











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Noncommunicable diseases (NCDs) accounted for seven of the ten leading causes of global mortality between 2000 and 2019, with a predominance of cardiovascular diseases, respiratory conditions, and neonatal disorders. Among these, ischemic heart disease was the leading cause, responsible for 16 % of deaths, with an increase of more than two million deaths during the analyzed period 1.
In Brazil, the national epidemiological profile reflects this scenario, where cardiovascular diseases (CVDs) have been the leading cause of death. Between 1990 and 2019, ischemic heart disease (IHD) remained the primary cause of mortality, the most prevalent condition was acute myocardial infarction (AMI) 2.
Early diagnosis is crucial to guide patients toward the most appropriate therapeutic approach, which range from minimally invasive procedures, such as cardiac catheterization and/or angioplasty, to more complex and highly invasive interventions, such as coronary artery bypass grafting (CABG) 3.
CABG is a highly invasive open-heart surgery that entails greater tissue trauma, longer hospitalization, and a more demanding rehabilitation process, requiring structured pre- and postoperative care to optimize outcomes 3. It aims to restore the heart's functional capacity and reduce symptoms by optimizing blood perfusion to the myocardium 4 and is indicated when there is no possibility of clinical treatment or less invasive techniques, such as MICS-CABG, TMR, or PMR 5. This surgical experience triggers intense emotional responses, which are characterized by fear of the disease progressing, uncertainty, and psychological distress, which affect both patients and their families throughout the perioperative period.
In the postoperative phase, individuals undergoing CABG may experience feelings of restlessness, fear, vulnerability, and insecurity, with difficulties to adapt upon returning home 6. Moreover, the system of beliefs and values acquired throughout life can interfere with the recovery process.
Adequate access to health information enhances knowledge and strengthens skills essential for postoperative self-care, thus promoting the adoption of behaviors that facilitate lifestyle modifications. Participation in structured educational interventions, such as cardiac rehabilitation programs, has demonstrated to significantly improve patients' understanding of surgical wound care, management of postoperative complications, and adjustment to the challenges imposed by cardiac surgery 7.
It is necessary to link actions aimed at promoting health and preventing complications in patients undergoing CABG to facilitate their recovery. Therefore, the identification of aspects related to disease knowledge and understanding of behaviors related to their health and illness, understood as health literacy (HL), are necessary to improve quality of life and help in the elaboration of ways to prevent or early detect complications 8.
HL is defined as a set of skills developed by searching, under- b standing, and coding health information for incorporation and = appropriate daily decision-making, using a three-dimensional f approach: Functional literacy (skills to read and write); interactive literacy (understanding of information and meanings of different forms of communication, as well as its applicability in the execution of daily tasks); and critical literacy (ability to critically analyze the information received) 9-10.
Faced with the complexity of analyzing HL, disease knowledge and the challenges of the rehabilitation process for this profile of patients, it was proposed to conduct a mixed-methods study 11. This method allows answering the research problem with a broad approach since its purpose is to obtain different and & complementary data on the same topic, in addition to allowing triangulation between quantitative and qualitative methods. Therefore, it possible to directly compare quantitative statistical results with qualitative findings and development a more complete understanding of the subject under analysis.
Thus, the following research questions emerged: Is there a relationship between knowledge of disease and HL in the late postoperative period of cardiac surgery due to infarction? What are the challenges experienced during the cardiac rehabilitation process? This research aimed to analyze disease knowledge and HL in the late postoperative period of cardiac surgery due to infarction, as well as to recognize the challenges experienced in the rehabilitation process.
Method
Study Design
This is a mixed-method and convergent parallel study 11. Both phases received the same weight, being defined as QUAN + QUAL, and theoretical interpretation was implicit 12. This methodology allows the combination of quantitative and qualitative results in a new structure, with the potential of generating unique insights into the phenomena under study 13. Quantitative and qualitative data were collected simultaneously and then compared to determine convergences or differences 11. Explanations of the phenomenon and recommendations based on accumulated evidence generated by this study, combined with the literature, are presented in the discussion section 14.
Several data integration points were described. First, all the quantitative data from the total sample of participants were presented. Second, all participants were interviewed aiming at the qualitative objective. Both data sets were analyzed together to answer the comprehensive, mixed-methods research question. The integration of quantitative and qualitative elements can improve the quality of a mixed-methods study and, therefore, generate important evidence for improving services, health, and public systems 15.
