











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
The data on violence against children and adolescents (NNA) in Colombia are of concern. In an observation window from 2015 to 2017, the Colombian Institute of Family Welfare (ICBF, 2018) recorded 56,782 cases of sexual abuse against underage children. The National Institute of Legal Medicine and Forensic Sciences (2018) reported 10,398 cases of intrafamily violence against this same population. These figures suggest that on a daily average during the period 2015-2017, 61 children and adolescents in Colombia were victims of sexual abuse and/or physical or psychological mistreatment.
Worldwide, the panorama does not seem to be very different. According to the World Health Organization (WHO, 2018) during 2016-2017, 23% of children and adolescents were victims of physical violence and 18.2% of girls under 18 experienced sexual abuse. In adulthood, the consequences of these experiences can be devastating. According to (Malarbi, Abu-Rayya, Muscara, and Stargatt, 2017) between 20% and 80% of children and adolescents who experience abuse develop post-traumatic stress disorder (PTSD), which is one of the most consistent predictors of mental illness in adult age.
Authors such as (De Young, Kenardy, and Cobham, 2011) argue that research in the field of childhood trauma requires more studies to understand the cognitive processes that are affected after an early traumatic experience. Although this situation has changed in the last ten years, addressing the effects on cognitive processes during childhood remains an underexplored area (Noriega et al., 2020). Specifically, in the case of Colombia and according to the review conducted by the authors of this study, there is little research that addresses this relationship between childhood trauma and its effects at the brain level.
On the global scene, there is a similar picture. In agreement with the results of a meta-analysis conducted by Malarbi et al. (2017), in a twenty-year period (1995-2015), it was found only 27 studies that addressed the effects of childhood trauma on neuropsychological variables. A same scenario occurs with neuroimaging findings in cases of childhood trauma, in which, in most cases, brain imaging has been performed when the childhood trauma victim is an adult, resulting in the loss of information on the immediate effect of trauma on the children and adolescents´ brain, who are still in formation. Recently, (Kribakaran, Danese, Bromis, Kempton, and Gee. 2019) issued a meta-analysis that identified 15 studies employing structural neuroimaging techniques in a sample of children with PTSD. The reported results suggest that, at the structural level, the affected areas after a traumatic experience are like those reported in adults, with important changes in brain maturation trajectories, mainly at the level of the frontal lobe.
Regarding functional neuroimaging studies in children with a history of psychological trauma, (Milani, Hoffmann, Fossaluza, Jackowski, and Mello. 2017) conducted a meta-analysis of studies published between 2000 and 2014, in which they compare the results obtained from the different tasks implemented. In the case of word list learning tasks, the included studies report hypoactivation in the right hippocampus compared to controls. In implicit face processing tasks, alterations in the synchronization patterns of the amygdala and hippocampus are reported. Finally, for go/not go inhibitory control tasks, greater activation of the middle frontal gyrus, right insula and anterior cingulate is observed. However, it should be noted this meta-analysis only identified eight studies published in a fourteen-year period, which clearly shows the need to broaden the empirical base to allow more accurate generalizations.
On the other side, it is important to advance functional neuroimaging studies in the child population, since the brains of children and adolescents are still maturing and consequently, areas such as the frontal lobe, which completes its development around the second decade of life, are particularly sensitive to the effects of early traumatic experiences (Barrera, Calderón, Trejos, & O'Boyle, 2017). To this end, the present study aims to describe preliminary results of brain activation patterns using a functional neuroimaging technique in a sample of children with PTSD and compare them with a group of controls to establish possible anatomical-functional correlate.
