











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Influenza virus infections are a public health concern, particularly among children and adolescents, who are at increased risk for severe outcomes such as pneumonia [1]. The complexity of respiratory infections is often heightened by the occurrence of coinfections, where multiple pathogens co-exist within the host.
Published studies have suggested that viral infections, including influenza, can predispose patients to secondary bacterial infections, which may lead to increased morbidity and mortality [2,3]. During the 2009 AH1N1 pandemic, a significant proportion of severe cases were associated with bacterial coinfections, particularly with Streptococcus pneumoniae, Staphylococcus aureus, and Mycoplasma pneumonia [3-5].
The interplay between various respiratory viruses and the influenza virus is noteworthy. Research indicates that coinfection with influenza and other viral pathogens may lead to a synergistic effect, exacerbating the clinical outcomes in pediatric populations and raising concerns about the implications of such coinfections on treatment and management strategies [6]. Furthermore, the presence of multiple viral pathogens may alter the immune response, potentially leading to more severe disease manifestations [7].
In Mexico, influenza surveillance is conducted through the normative system for the epidemiological surveillance of respiratory viral diseases [8], primarily coordinated by the General Directorate of Epidemiology within the Ministry of Health. This system in Mexico is supported by international collaborations, including participation in the World Health Organization's Global Influenza Surveillance and Response System (GISRS). This collaboration enhances the capacity for early detection of emerging influenza strains and facilitates the sharing of critical epidemiological data [9].
Data collection occurs through a network of sentinel surveillance sites including both public and private healthcare facilities, which provide vital information on hospitalizations, laboratory-confirmed cases, and mortality associated with influenza [10]. In the last quarter of 2023, surveillance guidelines were updated to implement simultaneous screening for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and influenza A/B viruses using reverse transcription polymerase chain reaction (RT-PCR). This screening is mandated for all patients with severe respiratory symptoms and for 10% of randomly selected ambulatory patients. Additionally, when influenza infection is ruled out, a more comprehensive viral panel (including adenovirus, human metapneumovirus, etc.) is performed for (1) all hospitalized patients or those with fatal outcomes and (2) 10% of the remaining cases [8].
Understanding the epidemiology of influenza and its interaction with other viral pathogens is crucial for developing effective prevention and treatment strategies. The aim of this study was to assess the effect of influenza virus coinfection with other viral pathogens on the odds of pneumonia diagnosis in children and adolescents, using data from a nationwide respiratory viral pathogen surveillance system.
Methods
A cross-sectional study was conducted using open influenza surveillance data from Mexico, focusing on cases of influenza confirmed by reverse transcription polymerase chain reaction (RT-PCR) among children (aged 9 years or younger) and adolescents (aged 10 to 15) in 2024. This timeframe coincides with the rollout of an RT-PCR-based viral panel for detecting coinfections [8]. The study population included all pediatric patients (aged ≤ 15 years) with influenza diagnoses recorded between January 1 and October 25, 2024, who met national surveillance criteria and had complete clinical, radiological, and epidemiological data in the audited system.
We extracted all data from Mexico's audited national influenza surveillance database, which contained standardized clinical records, laboratory-confirmed RT-PCR results, radiographic reports, and death certificates, when applicable. Our dataset included comprehensive demographic information (age, sex, and indigenous self-identification reported either by adolescents or parents/guardians for younger children), along with virological characteristics such as influenza subtype and the presence of respiratory viral coinfections. We also systematically recorded comorbidities, including obesity (defined as BMI Z-score ≥ +2, or ≥ +3 for children under 5 years), type 1 diabetes mellitus, asthma, immunosuppression from any cause, and hypertensive disorders.
The main outcome was pneumonia (no/yes), and it was considered positive if the diagnosis was confirmed through clinical and radiological criteria established by the World Health Organization (WHO) [11]. Patients without documented chest X-ray results or incomplete clinical/epidemiological data were excluded from the analysis.
