











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Actinomycosis is a chronic bacterial infection caused by branched gram-positive bacilli of the order Actinomycetales, family Actinomycetaceae, and genus Actinomyces. The main species responsible for actinomycosis in humans is Actinomyces israelii; however, Actinomyces georgiae, a less common species, was identified in this case. Forty-nine species have been described within this genus, of which 26 are associated with human disease, although many are part of the normal commensal microbiota 1,2.
Extensive cohort studies, including those involving up to 650 cases, have consistently shown that Actinomyces infections are polymicrobial. However, isolating Actinomyces as the sole pathogen, as in our case, is a unique and impressive feat that highlights the novelty of this presentation 3.
The disease occurs when the mucosal barrier is breached, allowing bacteria to invade deep tissues. Its progression is characterized by granulomatous tissue formation, extensive reactive fibrosis and necrosis, and the development of abscesses, fistulous tracts, and sinus drainage 4,5. Actinomycosis is a rare condition with a global distribution and no apparent predilection for age, race, season, or occupation. However, it is more frequent in men, with an incidence of approximately 0.3 cases per million population 1,6. Major risk factors include diabetes mellitus, immunosuppression, malnutrition, and previous tissue injury 2.
Clinical manifestations of actinomycosis may include a slow-growing, initially painless, indurated mass that progresses to abscess formation, fistulous tracts, and purulent drainage 5. This report presents the case of a patient with abdominal actinomycosis, whose clinical presentation, surprisingly, simulated a malignant neoplasm, manifesting as a painful mass adherent to multiple organs, with colo-cutaneous fistula and suppuration.
Case presentation
We present the case of a 77-year-old male patient who was admitted to the institution for three months because of an abdominal mass growth in the epigastrium. He also reported subjective fever, nocturnal diaphoresis, and unquantified weight loss. At the time of admission, the patient was asymptomatic regarding nausea and emesis.
Physical examination revealed an indurated mass approximately 10 x 7 cm, located in the epigastrium, in the subcutaneous plane, with a stony consistency, irregular borders, painful to palpation, and a 4 cm central phlyctenae spontaneously secreting purulent material, which was sent for culture, which was negative. In addition, hepatomegaly was palpable, with no signs of peritoneal irritation. No signs of acanthosis nigricans or other cutaneous manifestations associated with diabetes were observed. The patient's medical history included non-insulin-requiring diabetes mellitus, arterial hypertension, dyslipidemia, and a surgical history of phakectomy and traumatic amputation of the left toes. The patient had been a former smoker for 20 years, and his usual treatment included Sitagliptin/Metformin 50/1,000 mg once daily, Losartan 50 mg once daily, Amlodipine 5 mg once daily, Atorvastatin 40 mg once daily, and ASA 100 mg once daily.
Initial studies included a computed tomography (CT) scan of the abdomen (Figure 1), which showed focal thickening of the transverse colon accompanied by an ill-defined inflammatory lesion extending towards the abdominal wall and a collection suggestive of a colo-cutaneous fistula. This raised the suspicion of a neoplastic process. The contrasted thoracic CT scan showed no alterations. Relevant laboratory tests are presented in Table 1. Helicobacter pylori testing was not performed at the time of admission.
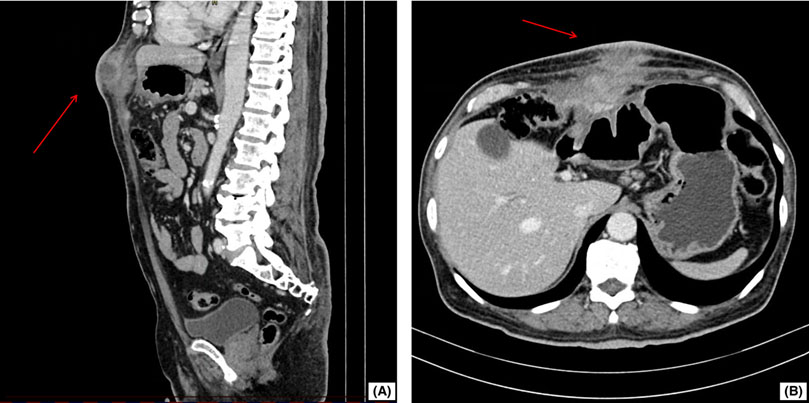
Figure 1 Abdominal CT Scan in Sagittal and Axial Views. (A) Sagittal View of the Abdomen: The imaging reveals a clear and distinct heterogeneous-density soft tissue mass (marked with a red arrow) in the abdominal wall extending toward the cutaneous surface. (B) Axial View of the Abdomen: A soft tissue mass (red arrow) adherent to visceral structures is visualized and consistent with multiorgan adhesions.
