals provide care 1,2.
The treatment process for children with cancer tends to be long and challenging, requiring successful adaptation so that children can use their cognitive, environmental, and affective resources, and effectively manage their emotions and behaviors when dealing with stressful events 3,4.
Coping during childhood is defined as the transactional process involving cognitive, behavioral, and emotional efforts, which are triggered to help the child avoid, escape, or act in difficult situations, aiming to reduce effects or adjust their behavior to effectively deal with adverse situations and negative events 5-8
Then, the way children deal with a difficult situation is influenced by the basic characteristics of their cognitive and social development, such as their beliefs regarding self-efficacy, self-control mechanisms, causal attribution, and relationship with the family and people around them 5,7.
In this sense, the Motivational Theory of Coping (MTC) by Ellen Skinner et al. 5,7,8, has been discussed in several Brazilian studies addressing aspects of coping with negative events in the life of children and adolescents 9-11.
This model defines coping as how people mobilize, guide, manage, energize, and direct behavior, emotion, and orientation, or how they fail to do so in stressful conditions. People not only play an active role in the transactional process of coping with adverse situations but are also shaped by this process 5,7,8. The reactions of children and how they cope with stress likely shape their social relationships, the subsequent stressors they will face and, eventually, their development 8.
Therefore, the perception that children develop of their disease is critical for them to have an active, positive, and lasting participation in the process of coping with the disease. It is known that means must be provided to help the child develop coping strategies in adverse situations experienced during the treatment. Then, board games can be considered a two-way street in the interaction with the child, through which health professionals can communicate more effectively, with understandable language, while entertaining the child.
While playing a board game, children direct their behavior through the meaning the experienced situation provides and engage in activities through which they can assume new identities, explore worlds, and learn by playing 12,13. Skuba! An Adventure under the Sea 14 is a board game for school-age children with cancer, which was developed and validated to facilitate communication between health professionals and children. The game promotes a playful learning environment, allowing children to use strategies to face challenges in an unknown environment.
Research Questions
Considering the context of the study, it is understood that a research question cannot be fully addressed when only one investigative approach is used. Therefore, to overcome the dichotomy between approaches and enable an adequate response to the question being investigated, the fusion of approaches emerges in the development of mixed-method investigations. The quantitative question that guided this study was: What are the effects of using a board game with children with cancer in terms of coping strategies? And the qualitative question was: What is the perception of children who played the game in terms of what coping strategies they used and their efficacy?
Method
Study Design
This is an intervention study that used a convergent mixed methods design, in which quantitative and qualitative data were collected concomitantly and associated for analysis in the data interpretation stage. The approaches were approximated through sequential procedures (when the results of a method are complemented with another method) and simultaneous procedures (seeking the possibilities of converging information to answer the study questions) 15,16, according to the criteria established in the 2018 version of the Mixed Methods Appraisal Tool 16.
The quantitative approach included a quasi-experimental study with the application of an intervention with pre- and post-assessment of the frequency and efficacy of the cancer child's coping strategies. The qualitative approach stage included participant observation with a focus on the child's perceptions, expressions, and interactions with the environment, and a semi-structured interview, complementing the understanding of the results obtained in the quantitative stage.
Setting and Participants
This study was conducted at the chemotherapy outpatient clinic of a referral hospital for children with cancer, in São Paulo, Brazil. Children aged 8 to 12 years with a confirmed diagnosis of cancer were considered to participate in the study. Children with a diagnosis of one month or more, undergoing outpatient chemotherapy treatment, and who had played two complete rounds of Skuba! An Adventure under the Sea 14 were included in the study. Those children who required hospitalization or surgery or who completed the chemotherapy treatment at the institution during data collection were excluded.
