











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
In 2017, there were 6.1 homicide victims per 100,000 population worldwide; the Americas had the highest rate with 17.2 1. In Colombia, according to the report of the Colombian Institute of Forensic Medicine for the year 2021, the homicide rate was 25.9 per 100,000 inhabitants 2. Over 25 years (1993-2018), the city of Cali, Colombia, recorded 45,819 homicides, an average of 1,762 per year (4.8 per day), while homicide rates declined from 102 to 47.8 per 100,000 inhabitants, reflecting a gradual annual reduction of 3.6% 3. Most homicides are focused on young people between the ages of 20 and 39 years, in the male population, 93.5% and with firearms AF 85% 3. The Hospital Universitario del Valle (HUV), the primary referral center within the public healthcare network of southwestern Colombia, receives the majority of trauma cases occurring in the city of Cali. In 2012, a total of 6,871 trauma patients were admitted to the HUV, of whom 31% (n= 2,142) were pediatric patients. Notably, 35% of the injury mechanisms in this population were associated with violence. 4. Some 5-year follow-up studies, before the Hospital Violence Interventional Program, report hospital readmission rates for violence of 44%-50% and death rates of 20%-25% 5.
According to other research, patients admitted with injuries from interpersonal violence are 80 times more likely to have a hospital re-admission for trauma than young people not exposed to previous trauma 6. In addition, hospital care for a second admission is 30% more costly than the first intervention 7.
To address this problem since 1993, Juvenile Violence Prevention programs have been developed in the U.S. and increasingly in level I Trauma Hospitals to reduce rates of readmission, death, psychoactive substances, hospital readmission and new criminal acts. The results of the research reported in the literature are variable, but with a tendency to decrease the rates of readmission and death due to new acts of violence 12-15.
Due to conditions of poverty, low schooling, unemployment, dysfunctional families, illegal cultures prone to violence, drug trafficking organizations and the presence of armed groups, an ecological public health approach is required to address youth violence 8. Hospital Violence Interventional Programs have become an alternative public health strategy to identify risk factors, protective factors and possibilities for prevention that begins in trauma hospitals where there is a unique opportunity, a “learning moment”, at the bedside of the patient in a critical situation, often close to death, to turn hospitalization into a turning point that manages to transform the cycle of violence 9-11.
Another impact generated by Hospital Violence Interventional Programs is a decrease in the rates of arrests by delinquent acts 16,17 and significant savings in overall costs due to a reduction in hospital admissions and court admissions 7,14,18,19.
Because of the conditions of urban violence existing in the territories where young people live (enemies, borders, confrontations, stray bullets, risk zones), the Transformed Circle of Violence Program, created in 2018 at HUV - Universidad del Valle, accompanies young people with strategies derived from the pedagogy of emergency and trauma. This methodology has been carried out for several years in international war and disaster scenarios to accompany children, adolescents, and young people 20.
The financing and sustainability of these hospital violence interventional programs is an ongoing challenge; the most stable programs with the best results are those that the hospitals finance and receive resources from various sources. The hope is that insurers will recognize the cost of these types of programs 21.
The objective of this study is to describe the results of the “Transforming the Circle of Violence Program Hospitalization an opportunity” initiative, which has been carried out in the HUV of Cali, Colombia, over a period of 5 years.
Materials and Methods
Between May 1, 2018, and June 30, 2023, a prospective descriptive cohort study was conducted within the registry of the Transforming the Circle of Violence Program. The study included survivors aged 13 to 29 years who were admitted to the Hospital Universitario del Valle “Evaristo García” (HUV) in Cali, Colombia, with traumatic injuries of external cause associated with violence. Data were obtained from pre-designed records completed by the interdisciplinary team and consolidated daily into an Excel database. A total of 290 young individuals were enrolled in the Transforming the Circle of Violence Program after providing informed consent.
