











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Cancer is a growing public health problem in Colombia, considered the second leading cause of death after cardiovascular diseases, with more than 100,000 new cases per year [1]. The threatening nature of this disease has been a determining factor for the use of complementary and alternative medicine (CAM), as evidenced by the high frequency of use reported in oncology patients compared to other patients with chronic conditions [2]. CAM is defined as a group of medical and healthcare systems that involve practices and products that are not considered part of conventional medicine, which includes mind-body therapies, biological based practices, energetic CAM, whole medical systems, and body manipulation [3].
Worldwide, a frequency of use ranging from 9.8% to 76% has been found in oncology patients [4]. In Colombia, the National Cancer Institute reports that 73.5% of its adult patients and 81.9% of the caregivers of pediatric patients use CAM [5,6]. The main reasons for using CAM are related to palliative purposes, their "natural" character, and their positive effects on quality of life [7-9]. However, many users of CAM obtain information about these practices from people other than medical professionals [10], avoiding communicating its use to their treating oncology physicians [11], often unaware of the potential side effects that may arise from their concurrent use with conventional treatment [7,8,12,13]. In that manner, it has been found that certain foods can interact with medications used in conventional treatment, for example, turmeric improves antitumor activity [14], and the Guinea Henweed has shown to reduce tumor burden, metastasis, and to improve the peripheral immune response in murine myeloid leukemia models [15].
Bucaramanga is one of the cities in the country with a Cancer Population Registry [13] that reports a growing trend in the incidence of various cancer diagnoses [16,17], in which were reported 3,801 new cases of cancer (excluding non-melanoma skin cancer) by 2016, with an incidence rate similar to that of the rest of the country [18], in addition to the increasing number of cases due to the aging population, and some of the health barriers presented by gastric oncology patients in the city [19] make it worth to study the frequency of use of alternative and complementary medicines among oncology patients in the city, information that is crucial for appropriate oncology care planning.
Therefore -and given that patients often do not discuss this issue with their treating physicians [11,20-22], and that the objective of this study was to characterize the frequency, reasons for use, and specific practices of oncology patients regarding CAM in the city of Bucaramanga, Colombia-, we hope to expand with the results the current knowledge on the use of CAM in Colombia and in the department of Santander, which involves as well the reasons for use and the main products used by the patients, under the concept of integrative medicine. Consequently, CAM therapies are integrated into the main course of treatment [3].
Method
A descriptive cross-sectional study was conducted and approved by the ethics committees of Hospital San Ignacio/Pontificia Universidad Javeriana in Bogotá and Fundación Cardiovascular de Colombia in Bucaramanga. All participants gave their consent to participate.
The methodology has been described previously [23]. A survey was designed based on the classification of CAM proposed by the National Center for Complementary and Integrative Health [24] and the results of focus groups that explored the types of practices and reasons for the use of CAM among oncology patients [25], that could represent the total CAM domains. The survey included sociodemographic data, clinical characteristics, frequency of CAM use according to standard categories, reasons for use, and specific practices.
A sample size of 525 subjects was defined based on an expected CAM’s frequency of use of 70% [26], A 95% confidence interval, a 5% precision, and a design effect of 2 were used. Sampling was carried out using random days, with the recruitment day considered a cluster and an expected intraclass correlation of 3.5%, which led to the need for at least 35 clusters with blocks of 15 observations each. Various institutions in the city were invited to participate, but only Hospital Internacional de Colombia of Fundación Cardiovascular de Colombia participated.
Patients over 18 years old with a histopathological diagnosis of cancer, who were undergoing active treatment with chemotherapy (systemic treatment) or had received radiotherapy or surgery in the past 4 months, were included. Patients at any clinical stage and with any type of cancer were included. Patients who could not answer the questionnaire due to their physical or mental condition were excluded, and participation by family members or caregivers on behalf of the patients was not accepted. The information was recorded on the RedCap platform [27] by pollsters previously trained. A pilot was conducted by 10 patients, in which the compressibility of the survey was tested. Also, after collecting the data, 10% of the patients was called randomly in order to verify the quality of data.