Quantitative Measurement
Distress and Coping Strategies
To assess the child's coping with the diagnosis of cancer, the Kid-cope instrument 17 was used in a version for children aged 7 to 12 years, adapted and validated for the Brazilian culture 18. This instrument identifies the strategies used by a child in a stressful situation, and two total scores can be obtained: frequency and self-assessed efficacy of the adopted coping strategy. Kidcope presents satisfactory reliability indexes, with Cronbach's alpha value of 0.77 for the total score 17,19.
This instrument has an open-ended question asking the child to describe a situation that he considers difficult in the context he is experiencing. Then, three other questions measure the level of distress-behavioral adaptation or disturbance and suffering-which is self-assessed by the child in the situation described by him, generating a total score of 3 to 15. Then, the instrument contains 15 items related to ten coping strategies, which are subdivided into three types: active coping (cognitive restructuring, problem-solving, emotional regulation, and social support), avoidant coping (distraction, social withdrawal, resignation, and wishful thinking), and negative coping (self-criticism and blaming others).
The first subscale corresponds to the frequency of using coping strategies by the child and the score ranges from 0 to 10. For each instrument item, the child must answer the question: Have you done that? with yes or no. Zero is attributed when the child has not used any item of that coping strategy, and one corresponds to the use of a coping strategy when the child answers 'yes' to any of the instrument items.
The second subscale corresponds to the efficacy of the coping strategy self-assessed by the child. Its score ranges from 0 to 20. For each instrument item, the child must answer the question: How much did it help you? with the options 'not at all,' 'a little,' or 'a lot,' corresponding to scores 0, 1, and 2, respectively. The score is given to each coping strategy, and not to each instrument item.
The final score obtained for the first scale indicates the number of coping strategies used by the child to deal with the treatment experience, while the total score obtained for the second scale indicates the degree of efficacy of the strategies used by the child 17,18.
Qualitative Measurement
Observation and Interview Guide
While playing the game Skuba! An Adventure under the Sea, the child's expressions and interactions with the family and the nursing team were observed. All observations were recorded in a field diary. After finishing the game and applying the Kidcope instrument for the second time, an interview was conducted with questions based on the Kidcope items and reports or expressions presenting connotations or meanings that required clarification and deep investigation. The following questions were made: In what sense did playing a game or watching TV help you forget the situation? Why did you prefer not to talk about the problem and how did it help you? How has spending time with family or friends helped you feel better?
Procedures
Pilot test
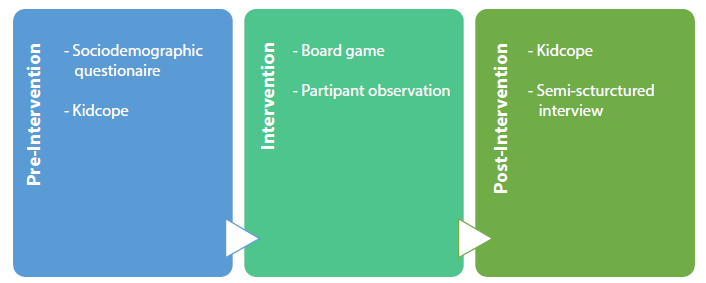
In the first stage, a pilot test was conducted with eight children, which applied the intervention and the Kidcope instrument. Aspects such as the understanding of the items by the target audience and the interval between instrument applications were analyzed. The Kidcope instrument was applied immediately before and immediately after using the board game. However, no variation was observed in the child's responses, because the child had not experienced the challenging situation again or a new one. Because of that, the interval for the application of the instrument and the interview was extended to 21 days, matching the day of the follow-up visit or a new cycle of chemotherapy. Data were collected at the chemotherapy outpatient clinic of the hospital, and the eligible children were identified by the researcher through an active daily search that took three months. Pre- and post-intervention measurements were evaluated (Figure 1).
Pre-intervention
Kidcope was applied in individual interviews, which were recorded on digital media. After the instrument application, the researcher presented the board game, its rules and objectives, and invited the child to play. During the game, with the parent's consent and the child's assent, audios were recorded on digital media with the child's expressions, questions or statements, observing the child's interaction with the game and the environment. All observations were recorded in a field diary after the child played the game. After the game, the child could provide additional comments and then the next meeting was scheduled for around 21 days later, based on the next visit of the child to the institution.