Sociodemographic variables were collected, including Poverty Status, Unemployment or Underemployment, and School Dropouts. Poverty Status represents the socioeconomic condition of individuals or households whose income or available resources fall below an established poverty threshold, thereby restricting access to essential needs such as food, housing, healthcare, and education. Unemployment or Underemployment describes the condition of individuals who are either without paid employment and actively seeking work or employed in positions that do not fully utilize their skills, education, or available working hours. School Dropouts denote individuals who leave the formal education system before completing the legally required level of schooling or before obtaining the corresponding degree or certification. The measurement of variables was conducted through a clinical interview.
Location
The study was conducted at the Hospital Universitario del Valle in the city of Cali, Colombia. This is a highly complex public hospital with 500 beds, 80 of them intensive care beds, and coverage for the southwestern part of Colombia. According to the institutional trauma registry, during the year 2020, about 4,500 trauma patients were admitted to this institution per year, 37.3% (n= 1,680) of them for penetrating trauma.
Patients
Young people between 13 and 30 years of age who signed the informed consent to enter the Transforming the Circle of Violence Program were included. Patients with suicide attempts, domestic violence, problematic consumption of psychoactive substances, street dwellers, young people living outside the program's area of coverage or those who refused accompaniment were excluded.
Work team and registration
The Transforming the Circle of Violence Program has an interdisciplinary team made up of a General Coordinator (specialist in Trauma and Emergency Surgery), an Administrative Coordinator, an administrative secretary, a psychologist, a social worker, 4 Community Social Managers, four specialists in Emergency Pedagogy and a specialist in Spiritual Care. In addition, the young people and their families are accompanied by a team of Family Medicine and final year psychology and social work students from the universities who do internships at the HUV.
Steps that make up the program
The young people who enter the program are accompanied in the following areas:
Physical recovery. Upon discharge, we seek to guarantee the right to health and physical recovery, accompanying them in the administrative and assistance processes with insurance companies and hospitals.
Emotional recovery. Accompaniment by psychology, art therapy and Emergency Pedagogy in individual and family outpatient consultations.
Family accompaniment. The development of healthy family relationships is sought through social work visits to homes and outpatient consultations.
Life project. Accompanying young people to develop educational, sports, employability, or economic projects that enable them to create healthy life projects.
Development of non-violent social skills. Through meetings of young people and activities of Pedagogy of Emergencies, we build with them non-violent ways of relating to each other.
Helping others. At the end of the accompaniment process, the young people give back what they have received by helping other young people or people in vulnerable conditions.
Analysis
Based on the Institutional Trauma Registry, data were prospectively entered into an Excel® database and analyzed using R statistical software 22. Means and standard deviations were calculated for continuous variables, and proportions for categorical variables. A p-value <0.05 was considered statistically significant. Specifically, Fisher’s exact test was used to compare categorical variables before and after the implementation of the program.
Results
Demographic and psychosocial characterization
During the period analyzed, 1,700 young candidates were admitted to the Program, of these, 954 (56%) were accompanied during their hospitalization period, and 290 (30%) met the criteria for the Program and were accompanied at hospital discharge by the multidisciplinary team of the Transforming the Circle of Violence Program for an average time of 10 months. The three main reasons for not being accompanied were: living outside the coverage area (20%), loss of contact (18%) and not being interested in the program (13%) (Figure 1).
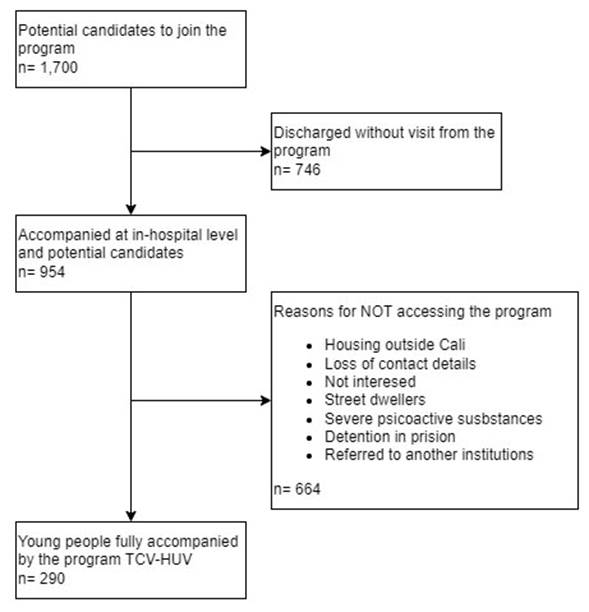
Figure 1 Flowchart of young people who eventually enter the Transforming the Circle of Violence (TCV)- Hospital Universitario del Valle (HUV) program.