Method
The study adopted a quasi-experimental methodology taking a non-representative sample of 15 children with PTSD from Medellín (Colombia) and its metropolitan area (2 boys and 13 girls aged between 9 and 14), who had lived at least one traumatic experience and whose scores on the child scale of PTSD symptoms (Bustos, Rincón, & Aedo, 2009) were greater than 24 points. PTSD diagnoses were confirmed by clinical psychiatric interview, conducted by professional psychiatrists at the Mental Health Center of the CES University in Sabaneta (Antioquia). On the other hand, a group of 7 participants (5 boys and 2 girls aged between 9 and 14) formed the control group (with scores below 8 on the child PTSD symptom scale). All participants, 5th to 9th graders, were contacted through meetings with parents and tutors in public schools, in the metropolitan area of the Aburrá Valley. The parents who agreed to their children's participation were given the respective informed consent (see ethical considerations) and the children were informed about the objective of the study in simple language (and filled out the respective informed assent form). All participants were right-handed, with no previous history of psychiatric disorders, craniocerebral trauma or learning disorders. In order to rule out other comorbid psychiatric conditions, the Brief Neuropsychiatric Interview for Children (MINI Kids; Sheehan et al., 1998) was used.
Procedure
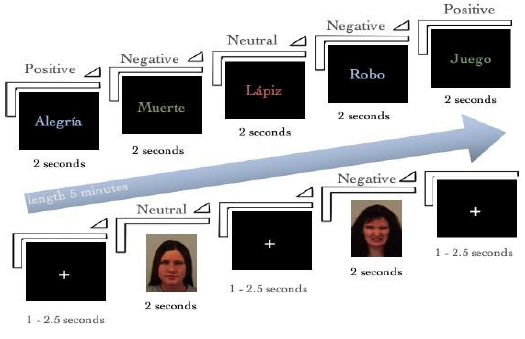
Once the participants were selected, they were scheduled for the functional imaging session. All participants were shown the equipment (see description below) and a practice was performed on similar equipment located in a next-door room. During functional imaging, two experimental tasks were introduced in a randomized manner, which were arranged by the research team in the Psychopy software (see Figure 1). To record the responses, a glove-like box of fiberglass buttons was used to automate the recording of the responses. For the two tasks, the reaction time and the number of hits were recorded for each condition. All neuroimaging was done in a single session, with a total duration of approximately two hours (including the practice session).
Emotional Stroop task
This task measures the ability to exert inhibitory control over a stimulus with different emotional valence. It was performed in two parts: the first was a standard version of the Stroop effect (for a detailed description see (Lezak, Howieson, Bigler, & Tranel, 2012), which was assessed by comparing congruent and incongruent words. The second part considered the emotional valence of the words, and its design was based on an adaptation of the original task proposed by (Thomaes et al. 2013), which consists of a series of 72 words with emotional content (24 positive, 24 neutral and 24 negative), which were randomly introduced by means of a projection in sequences of 2.5 seconds and with variable intervals between 1 and 3 seconds in duration. The participants' task consisted of identifying as soon as they could the printed color of each word (regardless of its emotional valence) and pressing the corresponding button on a kind of fiber optic glove placed on their right hand as appropriate: a word in red (left button, index finger), a word in green (middle button; middle finger), a word in blue (right button, ring finger). An example of the type of words used is introduced in figure 2.

Facial emotion processing tasks
This task assesses the ability to process nonverbal stimuli with different emotional valence. It consisted of an adaptation of the task proposed by (Masten et al. 2008) in which 72 faces (selected from the Karolinska Directed Emotional Faces; Lundqvist, Flykt, & Öhman, 1998) were taken and arranged as follows: 24 faces expressing negative emotions, 24 expressing no emotion, and 24 expressing positive emotions. Each trial was introduced randomly with 2.5-second intervals, followed by variable intervals of 1 to 3 seconds in duration. Participants had to recognize the emotional valence of the face and by means of a kind of fiber optic glove pressing the button in accordance with the use of their right hand as follows: face with negative valence (left button, index finger), face with neutral valence (middle button, middle finger) and face with positive valence (right button, ring finger) (See Figure 3).