Absolute frequencies, relative frequencies, and measures of central tendency were used for numerical variables and data analysis. The frequency of use was reported as a percentage, and clinical and sociodemographic characteristics between CAM users and non-users were compared using the chi-square test and the Kruskal-Wallis test, according to the data distribution and the nature of the variables. The significance level was set at a p-value of <0.05. Specific practices reported in open-ended questions were coded and grouped according to the basic description of the products (biological or processed) or practices (mind-body and others). Once coded and grouped, absolute and relative frequencies were measured and compared based on their palliative or curative purposes. The analysis was conducted using the Python® statistical package.
Results
A total of 528 patients with an active diagnosis participated, with a higher participation of women, patients with subsidized health insurance, and patients with a lower socioeconomic status. The most commonly reported type of treatment was chemotherapy (Table 1). Additionally, the most frequent type of cancer was breast cancer, followed by colon cancer and stomach cancer (Supplementary Table 1).
Table 1 Description of Sociodemographic and Clinical Variables versus CAM Use.
| Variables | Total | CAM Users | CAM No Users | p-value | |
|---|---|---|---|---|---|
| N | 528 | 352 | 176 | ||
| Age | Mean | 56.6 | 56 | 58 | 0.131 |
| SD | 14.2 | 13.8 | 14.9 | ||
| n (%) | n (%) | n (%) | |||
| Sex | Women | 375 (71.0) | 255 (72.4) | 120 (68.2) | 0.360 |
| Men | 153 (29.0) | 97 (27.6) | 56 (31.8) | ||
| Religion | Catholic | 385 (73.1) | 259 (73.6) | 126 (72.0) | 0.335 |
| Christian | 108 (20.5) | 72 (20.5) | 37 (21.0) | ||
| Other | 11 (2.1) | 9 (2.6) | 2 (1.1) | ||
| No Religion | 23 (4.4) | 12 (3.4) | 11 (6.2) | ||
| Marital Status | Single | 152 (28.8) | 100 (28.4) | 52 (28.4) | 0.888 |
| Married | 187 (35.5) | 122 (34.7) | 65 (36.9) | ||
| Free union | 101 (19.1) | 69 (19.6) | 32 (19.6) | ||
| Divorced | 41 (7.8) | 30 (8.5) | 11 (8.5) | ||
| Widowed | 47 (8.9) | 31 (8.8) | 16 (8.8) | ||
| Socioeconomic Status | Low | 381(72.2) | 248(70.5) | 133(72.2) | 0.155 |
| Medium | 142(26.9) | 102(29.9) | 40(27.7) | ||
| High | 5(0.9) | 2(0.6) | 3(1.7) | ||
| Occupation | Unemployed | 54 (10.2) | 37 (10.5) | 17 (9.7) | 0.835 |
| Employed | 43 (8.1) | 26 (7.4) | 17 (9.7) | ||
| Student | 7 (1.3) | 4 (1.1) | 3 (1.7) | ||
| Homemaker | 314 (59.5) | 207 (58.8) | 107 (60.8) | ||
| Self-Employed | 78 (14.8) | 55 (15.6) | 23 (13.1) | ||
| Retired | 32 (6.1) | 23 (6.5) | 9 (5.1) | ||
| Educational Level | None - Primary Education | 237(44.9) | 139(39.5) | 98(55.7) | 0.004 |
| High School | 201(38.1) | 144(40.9) | 57(32.4) | ||
| Technical/Technological | 54(10.2) | 40(11.4) | 14(8.0) | ||
| University - Postgraduate | 36(6.8) | 7(4.0) | 29(8.2) | ||
| Health Insurance | Contributory | 170 (32.2) | 113 (32.1) | 57 (32.4) | 0.950 |
| Subsidized | 345 (65.3) | 230 (65.3) | 115 (65.3) | ||
| Complementary Plan | 8 (1.5) | 6 (1.7) | 2 (1.1) | ||
| Other | 5 (0.9) | 3 (0.9) | 2 (1.1) | ||
| Cancer Stage | Localized | 279(52.8) | 191(54.3) | 88(50.0) | 0.093 |
| Lymph Nodes Involved | 103(19.5) | 68(19.3) | 35(19.9) | ||
| Metastasis | 134(25.4) | 89(25.3) | 45(25.6) | ||
| Most Common Cancer Diagnosis | Breast | 166 | 124(35.2) | 42(12.0 ) | >0.05 |
| Colon | 49 | 36(10.2) | 13(3.7) | ||
| Stomach | 36 | 19(5.4) | 17(4.8) | ||
| Ovary | 31 | 24(6.8) | 7(2.0) | ||
| Cervix | 26 | 15(4.3) | 11(3.1) | ||
| Treatment-Related Side Effects | Yes | 300(72.0) | 260(73.9) | 120(68.2) | 0.205 |
| No | 148(28.0) | 92(26.1) | 56(31.8) | ||
| Treatments Received | Chemotherapy | 438(83.5) | 296 (84.1) | 142 (80.7) | 0.038 |
| Radiotherapy | 163(30.9) | 112(31.8) | 51 (29.0) | 0.890 | |
| Surgery | 221(41.9) | 149 (42.61) | 72 (41.0) | 0.023 | |
| Palliative Care | 1(0.2) | - | 1(0.6) | 0.968 | |
Note. SD (Standard Deviation). Note: For the age variable, the Kruskal-Wallis test was used due to the nature of the variable and the non-normal distribution of the data. For other variables, the chi-square test was used. Bold text indicates statistically significant values.