The quantitative stage was conducted with the help of the Strengthening the Reporting of Observational Studies in Epidemiology guidelines 16. The qualitative step was analytical-descriptive and was guided by the Consolidated Criteria for Reporting Qualitative Research 17. As for the mixed method, the Mixed Methods Appraisal Tool 18, translated into Brazilian Portuguese, was the instrument that helped in methodological rigor analysis.
Setting and Study Period
The study was conducted in the participants' homes in the Western Paraná mesoregion, Brazil. Data collection occurred between December 2020 and April 2021, during the COVID-19 pandemic.
Population and Selection Criteria
The eligible population consisted of 44 patients who had AMI and underwent CABG in a referral hospital in cardiology in western Paraná, Brazil. They were identified by analyzing the medical records of surgeries performed in the final half of 2019.
Patients affected by AMI and submitted to CABG, aged >18 years, and who reached the minimum score in the Mini-Mental State Examination (being 13 points for non-literates and 18 points for low and medium education) were included.
Thus, 20 patients were excluded: the address of 10 of them was not found, five died, three had inability to communicate, reported by a family member, and two refused because of the COVID-19 pandemic. A total of 24 patients composed the study sample.
Data Collection Procedures
Participants were identified through hospital records and invited by telephone. After consent, quantitative data was collected via the Strengthening the Reporting of Observational Studies in Epidemiology guidelines and qualitative data via semi-structured interviews, which lasted approximately 60 minutes. Participants validated their responses, and educational guidance was provided.
Instruments
Data collection used a sociodemographic and clinical questionnaire, the Coronary Artery Disease Education Questionnaire Short Version (CADE-Q SV) 19 for disease knowledge, and the Eight-Item Health Literacy Assessment Tool (HLAT-8) 20 for health literacy. Semi-structured interviews addressed perceptions, difficulties, received guidance, and post-surgical follow-up.
Data Treatment and Analysis
Quantitative data were transcribed into Microsoft Excel 365®, verified, and exported to SPSS 20.0® and R for statistical analysis 21. Descriptive analysis included averages, medians, standard deviations, percentiles (25 % and 75 %) for quantitative variables, and absolute and relative frequencies for qualitative variables.
Then, quantitative data compliance, regarding normal distribution, was verified using the Shapiro-Wilk test to define the statistical approach. Variables with a normal distribution were submitted to the paired t-test, and those that did not present a normal distribution were submitted to the Wilcoxon test.
Comparison of the sociodemographic categories with CADE-Q SV and HLAT-8 scores was performed using the student's t-Test or one-way ANOVA, as appropriate. Tests were considered significant when p <0.05. For variables in which the ANOVA indicated statistical significance (specifically marital status in relation to CADE-Q SV), a post-hoc analysis was performed using Tukey's test. This analysis revealed a statistically significant difference between the "married" and "divorced" groups (p = 0.016), while the other comparisons did not reach statistical significance.
Qualitative data were analyzed through content analysis of statements 12: pre-analysis, coding, treatment of results and interpretation. In the first stage, statements were read and transcribed in full, then organized and transformed into text units for the corpus construction and insertion into the Interface de R Pourles Analyzes Multidimensionnelles de Textes et de Questionnaires (IRAMUTEQ_0.6-alpha3®) software.
In the second stage, the material was explored and codified. Statements were detached from the text into smaller categories, allowing us to identify the most relevant properties of the content. The categories identified were named using the software.
In the third stage of the qualitative analysis, the statements inserted in the software were interpreted and analyzed through similitude. The objective was to expand the meanings of the codes and themes found beyond initial representation. Data interpretation and understanding were based on the literature.
Through the elaboration of joint displays quantitative and qualitative data were integrated, aiming at an in-depth interpretation between the data from the two approaches. This strategy made it possible to identify divergences and convergences between quantitative and qualitative data.
Results
Quantitative phase
From the 24 participants, 75 % (n=18) were male. The average age was 59.6±6.6 years and 58.3 % (n=14) had studied for <9 years. The self-declared average family income was R$2,996.1 (US$599.2). The chronic disease that prevailed was hypertension (54 %; n=13), followed by diabetes mellitus (DM), associated with hypertension (21 %; n=5), as shown in Table 1.