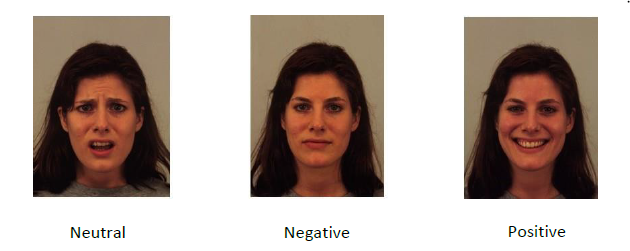
Image acquisition
All images were acquired using a Siemens (Skyra) three-tesla 20-channel Magnetic Resonance Imaging (MRI) machine with 20 channels. A sagittal T1-weighted scan was employed for the acquisition of the anatomical images using the following parameters: Total volumes=176; repetition time=2.3 sec; voxel size=0.98 x 0.98 x 0.98 mm; echo time=3 sec; field of view=250mm x 250mm; flip angle=9º. The fMRI (Functional Magnetic Resonance Imaging) data (47 axial acquisitions) were acquired with a gradient echo-planar imaging (EPI) with the following parameters: total volumes=184; repetition time=2.5 sec; voxel size=2.5 x 2.5 x 2.5 x 3 mm; echo time=20sec; field of view=200mm x 200mm; flip angle=70º.
Image data processing and analysis
FSL software was used for pre-processing and analysis of all anatomical and functional images. After extraction of the brain images using BET, a timing correction was done to temporally align the fMRI acquisitions. Motion correction of the data was also performed using MCFLIRT, as well as spatial smoothing using 5-mm FW-HM, to reduce noise effects. Initially, the functional images of each participant were aligned through their own previously registered structural image, followed by a transformation of their original space into a standardized MNI-152 space. A first level general linear analysis (GLM) was performed by a double gamma convolution to correct the delay between the EPI signal and the hemodynamic response function (HRF). At a second-order level, a fixed-effect GLM (see Beckmann, Jenkinson, & Smith, 2003; Woolrich, 2008; Woolrich, Behrens, Beckmann, Jenkinson, & Smith, 2004) was conducted on the blood oxygenated response (BOLD) to word stimuli as a function obtained from members of each group (PTSD vs. Control). The set of brain maps containing the significantly active voxel clusters as determined by family-wise t-tests were analyzed using a nonparametric activation set at z > 2.3 with a cut-off value of p < 0.05. Gaussian random field theory was considered to correct multiple comparisons (Worsley, Taylor, Tomaiuolo, & Lerch, 2004).
Ethical considerations
The present study was conducted in accordance with the most recent version of the Helsinki declaration (World Medical Association, 2018); and was approved by the ethics committee of CES University. Based on the protocol defined for research in human subjects by the same Committee, the 22 participants signed an assent, and their parents or legal representative signed the informed consent form.
Results
Emotional Stroop task processing
In order to verify the Stroop effect in both groups, a mixed ANOVA analysis (2 groups [cases, controls] X 2 conditions in the Stroop task [congruent, incongruent]) was conducted for the response time and number of hits variables. This analysis revealed that both groups had longer reaction times F (1, 20) = 19.4, p<0.05, and lower number of hits, F(1, 20) = 5.887, p<0.05, for incongruent words. For the case of words with emotional content, the 2X3 mixed ANOVA analysis (two groups [cases, controls] by three conditions [neutral, positive, or negative]), revealed no difference neither at the group level, nor at the condition level. However, the PTSD group showed slower reaction times in the processing of words with negative emotional content, without this difference reaching the significance threshold defined a priori (p<0.08), as shown in graphic 1.
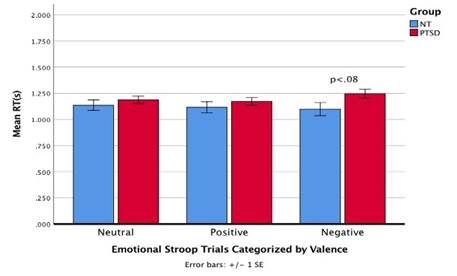
Graphic 1 Reaction time for PTSD and NT children when processing ink color when words of different emotional valence are superimposed.
On the other hand, the analysis of the functional neuroimages obtained during the performance of this task shows a greater activation of the left precentral gyrus in the PTSD group, when compared to the control group, during the processing of negative words (see Figure 4).
