











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Healthcare decisional capacity refers to the ability to make decisions regarding one's own health, including the consent to or refusal of treatments and procedures (Albuquerque 2021). In countries with an Anglo-Saxon legal tradition, this capacity is considered an application of what has conventionally been termed mental capacity or mental competence, and it refers to a set of abilities that include understanding, appreciation, reasoning, and expression of choice concerning a given diagnostic or therapeutic proposal (Appelbaum and Grisso 1988; Michaud et al. 2015; Barstow et al. 2018). This set of abilities, under the framework of Clinical Bioethics grounded in human rights, holds contextual relevance insofar as it constitutes the key to the exercise of personal autonomy from a philosophical perspective, and to the human right to respect for private life from a legal standpoint (Albuquerque 2015). For instance, consider a sixteen-year-old adolescent diagnosed with iron-deficiency anemia, whose underlying cause has already been investigated. The medical team proposes initiating treatment with oral iron supplementation, which is associated with mild and manageable gastrointestinal side effects. After receiving information aligned with her concerns, including the proposed treatment, its risks, benefits, and alternatives, the patient demonstrates understanding of the diagnosis (understanding), recognizes that anemia impacts her health and quality of life (appreciation), weighs the advantages and disadvantages of the medication (reasoning), and consistently expresses her decision to initiate treatment (expression of choice). In this case, the assessment of decisional capacity indicates that she is able to exercise her right to consent to the therapeutic proposal. Comparable situations may involve the refusal of treatments and procedures, in which adolescents must demonstrate the same abilities required to exercise this right as those demanded for the right to consent (Martins et al. 2025a). When an adolescent's healthcare decisional capacity is uncertain, it should be evaluated using the best available scientific evidence. As adolescents gain knowledge, accumulate experiences, and deepen their understanding, the role of the healthcare team and legal guardians can gradually shift, from providing direction, reminders, and advice toward engaging in a more balanced exchange of perspectives (World Health Organization 2021).
The human right to respect for privacy encompasses an individual's prerogative to live their life without interference in their body or personal choices (Albuquerque 2015). This right is grounded both theoretically and normatively in the United Nations Convention on the Rights of the Child (CRC), adopted in 1989 (United Nations 1989). Article 16 establishes the right to privacy, stipulating that arbitrary or unlawful interference in a child's private life must not occur (United Nations 1989; Eler and Albuquerque 2019). This right applies to adolescent health care with the same fundamental scope as in adult health care, although the extent of its application may vary (Tobin and Field 2019). The extent of this right is primarily determined by the developmental capacities of the adolescent patient (Tobin and Field 2019). The concept of evolving capacities refers to the understanding that an adolescent's overall development occurs gradually as their skills and competencies progress, and that age alone is not the sole determinant for the personal exercise of their rights (United Nations 1989; Eler 2022). From this perspective, the exercise of the patient's right to confidentiality, right to self-determination, and right to bodily integrity, all resulting from the human right to respect for private life, is closely linked, to varying degrees, to the adolescent patient's decisional capacity in healthcare, which advances progressively over time (Tobin and Field 2019). Within this same decisional context, it is important to recognize that vulnerability is a universal condition inherent to the human experience. Adolescents, however, present heightened vulnerability, characterized by an ontological fragility that limits their ability to protect themselves or respond appropriately to situations that pose a risk or cause actual harm. This condition increases the likelihood of physical or emotional injury, particularly in light of their ongoing developmental process (Herring 2016; Boldt 2019; Herring 2023). Evolutionary capacities and heightened vulnerability are interrelated, as both acknowledge adolescent development as a dynamic and individualized process, highlighting the need for additional protection against the physical and emotional fragilities intrinsic to this stage of life.
Respect for privacy, acknowledgment of evolving capacities, and consideration of heightened vulnerability in the adolescent decision-making process coexist in a continuous and interdependent state. Each represents an equally significant biological, ethical, and legal foundation. This interaction creates a dynamic equilibrium, referred to in this article as an "interface," in which no single dimension can be fully considered in isolation without influencing the others. The inherent complexity of this interplay requires that assessments of healthcare decisional capacity be grounded in robust scientific evidence, with clear criteria sensitive to the specific characteristics of adolescent patients. From the perspective of technical assessment instruments, academic undertakings have been occasionally found to be precisely insufficient, in the same sense as the timid discussions on the role of the assessor throughout this specific and complex process (Koelch et al. 2010; Dunne 2019; Miquel et al. 2019; Boceta et al. 2021; Cardona Isaza et al. 2021; Baltag et al. 2022). The assessor of the adolescent's healthcare decisional capacity is the one who operationalizes, in practice, the technical assessment of the adolescent's skills, with issues related to their profile and the assessment approach deserving attention in academic discussions. Therefore, aiming to fill this gap in the scientific debate, this article seeks to expand bioethical discussions on the skills and responsibilities involved of the evaluator in assessing adolescent healthcare decisional capacity.