Table 1 Sociodemographic and Clinical Characterization of Participants from the Western Paraná Mesoregion, Brazil, 2023 (n=24)
| Variable | ||
|---|---|---|
| Age - M±SD | 59.6±6.6 | |
| Per-Person Income - M±SD | R$2,996.1±2,707.4 | |
| Sex- n (%) | Female | 6 (25) |
| Male | 18 (75) | |
| Marital Status - n (%) | Single | 2 (8.3) |
| Married | 18 (75) | |
| Widowed | 1 (4.2) | |
| Divorced | 3 (12.5) | |
| Number of Children- n (%) | 1 to 3 | 14 (58.3) |
| More than 3 | 10 (41.7) | |
| Education - n (%) | <9 years | 14 (58.3) |
| >12 years | 4 (16.7) | |
| 9 to 12 years | 6 (25) | |
| Occupation - n (%) | Retired | 7 (29.2) |
| Paid activity | 7 (29.2) | |
| Sick pay | 7 (29.2) | |
| Unemployed | 2 (8.3) | |
| Housewife | 1 (4.1) | |
| Hypertension - n (%) | Yes | 18 (75) |
| No | 6 (25) | |
| Diabetes - n (%) | Yes | 7 (29.2) |
| No | 17 (70.8) | |
| Hypertension and Diabetes - n (%) | Hypertension and diabetes | 5 (20.8) |
| One of two | 15 (62.5) | |
| Neither | 4 (16.7) | |
| Smoking - n (%) | Yes | 9 (37.5) |
| No | 15 (62.5) | |
| Physical Activity - n (%) | Yes | 12 (50) |
| No | 12 (50) | |
| Medications - n (%) | Do not use | 6 (25) |
| 1 | 9 (37.5) | |
| 2 to 3 | 8 (33.3) | |
| 4 to 5 | 1 (4.2) | |
Source: Prepared by the authors.
The total HLAT-8 score was 18±6; 58.33 % of participants had unsatisfactory HL. Males had a lower mean HL (17±5) compared to females (21±8); however, there was no statistically significant difference between groups. Statistical significance was found when comparing knowledge of heart diseases and HL, and marital status (p-value 0.032; 0.014, respectively); divorced participants obtained higher averages on the scales. When comparing HL in terms of education, a lower average was observed among participants who had less than 9 years of education, with no statistically significant difference, as can be seen in Table 2.
Table 2 Comparison between the Participants Sociodemographic and Clinical Variables in Relation to HLAT-8 and CADE-Q SV Scores. West Paraná Mesoregion, Brazil, 2023. (n=24)
| Variable | HLAT-8 Mean (SD) | p-value* | CADE-Q SV Mean (SD) | p-value* |
|---|---|---|---|---|
| Total | 18 ± 6 | 36.1 ± 8.7 | ||
| Sex | ||||
| Female | 21 ± 8 | 0.185 | 35.5 ± 9.6 | 0.855 |
| Male | 17 ± 5 | 36.3 ± 8.7 | ||
| Marital Status | 0.032 | 0.014 | ||
| Single | 11 ± 6t | 28.5 ± 6.4 | ||
| Married | 17 ± 5 | 34.8 ± 7.6 | ||
| Widowed | 19 ± | 51 ± - | ||
| Divorced | 26 ± 5 | 44 ± 9.2 | ||
| Number of Children | 0.559 | 0.547 | ||
| 1 to 3 children | 17 ± 7 | 37.1 ± 8.6 | ||
| More than 3 children | 19 ± 3 | 34.8 ± 9.2 | ||
| Education | 0.185 | 0.522 | ||
| < 9 years | 17 ± 4 | 34.7 ± 9.3 | ||
| 9 to 12 years | 18 ± 9 | 36.5 ± 6.7 | ||
| > 12 years | 23 ± 6 | 40.5 ± 9.9 | ||
| Occupation | 0.323 | 0.769 | ||
| Retired | 15 ± 3 | 36.9 ± 12 | ||
| Paid work | 19 ± 8 | 38.6 ± 7.4 | ||
| On medical leave | 17 ± 6 | 34.3 ± 8.3 | ||
| Unemployed | 19 ± 4 | 36 ± - | ||
| Housewife | 28 ± -* | 27 ± -* |
Notes:*p-values obtained using Student's t-Test or ANOVA, depending on variable type. * Only one participant in this category. HLAT-8 = Eight-Item Health Literacy Assessment Tool; CADE-Q SV = Coronary Artery Disease Education Questionnaire Short Version.