Intervention
The intervention consisted of applying the board game Skuba! An Adventure under the Sea (Figure 1). First, the game, its rules and objectives were presented and one of the researchers played the game with the child. The game is played under the sea. The main character (the child) is a navigator sailing through a big storm and is taken to the deepest region of the sea, a totally unknown environment. The navigator must be able to return to the surface of the sea, but to be successful, the navigator has to overcome situations that are associated with the experiences and challenges of the child during the disease and treatment process. Immersed in this context, the child has to use strategies to overcome the adversities. The game has luck, bad luck, negotiation, and information cards, some of them with analogies between marine characters and the child's disease/treatment; for example: "Information card - The shark has a sensor that detects the presence of the enemy, just as our body has soldiers that recognize the presence of enemies, like viruses and bacteria. Advance four spaces."
Post-intervention
At that moment, the intervention was applied again, that is, one more round of the game was played with the child, seeking to rescue the content and elements present in the cards and in the narrative of the game. After completing the intervention, the child was invited to answer the Kidcope instrument again. After data collection, notes and records were made in a field diary based on the conversations, observations of the child's behaviors, non-verbal expressions, among other aspects.
Data Analysis
Quantitative
Data from the application of the Kidcope instrument were organized in an electronic spreadsheet specifically designed for this purpose and analyzed using the Statistical Package for the Social Sciences (SPSS), version 22.0 for Windows. The sample profile was presented using descriptive statistics with calculations of mean, standard deviation, median, maximum and minimum values, as well as absolute and relative frequencies. To analyze the comparison of the frequency of coping strategies before and after the intervention, the McNemar test was used for paired samples with binary variables. To compare the level of distress or the efficacy of coping strategies before and after the intervention, the Wilconox test was applied to paired samples with more than two variables. The associations between the child's sociodemographic and clinical variables and the distress and efficacy scales were analyzed using the Spearman correlation test with numerical variables. The Mann-Whitney and Kruskal-Wallis tests were used with binary categorical variables and with more than two options, respectively. The associations between the child's sociodemo-graphic and clinical variables and the frequency of coping strategies were analyzed using Fisher's exact test. The statistical significance level of 5 % was used in all tests.
Qualitative
Data from the semi-structured interview, complementing the application of Kidcope, were evaluated using qualitative content analysis 20. The transcripts of the speeches were read in full and then codes were extracted, analyzed, and grouped into subcategories according to the coping strategies of the Kidcope instrument. After that, the data were mixed, that is, the quantitative and qualitative analyses were mixed in a comparative manner to determine convergences, divergences, and combinations. Then, data codes were integrated using a joint display strategy, which corresponds to the joint illustrative presentation of quantitative and qualitative data 15,21.
Ethical Considerations
This study was approved by the scientific committee of the study site and by the Research Ethics Committee of the Universidade Federal de São Paulo (report n° 63057616.7.0000.5505). The children provided written informed consent, and their parents signed the informed consent. To maintain the confidentiality and anonymity of interviewed children, they were identified by the letter C plus a number corresponding to the order in which the interviews were performed.
Results
In total, 35 school-age children participated in this study, mean age of 9.77 years (SD±1.33), mostly male (n=21; 60.0 °%), who had studied for 4 years (n=10; 28.6 °%). They were accompanied by the mother (n=30; 85.7 %); diagnosed with central nervous system tumor (n=15; 42.9 %) and leukemia (n=10; 28.6 %). The time since diagnosis ranged from 2 to 24 months (mean: 10.5 months; SD±5.3).
When answering the instrument, the children reported difficult situations when dealing with the disease, highlighting personal problems as the most frequent ones (n=23; 95.7 °%), which mainly includeed venipunctures during the treatment (Table 1). Communication of bad news was the interpersonal situation most mentioned by the children (n=8, 22.9 °%) (Table 1).