Methods
A theoretical-documentary study was conducted grounded on the United Nations Convention on the Rights of the Child and incorporating bioethical perspectives outlined in Healthcare Bioethics, a branch of Clinical Bioethics developed in Brazil, which rests on a tripod of Patient-Centered Care, Shared Decision-Making, and Patients' Rights (United Nations 1989; Bowen 2009; Morgan 2021; Albuquerque and Tanure 2023; Albuquerque 2023a; Albuquerque and Eler 2025). Sources analyzed included books, academic articles, white papers, and guidelines from recognized governmental and non-governmental organizations in the field of safe and high-quality healthcare. Authenticity, credibility, representativeness, and significance were employed as scientific criteria for selecting documents (Flick 2023). Theoretical purposive sampling was applied across the entire document sample (Bowen 2009). Saturation was considered reached when additional searches no longer provided new information after multiple cycles of data collection (Merriam and Tisdell 2016). The data obtained through this research, comprising both primary data collected via qualitative and quantitative methods, and secondary data gathered through theoretical studies and literature reviews, were systematically analyzed. The initial proposal for data triangulation was limited due to the low occurrence of studies that allow such a methodological proposal (Bowen 2009). Only studies with clearly defined research practices, aligned with the standards of scientific integrity recognized by the international academic community, were included (All European Academies 2023).
Once the database had been compiled, a reflective thematic analysis was conducted, incorporating the researcher's subjectivity as a legitimate scientific resource in the interpretation of findings through the lenses of clinical bioethics and human rights (Morgan 2021). To examine the documents and their contents, a phenomenological epistemological approach was adopted, allowing for both objective and subjective interpretations to be inferred (Flick 2023). A critical perspective was adopted, grounded in the understanding that bioethical challenges arise within diverse sociocultural contexts and, therefore, must be addressed through a human rights framework to ensure the protection of human dignity (Albuquerque 2011). In this discussion, the term "capacity" is preferred over "competence" because it derives from the notion of legal capacity, which is inherent to the human condition and encompasses both the right to hold rights and the right to exercise them (Albuquerque 2021). For the purposes of this article, an adolescent is understood as an individual between the ages of ten and eighteen, in accordance with General Comment No. 20 of the Convention on the Rights of the Child (United Nations, Committee on the Rights of the Child 2016).
Results and discussion
Assessing adolescent healthcare decisional capacity involves evaluating an adolescent patient's demonstration of decisional skills within the healthcare context (Martins et al. 2025a). This assessment is grounded in historical-conceptual perspectives on the scope of decisional capacity, which establish an intersection between bioethical and normative dimensions. The literature identifies three such perspectives: a global understanding, a domain-specific understanding, and a decision-specific understanding. In addition, two deliberative bioethical approaches to patient decisional capacity are described: one focused on the outcome of the decision, and the other centered on the patient's functionality (Albuquerque 2021; Purser 2017; Eler 2020; Saunders 2020). These theoretical and practical perspectives support the assessment of the set of skills that constitute decisional capacity, as summarized in Table 1. Currently, the most ethically aligned approach to assessing this capacity, particularly in accordance with bioethical principles and human rights, is to base the assessment on the individual's functionality at the time the decision is made (Albuquerque 2021). This is because decisional capacity is proportional to the cognitive and functional abilities the person demonstrates at a given moment, rather than being determined by the specific content of the decision itself. Such an approach reinforces the principle of respect for privacy and autonomy (Albuquerque 2021). As might be expected, this position is not without criticism. However, many of these reviews can be mitigated by taking into account the adolescent patient's ability to comprehend and anticipate the potential magnitude of health-related harm resulting from their decision (Martins et. al. 2025b). A modern understanding of informed consent as a patient's right, from the perspective of human rights-based bioethics, combines information, voluntariness, and healthcare decisional capacity (Albuquerque 2015; General Medical Council 2020). This article discusses adolescent healthcare decisional capacity, focusing on specific skills involved in the process, and encourages both theoretical and practical explorations of the right to information and the identification of voluntariness. In such cases, the responsibility of the assessor is to ensure that the assessment of decisional capacity is conducted in alignment with human rights principles and, when applicable, adheres to the specific criteria outlined in relevant legislation. Once capacity is established, it is the adolescent's responsibility to assess the content and consequences of the decision being made. This understanding implies that irrationality alone does not invalidate a decision. Throughout life, individuals may make decisions that seem mistaken, irrational, or even self-harming from the perspective of an external observer. However, such decisions do not automatically disqualify a person from being considered capable in terms of decisional capacity (Albuquerque 2021). Consequently, the assessor's position as an outsider does not deliberate a privileged or superior perspective, and thus does not justify interference solely on the basis of disagreement with the content of the decision.