Source: Prepared by the authors.
The average CADE-Q SV score was 36.13 ±8.7. As for CVD knowledge level, the acceptable classification prevailed (n=13; 54.17 %). Nonetheless, no statistically significant results were found when comparing sociodemographic variables with the results of HLAT-8 and CADE-Q SV.
Table 3 Questions and Domains Descriptive Statistics of the HLAT-8 of Participants Living in the Western Paraná Mesoregion, Brazil, 2023. (n=24)
| Domain | Mean/SD per Domain | H | Mean/SD per Question |
|---|---|---|---|
| UHI | 1.35 ±1.75 | H1 | 1.17 ±1.74 |
| H2 | 1.54 ±1.79 | ||
| SHI | 2.60 ±1.36 | H3 | 2.96 ± 1.12 |
| H4 | 2.25 ±1.51 | ||
| HI | 3.14 ±1.34 | H5 | 3.33 ±1.37 |
| H6 | 2.96 ±1.30 | ||
| CHL | 1.81 ±1.64 | H7 | 3.67 ±1.37 |
| H8 | 0.96 ±1.43 |
Notes: UHI= understanding health information; SHI= searching health information; HI= health interactivity; CHL= critical health literacy. Source: Prepared by the authors.
Analysis of the HLAT-8 revealed that participants had low HL § in the four domains. The highest scores occurred in SHI (2.60 ±1.36) and HI (3.14 ±1.34), related to search for information and communication in health. UHI domains (1.35 ±1.75) and CHL (1.81 ±1.64) had the lowest scores.
Regarding disease knowledge, results from the CADE-Q SV, presented in Table 4, indicate there was a statistically significant difference related to the knowledge about the disease when related to diet, clinical knowledge, and psychosocial risk, with p<0.001.
The application HLAT-8 highlighted that the questions with the lowest scores were related to the participants' understanding of health information and their ability to identify the quality of online health information (H1 and H8), as shown in Table 3.
Table 4 Descriptive Statistics of CADE-Q SV Scores by Area of Knowledge Regarding the Disease of Participants Residing in the Western Paraná Mesoregion, Brazil, 2023. (n=24)
| Knowledge Area | Average/SD per Area | P-value/area |
|---|---|---|
| Clinical Knowledge | 6.38±2.7 | <0.001 |
| Risk Factors | 4.88±1.73 | 0.279 |
| Physical Exercise | 7.5±2.65 | 0.624 |
| Diet | 11.75±4.33 | <0.001 |
| Psychosocial Risk | 5.38±2.5 | <0.001 |
Notes: SD - standard deviation. Source: Prepared by the authors.
Among the five knowledge areas, the participants scored the highest in Diet (average = 11.75, SD = 4.33) and the lowest in Risk Factors (average = 4.88, SD = 1.73), based on the descriptive statistics of the CADE-Q SV. These comparisons refer to the relative means among the five domains.
Qualitative Phase
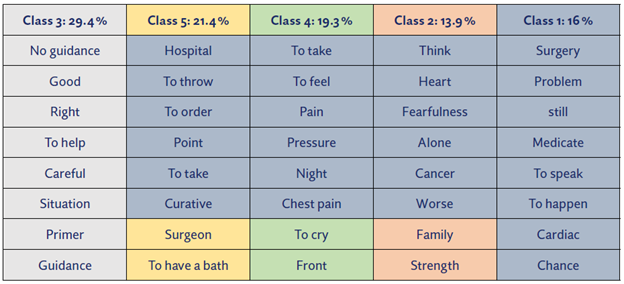
The qualitative phase included 24 interviews, with 90.23 % of the text analyzed using the Descending Hierarchical Classification technique (DHC) in the IRAMUTEQ®. The corpus was grouped into five lexical classes: Class 3 (29.4 %) informed the category (Mis)guidance and (mis)information related to care; Classes 5 (21.4 %) and 4 (19.3 %) supported Daily life transformed by the surgical procedure; and Classes 2 (13.9 %) and 1 (16 %) related to Feelings experienced during the surgical process and cardiac rehabilitation. The robust distribution of segments among these classes reflected and validated the thematic framework interpretive analysis.
Source: Prepared by the authors.