The Transforming the Circle of Violence registry has information on 290 subjects, with an average age of 20 ±3.8 years, 20% are minors, and 93% are male. Eighty-four percent come from the city of Cali, mainly from the poorest communes located in the eastern and hillside areas of Cali. Table 1 presents sociodemographic information.
Table 1 Demographic characteristics
| Transforming the Circle of Violence - HUV Program. N: 290 youths | |
|---|---|
| Variable | n (%) |
| Age 20 years (13-30) | |
| >14 | 3 (1) |
| 14-18 | 64 (22) |
| 19-25 | 180 (62) |
| 26-30 | 43 (15) |
| Sex | |
| Men | 270 (93) |
| Famele | 20 (7) |
| Place of origin | |
| Cali | 76% |
| Other | 24% |
| Socioeconomic level | |
| 0 | 2% |
| 1 | 55% |
| 2 | 34% |
| 3 | 7% |
| 4 | 1% |
| 5 | 0% |
| 6 | 0% |
| Poverty status | 98% |
| Unemployment or underemployment | 77% |
| School Dropouts | 60% |
The mechanism of injury
The injuries were caused by firearm (FA) 51%, sharp weapon (SHW) 35%, blunt weapon (BLW) 9% and others 5%. Approximately 20% of the youths accompanied were left withdisabilities, mainly paraplegia, monoplegia, and ocular loss. The average hospitalization time was 11 ± 8.7 days. The youth identified the cause of the injury as: quarrel 32%, invisible borders between gangs 27% and revenge in 20%.
Economic status and education
Ninety percent belong to low-income strata 1 and 2; 98% live in poverty and 87% work in the informal sector or are unemployed. Before the program, 60% of the young people reported dropping out of school, 30% only had primary school, 21% had a high school degree, and only 5% had some higher education.
Family composition
The predominant family composition is single parent with a female head in 53% of the cases; the predominant family relationships are conflictive in 71%; the predominant communication is aggressive in 75%; the parenting style is permissive in 79% and affective ties with the young person are scarce in 77% of the families. There are repeated transgenerational patterns such as parental abandonment 30%, psychoactive sustance consumption 25% and urban violence 17%.
Psychological evaluation
The traumatic events that the patient identifies as key in his life are an unprocessed mourning for the death of a close relative 30%, abandonment by a parent 30% and separation from their parents 22%. Although very few patients have post-traumatic stress disorder, most of them present some of its symptoms (hypervigilance or hyperactivity 57%, intrusive memories 35%, cognitive and mood symptoms 16% and avoidance symptoms 12%). The predominant affective symptoms are anger (30%), difficulties in expressing feelings (23%), sadness (15%), and apathy (11%) (Tables 2 and 3).