Table 1 Typology of the scope of the historical-conceptual understanding of decisional capacity and related deliberative bioethical stances
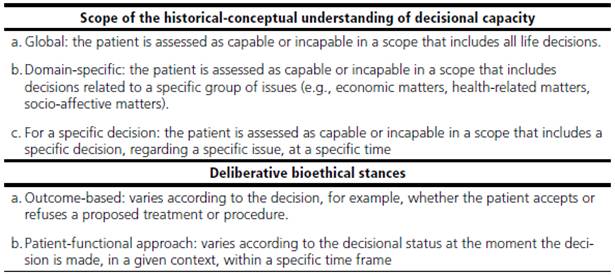
Source: prepared by the authors.
When it comes to assessing the decisional capacity of adults in civil matters not specifically related to healthcare, in many countries, the assessor is typically a legal professional, such as a lawyer (Albuquerque 2021). In contrast to countries like Australia, Canada, and England, which have established their own standards for decisional capacity, including those applied in healthcare, Latin American countries such as Brazil lack specific legal provisions. This absence affects not only the broader assessment of decisional capacity but also the more practical aspect of healthcare-related decisional capacity, which is the focus of this article. The Brazilian initiative most closely resembling a regulatory framework in this regard comes from the Federal Council of Psychology of Brazil, which provides guidance for psychologists on assessing decisional capacity, without reference to the patient's stage of life (Federal Council of Psychology of Brazil 2019). These authors argue that regulation should fall under the authority of human rights bodies, not professional associations, a pioneering initiative that deserves attention. In the specific case of healthcare decision-making for children and adolescents, even in Latin American countries with more advanced legislation in this area, such as Argentina, Costa Rica, Ecuador, Uruguay, Venezuela, and Colombia, the role of the assessor of healthcare decisional capacity remains unaddressed (Eler 2022). In this legislative gap, respect for the personal autonomy of adolescent patients, and, consequently, the human right to privacy, has persistently been challenged by mitigating practices, such as mild paternalism exercised by healthcare professionals and legal guardians.
Specifically in the healthcare context in Brazil, the assessment of the competencies that establish decisional capacity has traditionally been performed by medical professionals. However, this approach is limited and inconsistent with the understanding that, influenced by factors both intrinsic and extrinsic to the adolescent patient, including various factors not limited to biological aspects, healthcare decisional capacity is inherently multidisciplinary and should be assessed accordingly (Albuquerque 2021; Martins et al. 2025a). Furthermore, since an adolescent's healthcare decisional capacity is not directly proportional to their physical or mental disabilities or psychiatric conditions, the assessment should not be restricted to neurologists or psychiatrists, although some authors acknowledge that the input of these specialists may be necessary in certain cases (New South Wales 2007; Saunders 2020; Tan 2024). The central issue is not who performs the assessment, but how it is conducted, ideally based on criteria that are both clear and objective (Tan 2024). Detaching the assessment of an adolescent's healthcare decisional capacity from any single professional domain allows the patient's individual characteristics to be considered from multiple perspectives, thereby enhancing the likelihood of accurately understanding the authenticity of their decisions.
The Mental Capacity Act 2005, under English law, applies to adolescents aged sixteen to eighteen and brings relevant considerations in this regard (United Kingdom, Office of the Public Guardian 2007). In the Code of Practice for this law, it is stated that there is no single designated professional responsible for assessing a person's decisional capacity, including healthcare decisions (United Kingdom, Office of the Public Guardian 2007). Rather, responsibility lies with the person deemed most appropriate for the decision at hand, which may include physicians, social workers, informal caregivers, or other professionals directly involved in the patient's care. In this specific context, the possibility of informal caregivers participating in the assessment of healthcare decisional capacity contrasts with our position, which holds that the assessor should possess a higher education degree, even if not necessarily in the health field, combined with specific training for this purpose; that is, certified through a theoretical-practical course with state validation. This approach is intended to ensure that the assessor upholds a minimum level of professional competence in dealing with such a complex matter. Training these assessing skills across diverse professionals has the potential to optimize the assessment of healthcare decisional capacity, enabling a truly multidisciplinary approach to the matter (Menguy et al. 2024). This training should provide professionals with evidence-based strategies to generate reliable reports for legal and bioethical purposes, while respecting patient rights and addressing practical gaps in the assessment process, such as proper documentation in the patient's medical record (O'Connor et al. 2024; Sarang and Carter 2025). Professionals must develop technical competence to assess the skills comprising decisional capacity, particularly among adolescents, within a context that also allows them to recognize situations in which various environmental factors may influence these skills (Martins et al. 2025a; McWilliams et al. 2024). A recent field study (n = 44) involving professionals assigned to assessing the decisional capacity of adults in England revealed significant uncertainties experienced by assessors throughout the assessment process, which could be mitigated through targeted training programs. Key challenges identified include: difficulty in obtaining a comprehensive understanding of the patient's personal history and personal history; challenges in recognizing the presumption of capacity in adults, which, when applied to adolescents, entails acknowledging that they should not be presumed incapable; and the limited consideration of external factors influencing individuals' decisions (McWilliams et al. 2024). This overview further considers the associated bioethical and legal dimensions of decisional capacity.