Table 1 Relevant Clinical Laboratory Test Results
| Parameter | Result | Reference Values |
|---|---|---|
| Hemoglobin | 9.9 | 12-17.5 g/dL |
| Hematocrit | 29.4 | 36-50 % |
| Mean Corpuscular Volume | 67.4 | 80-100 fL |
| Mean Corpuscular Hemoglobin | 22.7 | 27-33 pg |
| Leukocytes | 11.938 | 4.500-11.000 /µL |
| Neutrophils | 9.013 | 1.800-7.700 /µL |
| Carcinoembryonic Antigen | 1.7 | 0-5 ng/mL |
| Serum Iron | 110 | 60-170 µg/dL |
| Glucose | 137 | 70-140 mg/dL |
| Aerobic culture | Actinomyces shaaliae georgiae |
Suspecting an infectious process, treatment was started with ciprofloxacin 400 mg IV every 12 hours and metronidazole 500 mg IV every 8 hours, in addition to performing a 5 cc ultrasound-guided drainage. The aerobic microbiological culture was positive for Actinomyces shaaliiae georgiae, which increased the suspicion of an infectious process associated with a neoplastic process. Despite antibiotic treatment, the patient continued to present symptoms, and a colonoscopy was performed. However, the findings were inconclusive, with no evidence of significant alterations. Therefore, an exploratory laparotomy was performed. During surgery, a stony mass was found firmly adhered to the abdominal wall, stomach, colon, and liver, with purulent material coming out. Surgical resection of the mass was performed, including subtotal gastrectomy, left hepatic lobectomy, resection of the mesentery, and left hemicolectomy, and a temporary colostomy was left.
Histopathological (Figure 2) study of the specimens obtained ruled out a neoplastic process and confirmed the presence of an infectious process by Actinomyces Shaaliae georgiae. Postoperatively, the patient developed respiratory and hemodynamic complications. Subsegmental pulmonary thromboembolism was diagnosed by Angio tomography, and treatment with low molecular weight heparin was initiated. However, the patient had an unfavorable evolution, developing cardiorespiratory arrest, which resulted in his death.
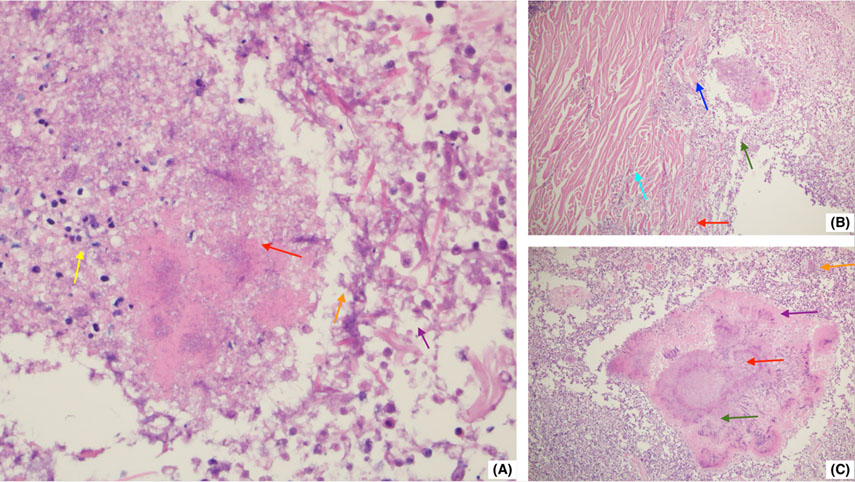
Figure 2 Histopathological findings of abdominal actinomycosis showing sulfur granules and suppurative inflammation.
(A): Areas of Necrosis and Inflammatory Response (H&E, x400)
(Red arrow): Coagulative necrosis: An extensive necrosis area with cellular architecture loss. The cytoplasm appears intensely eosinophilic, and nuclei are absent. The presence of sulfur granules and dense basophilic aggregates of filamentous Actinomyces bacteria surrounded by an eosinophilic Splendore-Hoeppli reaction is noted.
(Yellow arrow): Inflammatory infiltrate of polymorphonuclear cells (PMNs) dispersed around the necrosis.
(Orange arrow): Fibrillar material and eosinophilic cellular debris, with fragmented cells undergoing karyolysis and pyknosis.
(Purple arrow): Microabscesses containing cellular debris, with focal accumulations of inflammatory cells forming microabscesses.
(B): Transition Zone (H&E, x200)
(Blue arrow): Muscular degeneration and atrophy: Clear distinction between preserved striated muscle and inflamed tissue. The actinomycotic colonies are embedded within the fibrotic stroma.
(Cyan arrow): Perimuscular fibrosis: Proliferation of fibroblasts and collagen deposition, indicating chronicity.
(Green arrow): Perivascular granulomatous inflammation: Inflammatory infiltrate primarily composed of macrophages and epithelioid cells.
(Red arrow): Reactive neovascularization: Development of small blood vessels at the edges of inflammation.
(C): Sulfur Granules and Chronic Inflammatory Reaction (H&E, x400)
(Red arrow): Bacterial colony (sulfur granule): Basophilic center surrounded by an eosinophilic periphery. Sulfur granules are pathognomonic findings for actinomycosis.
(Green arrow): Foamy histiocytes and epithelioid cells: Activated macrophages with granular cytoplasm.
(Purple arrow): Multinucleated giant cells: Chronic granulomatous response featuring multinucleated cells.
(Orange arrow): Lymphoplasmacytic inflammatory reaction: Dense infiltrate of lymphocytes and plasma cells at the lesion's periphery.