Figure 1 Phylogram Generated from the Descending Hierarchical Classification of Interviews with Participants Residing in the Western Paraná Mesoregion, Brazil, 2023. (n=24)
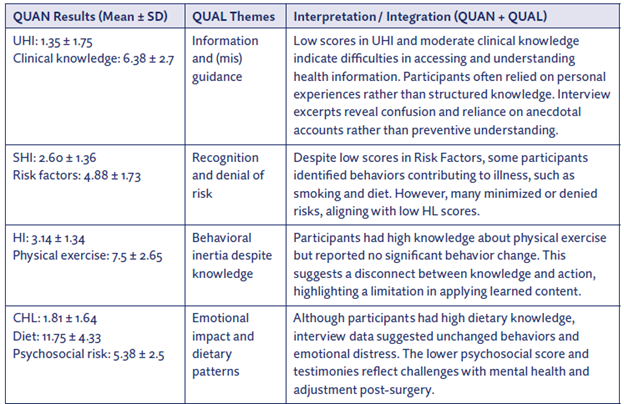
Figure 2 presents a combined representation of the QUAN + QUAL results, highlighting the areas of convergence and divergence between the CADE-Q SV and HLAT-8 scores and the participants' narratives. This integration allows for a deeper understanding of the health literacy and knowledge profiles of individuals undergoing CABG in the Western Paraná mesoregion.
For example, although the participants demonstrated reasonable clinical knowledge (average = 6.38), their low score in the IUS domain (average = 1.35) and their testimonies suggest that their health knowledge is based primarily on personal experiences rather than a formal understanding. Similarly, despite their recognition of behavioral causes of disease, the low score in Risk Factors (average = 4.88) suggests a limited understanding of disease prevention, which is reflected in ambivalent or contradictory attitudes, expressed in the interviews.
Divergence was also observed in the domains Physical Exercise and Diet: Participants presented high scores in these areas (average = 7.5 and 11.75, respectively), but reported maintaining unhealthy bey haviors after surgery. This points to a gap between knowledge and behavioral change. Finally, although knowledge about psychosocial risk was moderately good (average = 5.38), the emotional burden reported in the interviews reveals significant psychological challenges, reinforcing the importance of addressing emotional literacy in cardiac rehabilitation.
This joint presentation corroborates the dialogic nature of mixed methods research, highlighting how qualitative data can explain or contrast quantitative findings, enriching interpretation and providing insights into the complexity of health literacy and behavior.
Discussion
This study analyzed CAD knowledge and HL in individuals with infarction and late CABG, in which challenges in the rehabilitation process were identified through a mixed-methods approach. It can be highlighted for 1 using CADE-Q SV to assess disease knowledge in a South American population; 2 applying a mixed-methods design, as in Brawnwe et al. 22; and 3 integrating HLAT-8 and CADE-Q SV in a post-infarction and CABG population.
The results of this study indicated that participants had difficulties understanding health information since they had unsatisfactory levels of HL. These data corroborate the study conducted in Denmark with 15,728 people, with four out of 10 people reporting difficulties in accessing, understanding, and applying health information. From these, 8.18 % had inadequate HL and 30.94 % showed problematic HL levels 23.
The H L domains that scored the lowest in this study were related to understanding health information and critical literacy. Such results show difficulties in understanding disease care guidelines and health information, as well as interfering with the ability to select safe health information on the internet.
Our findings corroborate the results of a survey conducted with 1,700 Americans regarding information linked to social networks about COVID-19. The American study highlighted that people with limited HL had difficulties identifying the veracity of health information posted on media channels 24. While media platforms can disseminate information and educate people to take public health action, they can also lead to misinformation and misguidance 25.
Our study found no statistically significant difference between HL and CAD knowledge in relation to sociodemographic characteristics. In line with a study conducted with 76 participants, with acute coronary syndrome (ACS), in which 85.5 % obtained inadequate HL, regardless of their level of education 26. However, other authors agree that education levels and sociodemographic variables influence all dimensions of HL when associated with a higher prevalence of risks 27-28.
It is important to emphasize the conceptual differences between HL and health education; the first is a multidimensional concept, related to a set of skills and competencies, which can be developed through the second (education) 29. Therefore, social determinants tend to interfere with the development of fundamental skills necessary for HL, as they influence the health information used by patients 30-31.
As for CAD knowledge, in CADE-Q SV, despite participants having unsatisfactory HL, they had good knowledge about the disease. The areas with the most knowledge were Diet, Physical Exercise and Clinical Knowledge, with lesser knowledge regarding areas of Psychosocial Risk and Risk Factors 32.