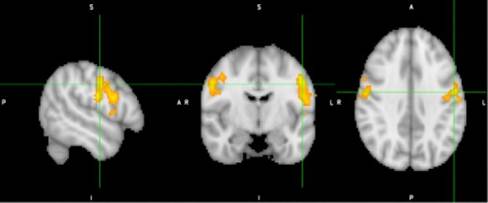
The image shows a greater activation of the left precentral gyrus in the group of children with PTSD, during the processing of negative words with the following Z max= 4.05; MNI, (-52, -8, 36).
Processing Faces with emotional content
Regarding the processing of faces with emotional content the mixed ANOVA 2X3 analysis (2 groups for three conditions (positive, negative, and neutral), points to an effect associated with valence F (2, 32) = 8.26, p<0.05 for the negative faces condition in the group of children with PTSD, who were faster executing this part of the task, compared to those in the control group (see Graphic 2).
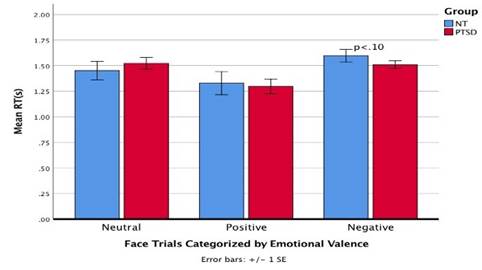
Graphic 2 Reaction times for children with PTSD and NT when processing faces of different emotional valence.
Regarding brain activation areas, it was observed greater activation of the left paracingulate gyrus in the group of children with PTSD, during the processing of faces with negative emotional content, compared to the brain activation of the control groups (see Figure 5).
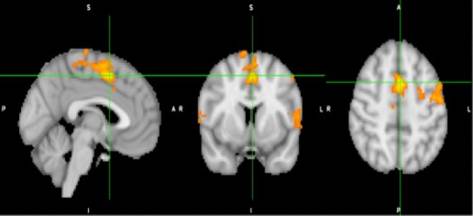
Figure 5 Neuroimaging of the PTSD group during the processing of faces with negative emotional content.
The image shows a greater activation of the paracingulate gyrus in the PTSD group, when processing the emotional content of the faces. Such activation is particularly strong in the case of faces with negative emotional content (values: Zmax=4.99; MNI, [x= -2, y=8, z=50]).
Discussion and conclusions
The aim of the present study was to describe preliminary results of brain activation, using a functional neuroimaging technique, in a sample of children with PTSD in order to establish possible anatomo-functional correlates when compared with a control group.
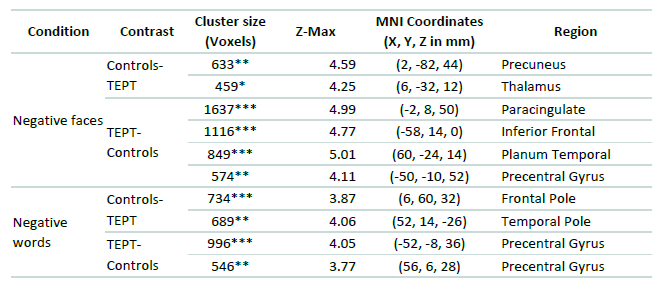
Summarizing, the results point to changes in the activation patterns of frontal structures in children with PTSD; a finding identified in previous works that used neuropsychological measures (Carrión & Weems, 2017; Barrera et al., 2017; Barrera, Calderón, & Bell, 2013). Such changes are particularly remarkable as regards the case of negatively valenced stimuli (see Table 1). This is interesting, if one considers that the frontal lobe is one of the last structures to acquire its complete maturation, so its development is highly influenced by the external factors that are part of infant development (Anderson, Anderson, Northam, Jacobs, & Catroppa, 2001).