Table 2 Family diagnosis
| Transforming the Circle of Violence - HUV Program. N: 290 youths | |
|---|---|
| Variable | n (%) |
| Family composition | |
| Single parent famele | 154 (53) |
| Nuclear | 52 (18) |
| Extensive | 35 (12) |
| Young woman with a partner | 14 (5) |
| Another | 35 (12) |
| Family relationships | |
| Conflicting | 103 (36) |
| Close and conflictive | 73 (25) |
| Nearby | 46 (16) |
| Very narrow and conflictive | 29 (10) |
| Distant | 26 (9) |
| Very narrow | 12 (4) |
| Types of communication | |
| Aggressive | 218 (75) |
| Crusher | 46 (16) |
| Assertive | 26 (9) |
| Parenting style | |
| Permissive | 229 (79) |
| Negligent | 29 (10) |
| Positive parental | 17 (6) |
| Others | 14 (5) |
| Family displacement by violence | 20% |
Table 3 Psychological characteristics
| Transforming the Circle of Violence - HUV Program. N: 290 youths | ||
|---|---|---|
| Variable | n (%) | |
| Cause injury | ||
| Quarrels | 93 (32) | |
| Invisible boundaries: Territoriality/Violence/Street Gangs | 78 (27) | |
| Revenge | 58 (20) | |
| Theft | 35 (12) | |
| Other | 26 (9) | |
| Post-traumatic stress disorder symptoms | ||
| Hypervigilance or Hyperactivity | 165(57) | |
| Intrusive memories | 101(35) | |
| Cognitive or mood Symptoms | 46(16) | |
| Avoidance Symptoms | 35(12) | |
| Affective Symptoms | ||
| Anger | 87(30) | |
| Sadness | 44(15) | |
| Apathy | 32(11) | |
| Frustration | 22(7) | |
| Anxiety | 20(7) | |
| Emptiness | 14(5) | |
| Others | 41(14) | |
| No data | 41(14) | |
| Psychoactive substance consumption | 131(66) | |
| Psychiatric disease | 12(4) | |
| Transgenerational patterns * | 179 (62) | |
| Violence | -17% | |
| Father abandonment | -30% | |
| Family history of psychoactive sustance consumption | -25% | |
| all | -16% | |
* Parents of youths with a personal history of violence
Background
Forty percent of the youths had been injured by penetrating trauma because of interpersonal violence before this admission to the hospital. On the other hand, 21% of the youths had been arrested, 26% belonged to a gang, and 14% to a criminal gang. Within the family background, 20% of the families had been displaced by violence, mainly from the Colombian Pacific coast.
Effects of the program on the young people who join
Accompanying time
The average time of accompaniment was 10 ±8.7 months, of which 28% lasted more than one year and 60% more than 6 months. Of the young people who entered the program, 10% were released due to recidivism.
Physical, social and emotional recovery
The following is a description of before and after the Transforming the Circle of Violence Program: they complete their physical recovery process from 60% to 82%, receive family and psycho-pedagogical support from 0% to 94%, spiritual support from 0% to 30%, health insurance and identity card from 60% to 100%; school integration went from 35% to 75% and integration to higher education from 5% to 20%.
Job placement
The number of young people who found formal or informal employment increased from 23% before the program to 40% after the program. Of these, five young people from the program have been linked to the HUV.
Re-entry and death due to new acts of violence
According to our data and those reported in the literature, the rate of hospital readmission decreased from 40% to 10%, and deaths due to violence from 20% to 3% for the years 2019 and 2023, respectively. These figures correspond to historical (before-after) comparisons within the same cohort. (Table 4).
Table 4 Program Achievements Transforming the Circle of Violence*
| Variable | Before (%) | After (%) |
|---|---|---|
| Physical recovery is completed | 60 | 99 |
| Psychological Accompaniment | 0 | 40 |
| Family Accompaniment | 0 | 80 |
| Emergency pedagogy | 0 | 100 |
| Restoration of rights | 60 | 100 |
| School linkage | 35 | 75 |
| Access to higher education | 4 | 20 |
| Criminal activities | 50 | 10 |
| Reentry by violence | 40* | 10 |
| Death by violence | 20** | 3 |
*Date are extracted from the prospective follow-up registry of the 290 young people included in the study.
**Mortality data from the literature. Purtle et al. Hospital-based violence intervention programs save lives and money. J Trauma Acute Care Surg Volume 75, Number 2
Transforming the Circle of Violence Program Funding
The resources for the financing of the Transforming the Circle of Violence program come from the HUV 60%, donations 30% and resources from the universities of the region 10%; however, what has allowed it to survive during these 5 years is that the HUV has identified that the care of psychosocial wounds is as important as the care of physical wounds.