Table 1 Classification of Difficult Situations Reported by the Child regarding the Nature of the Problem. São Paulo, SP, Brazil
Source: Prepared by the authors.
The feeling that obtained the highest mean value both in the pre-intervention (3.02±SD 1.04) and post-intervention phases (2.62±0.84) was "feeling sad" (data not provided). The level of distress decreases after the intervention (p<0.001). Regarding the frequency of using coping strategies, the children used more coping strategies after the intervention (p=0.004), with an increase in the use of active coping (p=0.001) and avoidant coping (p=0.029). No difference was observed in the use of negative coping (p=0.157) (Table 2).
Table 2 Mean, Standard Deviations, Ranges and p Values of the Kidcope Subscales. São Paulo, SP, Brazil
| Kidcope | Pre-intervention (n=35) | Post-intervention (n=35) | p | ||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Range | Mean | SD | Range | ||
| Distress level | 7.60 | 2.45 | 4-12 | 6.66 | 1.92 | 4-11 | <0.001 |
| Strategy | 5.91 | 1.38 | 3-8 | 6.63 | 0.91 | 4-8 | 0.004 |
| Active coping | 3.29 | 0.75 | 3.80 | 0.74 | 0.001 | ||
| Negative coping | 0.09 | 0.03 | 0.157 | ||||
| Avoidant coping | 2.54 | 0.88 | 2.80 | 0.79 | 0.029 | ||
| Efficacy | 5.91 | 2.34 | 1-12 | 9.49 | 2.24 | 4-14 | <0.001 |
| Active coping | 3.60 | 1.71 | 6.09 | 1.48 | <0.001 | ||
| Negative coping | 0.09 | 0.37 | 0.03 | 0.16 | 0.157 | ||
| Avoidant coping | 2.23 | 1.14 | 3.37 | 1.14 | <0.001 | ||
Source: Prepared by the authors.
Regarding the degree of efficacy of self-assessed coping strategies, an increase in the mean scores (p<0.001) was observed, indicating the use of more efficient coping strategies by the child, mainly active coping (p <0.001) and avoidant coping (p<0.001). For efficacy, no difference was observed in the use of negative coping (p=0.157) (Table 2).
Regarding avoidant coping, the children reported they did not notice the time passing, as the game promoted distraction and learning. In addition, the records made in a field diary by the researcher during participant observation showed that, when playing, the child changes the focus away from the procedures performed at the moment, such as infusion of chemotherapy drugs, and loses the notion of time, sometimes surprised to hear the mother warning that it's almost time to leave. In active coping, the children seek to believe that everything will be fine and avoid negative thoughts, as the game makes them understand that not everything was lost (Table 3).
Table 3 Mixing of qualitative data regarding the frequency of using coping strategies before and after the intervention; qualitative data were related to the frequency and efficacy of coping strategies after the intervention. São Paulo, SP, Brazil.