In Ontario, Canada, the Department of Justice, through the Office of the Public Guardian and Trustee, maintains a publicly accessible list of trained and legally authorized capacity assessors. These professionals, who may be physicians, psychologists, social workers, nurses, or occupational therapists, are empowered under the Substitute Decisions Act of 1992 (Ontario 1992) to perform capacity assessments. They are officially designated as Capacity Assessors. This consideration has two key implications for assessing decisional capacity, which can also be applied to adolescent healthcare. First, there should not be a specific professional designated for all situations; rather, the assessor should possess sufficient knowledge of both the specific decision and the adolescent's broader circumstances. Second, the assessment is inherently relational and context-dependent, influenced by multiple factors, consistent with the nature of healthcare decisional capacity itself, including scenarios in which the adolescent refuses treatments or procedures (Martins et al. 2025a; Martins et al. 2025b).
It is essential that the assessor of adolescent healthcare decisional capacity possesses in-depth knowledge of the factors influencing this capacity, including the refusal of treatments and procedures (Kane et al. 2022; Ariyo et al. 2023; O'Connor et al. 2024; Martins et al. 2025a; Martins et al. 2025b). The following points regarding the assessor's role are particularly noteworthy:
When assessing whether an adolescent possesses the skills comprising healthcare decisional capacity, the assessor should adopt an active role in promoting personal autonomy and supporting adolescent health. This entails encouraging the patient to reflect on their decisions, providing clear and accessible information, and ensuring that they feel respected, embraced, and key to their care (Albuquerque 2021). Importantly, the assessor should not participate in bioethical deliberations regarding the patient's decisions, as this would create a conflict of interest.
The assessor of adolescent healthcare decisional capacity must possess the ability to understand and engage with another person's feelings, thoughts, and perspectives without judgment or imposing their own emotions; in other words, they must demonstrate empathic capacity (Albuquerque 2023b).
Throughout the health decisional-making process for adolescent patients, the professional assessing healthcare decisional capacity must act in accordance with the protection, advocacy, and promotion of human rights, and must not induce, nor be influenced by, political, philosophical, moral, ideological, religious, or sexual orientation convictions, or by any form of prejudice (Federal Council of Psychology of Brazil 2019).
When an assessor is uncertain whether a patient possesses healthcare decisional capacity, it is recommended to refer the patient for assessment by a more experienced professional (Tan 2024).
Some issues regarding the qualifications of healthcare decisional capacity assessor, particularly in the assessment of adolescent healthcare decisional capacity, still require further clarification. The literature provides no evidence comparing assessments conducted by healthcare professionals with those performed by professionals from other fields. Similarly, there is no data indicating that evaluation by a single assessor is sufficient to determine adolescent healthcare decisional capacity. Moreover, it cannot be assumed that involving a panel of assessors is mandatory, as such a panel could easily become unnecessarily large. Despite this, given that healthcare decisional capacity is composed of skills influenced by a wide range of determinants, it becomes even more complex to determine whether a single individual could possess sufficient expertise to assess it. In contrast, the fact that such assessments can be conducted for a specific decision at a specific point in time appears to narrow the range of skills required of the assessor. Nonetheless, it is undeniable that these points require further discussion, which underscores the need for continued scientific research.
Final considerations
The assessor of adolescent healthcare decisional capacity must be able to understand the health-disease continuum and the factors that shape these skills, considering the patient's trajectory and sociocultural context, while promoting personal autonomy in a contextualized manner grounded in respect for human rights. Recognizing that evidence-based assessment of adolescent healthcare decisional capacity constitutes the most appropriate standard for ensuring ethical, safe, and high-quality care is essential for advancing professional practice and safeguarding patients' rights. Consequently, future research should aim to compare the accuracy of assessments conducted by individual versus multiple assessors, as well as to evaluate the reliability of analyses performed by professionals from diverse disciplinary backgrounds.