Informed consent
Informed consent was obtained or waived for treatment and open-access publication from all participants in this study. Additionally, informed consent was obtained from those involved. The Research and Ethics Committee issued approval 1115875. We hereby report that on October 3, 2024, as recorded in Act 19/2024, the Hospital Research and Ethics Committee approved the review of the aforementioned clinical history for the purpose of preparing a case report.
Discussion
This case presents a unique diagnostic challenge where actinomycosis mimicked malignancy, requiring careful evaluation of our diagnostic approach and differential diagnosis. Our patient's presentation with a painful, indurated epigastric mass with cutaneous involvement and constitutional symptoms strongly suggested neoplasia, particularly given the CT findings of a heterogeneous mass with multiorgan adhesions.
Regarding our diagnostic workup, we followed established protocols for suspected abdominal masses. The CT imaging showed characteristic findings that could be consistent with either infectious or neoplastic processes 7. Computed tomography findings in actinomycosis include the formation of abdominopelvic abscesses, bowel wall thickening, inflammatory infiltration of the pericolic fat, and mass lesions, which can mimic neoplastic processes 8. The diagnosis frequently requires biopsy and histopathological identification of the organism 9, as well as microbiological studies to confirm the presence of Actinomyces spp. For Helicobacter pylori detection specifically, tissue biopsy and biochemical tests on bacteria isolated from biopsy samples have shown superior diagnostic accuracy compared to other methods 10. The positive aerobic culture for A. shaaliae georgiae was crucial, though this initially increased rather than decreased our suspicion of malignancy, as co-infection with neoplasms has been reported 11.
The differential diagnosis in this case should have included several conditions beyond malignancy. Tuberculosis could present similarly with chronic constitutional symptoms, mass lesions, and fistula formation. Other considerations should consist of Crohn's disease with complications, other granulomatous diseases, inflammatory bowel disease with perforation, and chronic infections such as nocardiosis or cryptococcosis. The clinical features of abdominal actinomycosis, as described in previous case series, can closely mimic those of other conditions, making diagnosis challenging 11. Antibiotics are usually added to culture media to inhibit the growth of normal flora, which may explain why A. shaalae georgiae was isolated as the sole pathogen.
Our patient's diabetes mellitus was likely a contributing factor, as it represents a known risk factor for actinomycosis 12. The causative pathogen, a gram-positive, spore-forming bacterium that is a regular part of the human microbiota, most commonly Actinomyces israelii, can become pathogenic when conditions favor invasion 2. Sometimes the bacilli are arranged in a filamentous form. Various risk factors have been associated with this infection, most notably direct inoculation via abdominal surgery or colonization of intrauterine devices, particularly in cases of bladder infections 12. The cervicofacial region is the most common location for actinomycosis, with abdominopelvic cases comprising only about 20% of all instances 7. A study on appendicular actinomycosis revealed an incidence of only 0.23% among patients who underwent appendectomy 13.
The polymicrobial nature of most actinomycosis cases makes our finding particularly noteworthy 3. In most cases, Actinomyces does not appear in isolation; instead, it is typically accompanied by other microorganisms. Therefore, its exclusive identification in a lesion is uncommon. The identification of Actinomyces species in this case was performed using conventional microbiological methods and biochemical tests; thus, PCR methods were not employed, and primer sequences and electrophoresis images are not available. Furthermore, a thorough literature review found no previous reports describing Actinomyces schaalii georgiae as the sole cause of this particular presentation, without the presence of other microbial agents.
The surgical approach was justified given the extensive multiorgan involvement and the failure of medical management 9,12. The aggressive nature of this infection, as demonstrated by the histopathological findings including tissue invasion, fibrosis, and chronic inflammation, required radical surgical intervention. The management of actinomycosis typically requires a multidisciplinary approach based on source control and prolonged antibiotic therapy 2,12. Clinical experience from single-institution studies demonstrates that surgical management is often reserved for those who fail medical treatment or develop complications 9.
This case illustrates that actinomycosis must be included in the differential diagnosis of tumoral disease, as it could alter the patient's workup and reduce delays in diagnosis 11. The atypical presentation, characterized by a painful suppurative mass and extensive organ infiltration, combined with the isolation of A. shaaliae georgiae as the sole pathogen, makes this case particularly valuable for the medical literature. The spectrum of imaging findings and common mimickers of abdominopelvic actinomycosis emphasizes the diagnostic challenge presented by this condition 8.
Conclusion
To our knowledge, this case represents an uncommon presentation of Actinomyces shaaliae georgiae as a sole pathogen causing abdominal actinomycosis with colo-cutaneous fistula and multiorgan adhesions mimicking malignancy. The case contributes to the medical literature by: (1) expanding the clinical spectrum of A. shaaliae georgiae infections, (2) demonstrating that actinomycosis can present as an isolated pathogen rather than in its typical polymicrobial nature, and (3) highlighting the diagnostic challenge when infectious processes closely mimic neoplastic disease. This report emphasizes the importance of maintaining high clinical suspicion for actinomycosis in patients with chronic abdominal masses, particularly in the presence of risk factors such as diabetes mellitus.