Summary statistics were computed, and the effect of viral coinfections on the odds of pneumonia diagnosis was assessed using odds ratios (OR) and 95% confidence intervals (CI) from a multiple logistic regression model. The model accounted for potential confounders, including sex, age, influenza virus subtypes, self-identified Indigenous status, and personal history of obesity, type 1 diabetes mellitus, or immunosuppression. Since only publicly available data from the DGE of Mexico were analyzed for academic purposes, health research ethics committee approval was waived.
Results
Data from 2,057 children and adolescents were analyzed. Figure 1 presents the study profile. The mean age of participants was 7.1 ± 4.6 years, and nearly 6 in 10 participants were female (57.5%, n = 1,317/2,057). The A(H3) influenza subtype was the most identified, present in 40.4% of cases (n = 532/2,057) (Table 1).
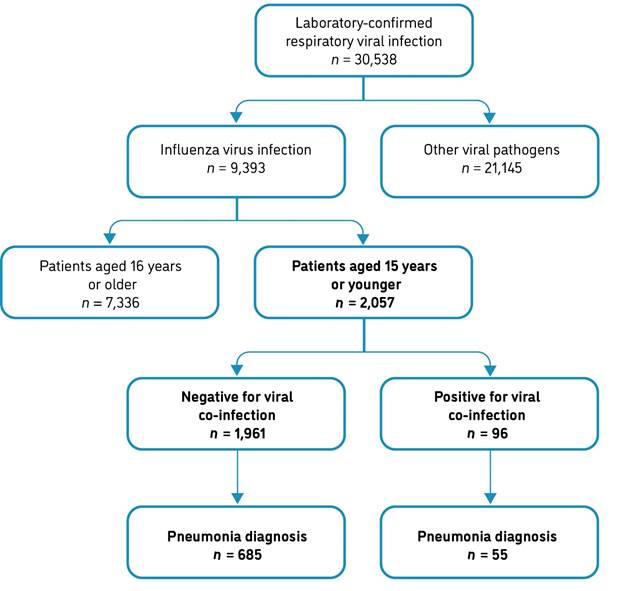
Notes. 1) Influenza virus and other viral infections were diagnosed using reverse transcription polymerase chain reaction (RT-PCR); 2) Pneumonia was confirmed based on clinical and radiological criteria.
Figure 1 Study profile, Mexico 2024
Table 1 Selected characteristics of children and adolescents included in the analysis, Mexico, 2024.
| Overall | Pneumonia diagnosis | p | ||
|---|---|---|---|---|
| (n = 2,057) | No (n = 1,317) | Yes (n = 740) | ||
| Sex | ||||
| Female | 1,182 (57.5) | 776 (58.9) | 406 (54.9) | 0.074 |
| Male | 875 (42.5) | 541 (41.1) | 334 (45.1) | |
| Age group (years) | ||||
| < 5 | 713 (34.7) | 363 (27.6) | 350 (47.3) | < 0.001 |
| 5-9 | 639 (31.1) | 428 (32.5) | 211 (28.5) | |
| 10-15 | 705 (34.3) | 526 (39.9) | 179 (24.2) | |
| Identified influenza virus subtypes | ||||
| A(H1N1)pdm09 | 444 (21.6) | 284 (21.6) | 160 (21.6) | 0.173 |
| A(H1) | 10 (0.5) | 6 (0.5) | 4 (0.5) | |
| A(H3) | 812 (39.5) | 532 (40.4) | 280 (37.8) | |
| B | 694 (33.7) | 444 (33.7) | 250 (33.8) | |
| A(non-subtyped) | 97 (4.7) | 51 (3.9) | 46 (6.2) | |