Discussion
Youth violence is a public health problem in the world; its manifestation in Latin America and in the city of Cali reaches epidemic levels. As in the Hospital Violence Interventional Programs in the US, the HUV addresses youth violence as apublic health problem. Additionally, for the injured youth, hospitalization is a unique opportunity, a "learning moment"that can become a turning point to transform the circle of violence 9. United Nations UNDOC records show that criminal activity in the world produces 4 times more deaths than wars and terrorist violence 1.
The program's records show a significant decrease in the number of young people who relapse into delinquent activities from 50% to 10%; it is important to note that this percentage has been maintained during the 5 years of the program. Most of the young people admitted to the hospitals for interpersonal violence have very low schooling or a history of having dropped out of school; there is evidence that shows that schooling is a risk factor for criminal activities. In addition, a study shows that not only the level of education but also the quality of education can reduce the rates of criminal activity by up to 50% 23,24.
Among young people who enter the HUV injured, 60% drop out of school, 71% fail to complete high school, and fewer than 5% pursue higher education. The Transforming the Circle of Violence - HUV Program has developed its own school leveling project, enabling 75% of young people to complete high school and 20% to access higher technical education. A component of both our baccalaureate curriculum and the intra and extra-hospital accompaniment is carried out using the tools of the Pedagogy of Emergencies 20. This methodology, created by the pedagogue Bernd Ruff, uses elements of Waldorf Pedagogy 25 to accompany adolescent children and young people in contexts of war conflicts and natural disasters. In this sense, as far as we know, this is the first Hospital Violence Interventional Program in the world to use Emergency and Trauma Pedagogy as part of the accompaniment. Although we are convinced of the benefits of this methodology, its results can only be evaluated in the coming years.
Adversity in childhood and the family environment are clearly identified risk factors, even more critical than violent community contexts and relationships with delinquent peers 26,27. In the family assessment of the young people, the following risk factors were identified: displacement due to violence 20%, transgenerational violence and family composition with an absent father in more than 50% of the families; conflictive family relationships, permissive parenting models and aggressive types of communication in about 80% of the families. During the accompaniment, 88% of the families of the young people have received accompaniment at home and in workshops to strengthen positive family bonds that allow them to transform family life.
Some studies have identified a wide range of psychological sequelae in young people admitted to hospitals, with rates of Post-traumatic stress disorder ranging from 25% to 80% 28,29. Although post-traumatic stress disorder manifests months or years after the traumatic event, in the present series, the majority manifested at least one symptom, mainly hypervigilance and hyperactivity in 57% and intrusive memories in 35% and additionally affective symptoms such as anger, sadness or apathy, among others.
The presence of Psychoactive substance consumption is a risk factor for youth violence. However, the Transforming the Circle of Violence - HUV Program does not link and refers to specialized services for treatment of those patients withproblematic consumptionof Psychoactive substance (when consumption affects health, family relationships and friends; or when it alters daily activities such as work or study or involves economic problems). The consumption of PS by young people in the program is high at 66%. In addition to the health problems associated with PS consumption, it is related to the risk of violence linked to theft and drug trafficking, which is the most frequent crime committed by adolescents 30. To accompany psychological symptoms and PS consumption, the Transforming the Circle of Violence - HUV Program team uses psychological tools such as grief management, emotional intelligence, self-care, social skills development and art therapy in individual and family consultations, group therapies and workshops.
Based on the literature and our own data, before the Program, hospital readmission rates vary between 40% and 50% and 20% and 25% and death rates due to new violence in the following 5 years 5. Our data indicate that for the group of patients admitted and accompanied by the Transforming the Circle of Violence - HUV program, the readmission and death rates within the first 5 years of the program were 10% and 3%, respectively. These results are similar to those reported for the Hospital Violence Interventional Programs in the USA 13-16.
Conclusions
This is the first Hospital Violence Interventional Program in Colombia, the second in Latin America and the first program in the world to introduce Emergency and Trauma Pedagogy for the comprehensive care of young people admitted for traumatic injuries of violent origin. Our data show that these types of programs decrease hospital readmission rates, death due to violence and recidivism in criminal activities. More hospitals in Colombia, Latin America and the world should replicate this type of program.