| Subscale | Strategy | Kidcope items | Quantitative (n=35) | Qualitative (post intervention) | |||
|---|---|---|---|---|---|---|---|
| Pre-intervention | Postintervention | p | Frequency | Efficacy | |||
| n (%) | n (%) | ||||||
| Active coping | Cognitive restructuring | 5. I tried to see the good side of things. | 23 (65.71) | 33 (94.29) | 0.002 |
"I think it's good to look on the bright side, that everything will be fine, that it will work out" (C16, 10 years old). "I always think that not everything is lost, nothing is lost in the game, nothing is lost in life, I try to see it that way, positively" (C25, 11 years old). "I don't scream, but sometimes I cry (...) because sometimes it's terrible and it hurts" (C24, 8 years old). "When I got sick, I had to come to São Paulo, this is very bad (...) I like it here, but I wanted to stay at home because I feel better there" (C16, 10 years old). |
"I think positively, and I have faith in God and that's why I believe that in the end everything will be fine, it will be alright" (C33, II years old). "I wanted them to tell me, to talk to me, not only the psychologist, but the others too, the doctor, the nurse" (C12, 9 years old). |
| Problem-solving |
8. I tried to fix the problem by thinking of answers. 9. I tried to fix the problem by doing something or talking to someone. |
23 (65.71) | 31 (88.57) | 0.057 | |||
| Emotional regulation |
10. I yelled, screamed, or got mad. 11. I tried to calm myself down. |
35 (100.0) | 35 (100.0) | - | |||
| Social support | 14. I tried to feel better by spending time with others like family, grown-ups, or friends. | 34 (97.14) | 34 (97.14) | >0.999 | |||
| Avoidant coping | Distraction |
1. I just tried to forget it. 2. I did something like watch TV or played a game to forget it. |
25 (71.43) | 33 (94.29) | 0.008 | "The game made me forget I was here, it seems that time doesn't pass" (C18, 9 years old). "I thought the game was very important, because you are in the universe of the navigator. You are entertained, you play, you learn, you understand things, that's good" (C29, 12 years old). | "It helps a lot because we think we are under the sea, we keep imagining ourselves in the sea, moving back and forth in the sea, and then we even forget that we're here, so I thought the game was good" (C35, 12 years old). |
| Social withdrawal |
3. I stayed myself. 4. I keep quiet about the problem. |
21 (60.0) | 20 (57.14) | >0.999 | |||
| Wishful thinking |
12. I wished the problem had never happened. 13. I wished I could make things different. |
31 (88.57) | 31 (88.57) | >0.999 | |||
| Resignation | 15. I didn't do anything because the problem couldn't be fixed. | 12 (34.29) | 14 (40.00) | 0.625 | |||
| Negative coping | Self-criticism | 6. I blamed myself for causing the problem. | - | - | - | "Because it's her fault (points to the mother and smiles), she let me be pierced so many times for the exams" (C2, 8 years old). | |
| Blaming others | 7. I blamed someone else for causing the problem. | 03 (8.57) | 01 (2.86) | 0.500 | |||
Source: Prepared by the authors.
The scores obtained from the distress scale showed a negative correlation with "feeling nervous," both in the pre-intervention phase (p=0.031) and post-intervention (p=0.024), and indicates that the younger the child, the stronger the perception of nervousness in the difficult situations reported/experienced. According to the results of this study, girls seem to report more feelings of anger than boys (p=0.031). In the frequency subscale, no significant correlation was observed between the sociodemographic and clinical variables of the children in relation to the coping strategies they used, in both phases of the study. In the efficacy subscale, a positive correlation was observed between the child's age and the "emotional regulation" coping strategy (p=0.013), indicating that the older the child, the better the ability to control the emotions in a difficult situation.
With regard to the observations made during the game, it was noted that the child, although often weakened by the chemotherapy, tried whenever possible to solve problems, think of solutions, do something, or talk to someone: "The child played and explained to the nurse how he preferred to position the chemotherapy infusion equipment to facilitate his movement" (Observation Note, C30).
In terms of active coping strategies, the children revealed that they tried to believe that everything would be all right because the game made them understand that all was not lost: "I try not to think about bad things because what we think might not be true" (C14; 11 years old).
In terms of avoidant coping, the distraction offered by a game, for example, made the child feel as if they were in a different context, leading them to forget the situation they were experiencing: "We think we're at the bottom of the sea, we imagine we're in the sea and then we even forget we're here, so I thought the game was good" (C35; 12 years old).
Negative coping was reported by only a few children when, for example, they referred to their parents' guilt for allowing the venipuncture: "Because it's her fault (points to her mother and smiles) that she let them cheat me so much for the blood test" (C2; 8 years old).
In the mix of qualitative data with the frequency and effectiveness of coping strategies before and after the intervention, it is possible to observe the approximation of an adequate response to the question investigated in this study (Table 3).