| Coinfection with other respiratory viruses | ||||
| No | 1,961 (95.3) | 1,276 (96.9) | 685 (92.6) | < 0.001 |
| Yes | 96 (4.7) | 41 (3.1) | 55 (7.4) | |
| Self-identified as an indigenous person | ||||
| No | 2,024 (98.4) | 1,300 (98.7) | 724 (97.8) | 0.131 |
| Yes | 33 (1.6) | 17 (1.3) | 16 (2.2) | |
| Personal history of: | ||||
| Obesity | ||||
| No | 2,025 (98.4) | 1,300 (98.7) | 725 (98.0) | 0.195 |
| Yes | 32 (1.6) | 17 (1.3) | 15 (2.0) | |
| Type 1 diabetes mellitus | ||||
| No | 2,046 (98.5) | 1,312 (99.6) | 734 (99.2) | 0.198 |
| Yes | 11 (0.5) | 5 (0.4) | 6 (0.8) | |
| Asthma | ||||
| No | 1,947 (94.7) | 1,249 (94.8) | 698 (94.3) | 0.620 |
| Yes | 110 (5.4) | 68 (5.2) | 42 (5.7) | |
| Immunosuppression (any cause) | ||||
| No | 2,002 (97.3) | 1,296 (98.4) | 706 (95.4) | < 0.001 |
| Yes | 55 (2.7) | 21 (1.6) | 34 (4.6) | |
| Hypertensive disease | ||||
| No | 2,050 (99.7) | 1,313 (99.7) | 737 (99.6) | 0.704 |
| Yes | 7 (0.3) | 4 (0.3) | 3 (0.4) | |
Notes. 1) Counts and relative frequencies (%) are presented, along with the p-value from the chi-squared test; 2) Indigenous self-identification was determined based on reports by adolescents or, in the case of children, by their parents or legal guardians; 3) Body mass index Z-scores were used to identify obesity in children and adolescents, defined by a Z-score of +2 or higher, or +3 for children under 5 years old.
Coinfections with other respiratory viruses were recorded in 96 participants (4.7%). Among patients with coinfections, the following viral pathogens were detected (in descending order of frequency): enterovirus/rhinovirus (25 cases), adenovirus (19 cases), respiratory syncytial virus (14 cases), parainfluenza 3 (9 cases), and non-subtyped influenza A (8 cases). SARS-CoV-2 was identified in 6 cases, and influenza A(H3) was detected in 3 cases. Parainfluenza 1, coronavirus 229E, and metapneumovirus each accounted for 2 cases. Rare detections (1 case each) included influenza A(H1N1)pdm09, influenza B, coronavirus OC43, coronavirus HKU1, parainfluenza 4, and bocavirus.