These findings corroborate the results observed in the Persian validation of the CADE-Q SV from English to Farsi, where the highest and lowest scores of patients' knowledge were attributed to the areas of Nutrition and Psychosocial Risk, respectively 32, which were also evidenced in this study. Similar results were found when validating the CADE-SV for Brazilian Portuguese and French-Canadian. The area with the greatest knowledge was related to Risk Factors and Diet, with less knowledge on Psychosocial Risk 33.
However, this study partially diverges from these previous findings, suggesting that variations in knowledge levels across different domains may be influenced by cultural and lifestyle differences among populations 32.
HL in CAD influences outcomes through behavioral changes shaped by beliefs, perceptions, and sociocultural factors. A Chinese study found that greater disease knowledge was associated with lower adherence to healthy behaviors, while inadequate HL correlated with greater use of health services and acceptance of medical recommendations 34, thus diverging from the findings of this study.
Despite lower scores in the risk factors domain of the CADE-Q SV, participants recognized determinants of their illness but maintained unhealthy behaviors such as smoking, alcohol use, and sedentarism. These findings are consistent with studies showing adherence to pharmacological treatment despite persistent risk factors 35, and with evidence linking HL to physical activity, but not to smoking or alcohol consumption 36.
Proper management of lifestyle-related risk factors, which can be changed, requires people to gain some understanding of their disease. Thus, low HL and low health education are associated with a higher prevalence of risk factors 27. Therefore, a process centered on the person and their needs for cardiac rehabilitation, which considers the barriers and profiles of HL, becomes determinant for effectively targeting and providing services 36.
In a systematic review with meta-analysis, covering 17 studies conducted in 12 countries in five continents, it was observed that inadequate HL was highly prevalent in patients with CAD, while was associated with a higher risk of CVD, thus reinforcing significant changes in relation to the self-care of patients through educational interventions 37.
It should be noted that HL may be a consequence of AMI, which is a recurrent cause of hospital admissions; however, it is sensitive to interventions by primary services 38, which must be an interconnected network to provide comprehensive care.
The absence of communication and formal protocols between primary and specialized care leads to discontinuity after hospital discharge, making patients and families responsible for seeking information and managing care needs 39, results also found in this study.
Integrated data analysis highlighted the challenges experienced by participants in the late cardiac rehabilitation process. Most reported weaknesses in accessing health information and guidance during the recovery phase, in line with HLAT-8 data, in which participants had unsatisfactory HL. However, they were not usually seeking information or health guidelines and had difficulties understanding them. Furthermore, the information and guidance given at discharge had little impact on the rehabilitation process.
Finding health information and critically assessing health are decisive skills for those with multiple chronic illnesses since they need multiple sources of information to understand and cope with each of their illnesses 40. The difficulty in understanding health instructions can lead to a lack of self-confidence in the ability to practice self-care, constituting a detrimental factor for compliance with treatment 41.
Another important finding concerns participants' low knowledge of psychosocial risks, as it is known that CABG is a procedure full of feelings of doubt, fear, and uncertainty, before and after the surgical procedure. Stress was identified in participants' statements and CADE-Q SV as a risk factor for a cardiac event, being considered as important as DM and hypertension.
A recent study with 190 patients followed for three months after cardiac surgery identified that 14.7 % presented elevated levels of depression, anxiety, irritability, and dyspnea 42-44, which corroborates this study's findings. Nursing guidelines at discharge can reduce postoperative stress, as interaction with health professionals and family support positively influence care perception, clarify doubts, and promote self-care 45.
Conclusion
This study identified acceptable levels of CAD knowledge and unsatisfactory HL among individuals who underwent post-myocardial infarction and CABG. The primary challenge observed in the rehabilitation process was the difficulty in understanding professional healthcare guidelines necessary for lifestyle changes.
The integration of quantitative and qualitative data revealed important divergences between knowledge acquisition and health behaviors, highlighting barriers to effective self-care. Emotional challenges, limited understanding of risk factors, and discontinuities in care transitions further complicate the rehabilitation process.
These findings underscore the need for nursing interventions that assess HL and disease knowledge to design individualized educational strategies, aimed at promoting behavior change, preventing complications, and supporting long-term recovery. Incorporating HL assessment tools into the routine of nursing care is essential to optimize patient outcomes after cardiac surgery.