A total of 67% of the surveyed patients reported using CAM. CAM users had a higher educational level and more frequently received systemic treatment and surgery (Table 1). The use of biologically based medicines, especially natural origin foods, was found to be more common, whereas the use of medicine based on alternative medical systems was less frequent. The primary reason for use was related to palliative goals; patients reported that they mostly obtain information about CAM from sources other than their healthcare team, with few patients discussing this topic with their doctors. A high percentage of patients reported having a favorable experience with CAM use, perceiving it as low-cost (Table 2).
Table 2 Practices of Alternative and Complementary Medicine (CAM) Use.
| Items Describing CAM Use | % | ||
|---|---|---|---|
| CAM Types | Biological Basis | Special Foods of Natural Origin | 64% |
| Special Diet | 14% | ||
| Herbal Products | 55% | ||
| Animal-Based Products | 32% | ||
| Products Intended to Supplement Nutrition | Vitamins and Supplements | 48% | |
| Alternative Medical Systems | Homeopathy | 11% | |
| Traditional Practices | 1.7% | ||
| Acupuncture | 0.3% | ||
| Other Therapies | Massage | 3% | |
| Energy Therapy | 3% | ||
| Mind-Body Therapy | 2% | ||
| Reasons for Use | Palliation | Counteracting Adverse Effects of Treatment or Disease | 52% |
| Emotional Support | 8% | ||
| Disease Control | Cure the Disease | 20% | |
| Prevent Recurrence | 16% | ||
| Toxicity | Its Natural Properties Compared to Conventional Medicine | 5% | |
| Others | Exploring All Available Options to Treat the Disease | 3% | |
| Other Reason | 28% | ||
| Initial Source of Information | Medical Recommendation (Conventional or Alternative) | 7% | |
| Another Person Outside the Medical Team (Family, Friends, Patients, Pharmacists, Marketplaces) | 86% | ||
| Media | 4% | ||
| Other | 3% | ||
| Effects of CAM Use | Favorable | 85% | |
| Indifferent | 13% | ||
| Unfavorable | 1% | ||
| Perception of CAM Costs | High Cost | 33% | |
| Medium Cost | 26% | ||
| Low Cost | 41% | ||
| Discussion with Treating Physician about CAM | Yes | 35% | |
| No | 65% | ||
| Reasons for Not Discussing It | No Need | 21% | |
| The Doctor Did Not Ask | 64% | ||
| Possible Disapproval from the Doctor | 13% | ||
| Other | 2% | ||