Discussion
A child with cancer experiences daily situations that cause distress, pain, and fear. These situations must be considered by health professionals who assist them so they can plan strategies with the family to minimize damage to their physical and mental health. In this study, it was very important to understand the situations considered as difficult by the children during their chemotherapy treatment and which of these situations make them mobilize resources to face them.
Personal problems, such as venipuncture, discomfort caused by signs and symptoms related to the disease and treatment, and clinical or surgical complications, were the most difficult situations mentioned by the children, which triggered feelings such as nervousness, anger, and mainly sadness, for limiting their physical conditions and affecting their daily lives.
When the condition of disease and hospitalization becomes a research topic in the area of coping, the stressor most reported by children is exposure to invasive medical procedures 22-24. The children must be able to recognize these situations so that they can develop strategies for their emotional self-regulation. It is about making the children able to adjust their affective, behavioral, and attention responses to deal with difficult situations during cancer treatment.
By giving voice to the children, and as they progress in the game and receive encouraging cards, they feel more capable and secure in challenging situations, assuming more active behaviors, and they change the focus away from the clinical procedures. After the intervention, a significant increase was observed in the use of the distraction and cognitive restructuring coping strategies, reinforcing the main objective of developing a board game which is to provide entertainment and pleasure for the child, increasing their distraction time and helping them feel stronger to face the disease. Also, with the game, it is possible to offer information that minimizes doubts and explains the reason for some signs and symptoms the child experiences. Distraction is one of the coping strategies most used by children with cancer 25-27, particularly when they have to cope with hospitalization 28.
The children's engagement with the game made them forget that they were in a hospital environment, in a clinical procedure or receiving medication that caused undesirable side effects. In addition, the game narrative and metaphors promoted a more positive perception of the difficult situations experienced by the child. The game allowed child distancing and immersion in another context, providing a return to "being a child," which is often forgotten in the hospital environment. Active coping strategies were also considered more effective after the intervention, as the game encourages the child to change the focus away from the problem.
The board game also helped increase the efficacy of other strategies, such as problem-solving, emotional regulation, social support, and resignation. The child's interaction with the game helps redefine the child's experience with the disease through the symbols and meanings in the game. When the children can talk to someone about the problem, it can help them cope with it; however, they do not see themselves as subjects of rights, that is, the professionals do not take them into account, always talking to the parents or guardians about the disease and the treatment.
It is essential to include the child in the communication process between the health professional and the family, since communication is mostly and mainly with the mother, while the child is excluded from it. Information about the child's health is provided by parents and the relationship between the health professional and the child is restricted to affective contact with the family 29-31.
Despite the increase in the scores of coping strategies in the post-intervention period, it does not mean the children will use more effective strategies, as it will depend on the type of situations they will experience and the availability of resources to help them in this process. The use of a coping strategy should not be considered intrinsically effective or not, adaptive or mal-adaptive 32,33.
This study validates the positive effects of using a board game as a resource to help the child face difficult situations related to a disease such as cancer but also highlights the use of this tool in the communication of nurses with children, enabling attentive listening and sharing of information about the disease and treatment.
Limitations
It is important to emphasize that, despite the game reflecting in the child's imagination, its effects were evaluated in a short period. Then, this intervention cannot be considered as a punctual action by health professionals but incorporated into the care provided to children with cancer, so that this resource can bring benefits during the treatment process.
Conclusion
The board game helped decrease the level of distress, favored the use of coping strategies of distraction and cognitive restructuring and increased the efficacy of active coping strategies of cognitive restructuring, problem-solving, emotional regulation, and social support, as well as avoidant coping strategies of distraction and resignation.
The child's interaction with the game helps the child redefine the experience with cancer, learning new ways to cope with the situation based on the symbols and new meanings acquired. The board game Skuba! An Adventure under the Sea had a positive effect on the frequency and efficacy of coping strategies used by children with cancer.