However, when reviewing in detail the frontal areas involved in negative valence emotional processing, structures such as the frontal pole, the inferior frontal sulcus and the paracingulate gyrus are found; a result that is noticeable because these structures are part of a network associated with emotional regulation processes. This finding is consistent with (Ardila. 2013) and (Fuster´s proposal. 2015), which state that within the executive functions it is possible to distinguish a metacognitive and an emotional component. Particularly, in children with PTSD participating in the present study, the emotional inhibitory control processes involved in the Stroop-type task may be affected.
A second aspect to discuss is the evident contradiction found between the longer times spent by the group of children with PTSD in the valoration of words with negative emotional content in the Stroop task and the shorter times spent by this same group in the case of emotional face processing with negative valences. In this regard, there are several elements to consider that may explain this outcome. First, it is the nature of the stimuli employed: while in the first task they require verbal processing, in the second one the stimuli are of a visual nature. The tendency of people with PTSD to process more quickly facial expressions with negative valence has been a consistent finding since it was reported by (Masten et al. 2008) and has been the subject of several analyses. Lately, (van den Bulk et al. 2016) have suggested that such a result could be associated with an amygdala-mediated primary emotional response; however, the data obtained in the present study do not seem to fit this possibility given that no differences in amygdala activation patterns were found. A second element concerns the task itself: in the Stroop task the participant must endeavor to inhibit information that is not necessary (the emotional valence of the words) in order to give a response, while in the emotional face processing task the participant must indicate directly and explicitly the emotional valence of the facial expression. A theoretical model that could contribute to explain this aspect is the one postulated by (Gyurak, Gross and Etkin. 2011), who propose a dual model of emotional processing, according to which there are explicit emotional regulation and components of automatic nature.
Consequently, the processing involved in the face task, being oriented to evaluate the emotional valence of the face, would generate a faster explicit processing, associated to an avoidance behavior of the negative stimulus. On the other hand, the color of the word process is regulated by an implicit processing of the word´s emotional valence that generates an interference in the performance of the task. However, in the specific case of children with PTSD, the difficulty seems to be more associated with an impairment, not so much in detecting stimuli with negative emotional content, but in controlling the response that it generates. If this is the case, the reformulation of Gyurak's dual model of emotional processing by (Braunstein, Gross, and Ochsner. 2017) may help to include the mechanisms that are involved in the emotional processing of negative stimuli in children with PTSD.
According to the reformulation of Gyurak's dual model of emotional processing, as well as the explicit-implicit regulation processes, there is an additional procedural variable ranging from more automatic to more controlled. In this sense, children with PTSD, perform a more automatic processing of negative valence stimuli (which would explain the faster reaction times for the processing of negative faces) and would be less accessible to controlled processing (which would affect the word color process with negative emotional content).
Although it is true the present study shows preliminary data that do not allow an adequate generalization, they introduce the possibility of approaching the emotional processing associated with trauma through two courses of action: one oriented to the more cognitive and explicit aspects of the emotion linked to trauma; and the other oriented to the more physiological aspects related to the implicit processing of the emotional content.
Finally, the analysis of the data obtained allows pointing out the impact that the early traumatic event has on brain development, particularly at the frontal lobe level, as well as the deep relationship between the cognitive and emotional components in the emergence and maintenance of the symptoms associated with PTSD. A better understanding of this relationship will allow the development of therapeutic techniques more adjusted to this population in the Colombian context.
Concerning the limitations of the present study, first, it is necessary to mention the size of the sample (22 participants in total), not only because of the low number of participants, but also because of the difference in the size of the groups (15 and 7, respectively) and the gender distribution of the groups (more girls than boys in the PTSD group, and more boys than girls in the control group). According to the authors of this study, the last aspect could be reflecting more an epidemiological reality, in which girls are more susceptible to experience traumatic situations, when compared to boys. As this paper is part of a project with a larger sample, it aims at confirming or discarding the achieved results in the future. To conclude, with respect to the facial stimuli used, it is suggested to work with faces whose phenotype is similar to that of the participants. In this sense, using stimuli such as those validated by (Zapata, Zapata, Gantiva, Suárez and Barrera. 2020) for the Colombian population, could help in terms of task constructions in which the emotional component plays an important role.