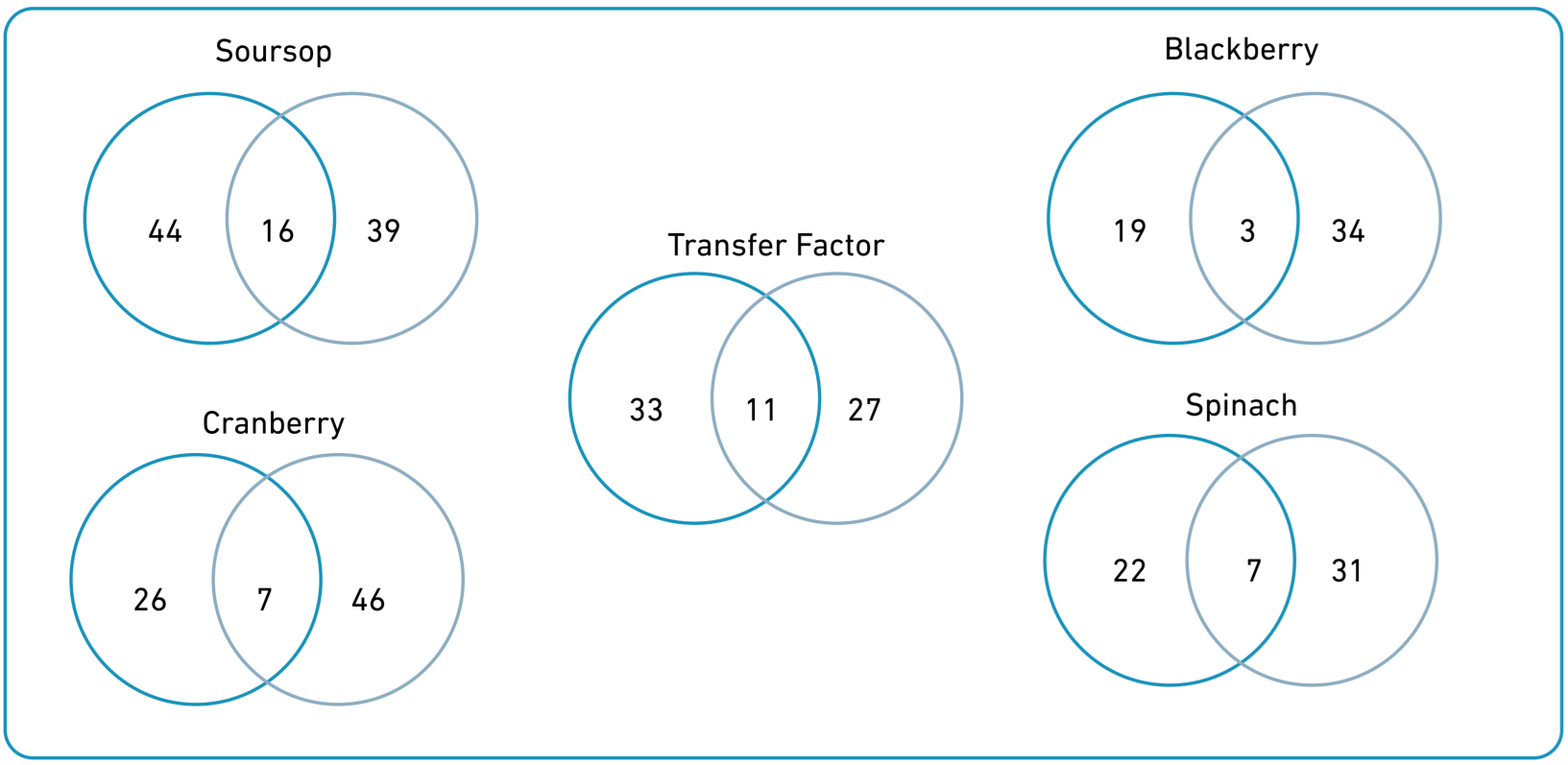
Soursop was the most reported product (36%), followed by cranberry (31%), transfer factors (27), blackberry (26%), and spinach (24%). Soursop and transfer factors had a greater frequency for curative than palliative purposes, whereas the opposite was observed for blackberry, cranberry, and spinach (Figure 1). The reasons for use of the 15 most frequent products are described in Supplementary Table 2.
Discussion
Our study found a high CAM’s frequency of use among oncology patients in Bucaramanga (67%), a value consistent with reports from Chile [28], but lower than findings in other Latin American contexts, such as Argentina and Bogotá, Colombia [6,29]. Additionally, the frequency of use reported in European countries is generally lower [9,30-32]. This variation highlights the influence of sociocultural and healthcare system factors on adopting CAM, as has been described in comparative studies [33]. In Latin America, the accessibility and affordability of CAM, coupled with traditional beliefs and a fragmented healthcare system, may contribute to its widespread use, whereas in European countries, stricter regulatory frameworks and integrative medicine models shape different utilization patterns [33].
The data were obtained from a single treatment center, similar to studies conducted in Bogotá and Chile. Therefore, the results should be interpreted cautiously in terms of their representativeness of the broader oncology patient population in the city. Beyond this, the differences in usage frequency could originate from sociodemographic and cultural patterns that influence perceptions of CAM [24,34]. The majority of CAM users were women, which aligns with previous studies showing that women have a significantly higher frequency of use [31-36], likely related to a more favorable stance towards CAM and an understanding of their health condition from various dimensions [37]. This gender disparity is a well-documented trend in CAM research and may be explained by a greater willingness among women to explore non-conventional therapeutic options, as well as a higher perceived need for holistic approaches to health [38]. Moreover, gendered health behaviors and decision-making patterns should be considered in the development of CAM-related interventions and policies.
Most CAM users in this study were patients with a low educational level and socioeconomic status, reflecting the overall behavior of the sample. However, CAM users had a higher educational level than non-users, with a statistically significant association, which was not observed for socioeconomic status (Table 1). This result is partially similar to what has been previously reported, as CAM users tend to have higher levels of education but also higher income levels [7,31,36,39,40]. Our finding is possibly related to the high frequency of use of expensive products such as transfer factors, which are marketed for widespread use but might be more accepted and affordable for individuals with higher educational levels. This paradox-where higher education is linked to greater CAM use despite economic constraints-suggests that education fosters health-seeking behaviors that include CAM, while financial limitations shape the type of CAM therapies accessed [39].
The frequent use of biologically based products could be associated with the perception of lower risk, as they are considered natural [7-9,41]. However, it has been observed that garlic, ginkgo, St. John's wort, and kava can negatively interact with anticancer medications [42]. On the other hand, frequently used products in this category, such as soursop, blackberry, and cranberry, have shown divergent results in experimental models, ranging from neurotoxicity in soursop experiments to antioxidant effects in cranberry studies [43-45]. For other commonly used products like transfer factors, we did not find information regarding their pharmacokinetic potential or interactions with anticancer treatments. This underscores a critical gap in the evidence base for many widely used CAM therapies, reinforcing the need for rigorous pharmacological studies and clinical trials to elucidate both efficacy and safety profiles [33]. Additionally, this highlights the necessity of healthcare provider training in CAM-related counseling to mitigate risks associated with its unsupervised use.
The most frequently reported reasons for use were palliative purposes, which aligns with findings from other studies [32,36]. Patients generally do not use CAM as a replacement for their conventional treatment; rather, they use it to gain better control over their health condition and to approach their illness from a psychological perspective [9,46]. In this same vein, the primary source of information for patients was their family and friends, which aligns with the conceptualization of CAM as stemming from popular knowledge [24,30,32,34,44]. However, in higher-income countries, it is assumed that the use of CAM should originate from a medical recommendation [32]. This disparity in information sources suggests a need for educational interventions aimed at improving patient awareness and encouraging dialogue with healthcare providers about CAM use. In countries like Colombia, where physician knowledge of CAM is often limited, capacity-building programs within oncology services could facilitate evidence-based guidance on CAM therapies. The integration of CAM into conventional healthcare settings requires not only patient education, but also structured training programs for medical professionals to ensure safe and effective recommendations [47].
Our study has several limitations. Conducting it at a single healthcare institution limits its external validity, even though the center where the study was conducted serves a significant proportion of cancer cases in the city and the region. The results should, therefore, be understood in relation to the characteristics of the study population, which includes a higher proportion of patients with subsidized health coverage, correlating with lower educational levels and fewer resources. However, some of our findings, such as the educational level, showed independence from the effect of these variables. On the other hand, the results reported by patients may be subject to memory bias or social desirability. Nevertheless, the presence of an interviewer has shown higher reporting of CAM use compared to when patients self-administer the survey [48]. Future studies should consider longitudinal designs to assess changes in CAM use over time, as well as qualitative approaches to understand the motivations, experiences, and decision-making processes of oncology patients regarding CAM. Integrating CAM research into national cancer control strategies could also support the development of policies that address both safety concerns and patient preferences.
The results of our study highlight the need for increased research into CAM, particularly the development of clinical studies that can support the therapeutic potential or drug interactions of products frequently used by patients in this region. Additionally, the high frequency of CAM use underscores the need to strengthen integrative medicine services, making our study's contribution relevant to this purpose. Given the widespread use of CAM among oncology patients, integrating CAM discussions into routine oncology consultations could enhance patient-provider communication and ensure safer, evidence-based practices. Moreover, public health strategies should focus on regulating and standardizing CAM products and services to align with national healthcare objectives while respecting cultural health beliefs.
Conclusions
In conclusion, this study demonstrates a widespread use of complementary and alternative medicine (CAM) among oncology patients in Bucaramanga, reflecting a trend toward complementing conventional treatment. Integrating integrative medicine services is essential to optimize oncology care.