Figure 2 shows the symptom onset dates of enrolled patients stratified by coinfection status. The majority of influenza cases occurred during the first quarter of the year (January-March).
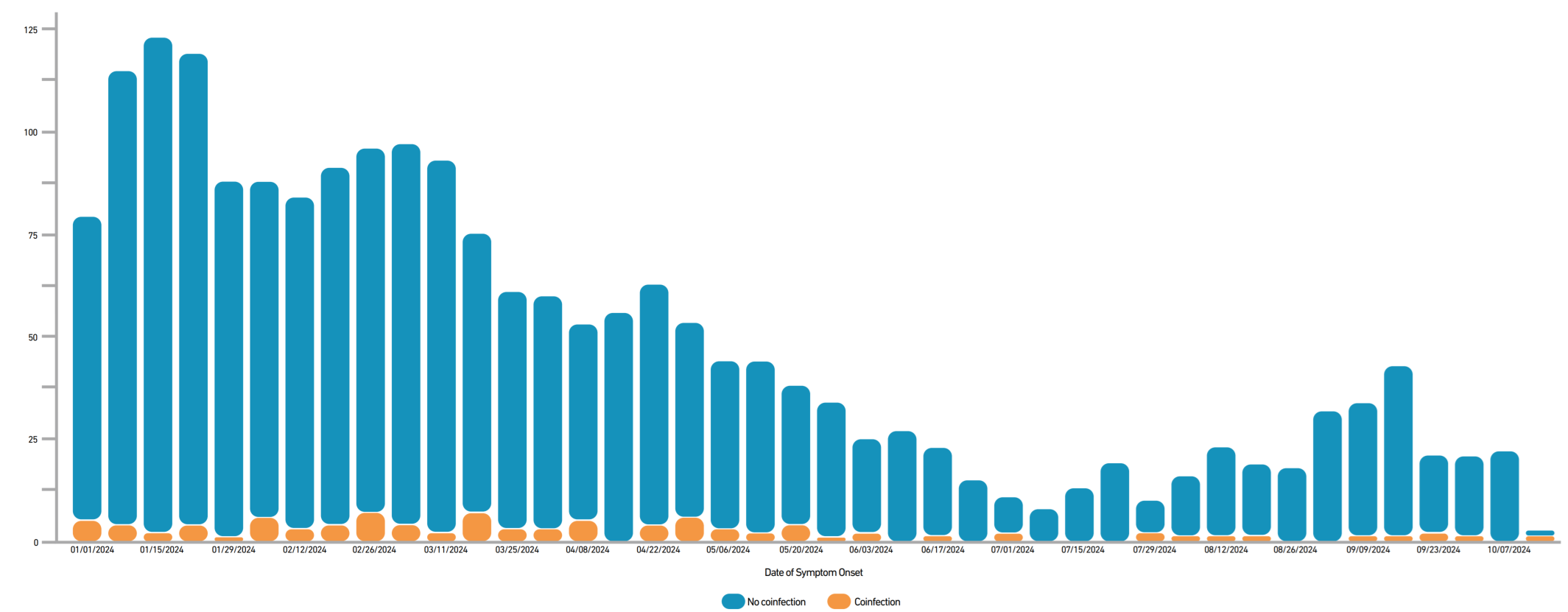
Figure 2. Symptom onset dates of enrolled patients stratified by viral coinfection status, Mexico 2024.
The overall prevalence of pneumonia in the study sample was 36.0% (n = 875/2,057). As shown in Table 1, coinfection was more frequent among patients with pneumonia versus those without pneumonia (7.4% vs. 3.1%, 𝑝 < 0.001). Among participants with coinfections, 90.7% required hospitalization, a proportion higher than observed in non-coinfected patients (65.5%, 𝑝 < 0.001).
Pneumonia patients were younger, with a higher proportion of those under 5 years old (47.3% vs. 27.6%, 𝑝 < 0.001), and had a greater prevalence of immunosuppression (4.6% vs. 1.6%, 𝑝 < 0.001). A total of 48 deaths were registered, 43 of them (89.6%) in children and adolescents with pneumonia. The overall prevalence of coinfection in patients with a fatal outcome was 8.3%.
In the multiple logistic regression model, coinfection was associated with a 95% increase in the odds of being diagnosed with pneumonia (OR = 1.95, 95% CI 1.27 - 3.00). Compared to adolescents aged 10-15 years, children aged 5 - 9 years (OR = 1.48, 95% CI 1.16 - 1.89) and those under 5 years (OR = 2.86, 95% CI 2.27 - 3.60) were also more likely to receive a pneumonia diagnosis. A personal history of immunosuppression (due to any cause) significantly increased the odds of pneumonia (OR = 2.97, 95% CI 1.68 - 5.27). Obesity was also significantly associated (OR = 2.24, 95% CI 1.07 - 4.71). No other significant associations were found. See Table 2.
Table 2 Factors associated with the odds of pneumonia diagnosis, Mexico 2024.
| OR (95% CI), p | ||
|---|---|---|
| Bivariate analysis | Multiple analysis | |
| Sex | ||
| Female | 1.00 | 1.00 |
| Male | 1.18 (0.98 - 1.42), 0.074 | 1.18 (0.98 - 1.43), 0.080 |
| Age group (years) | ||
| 10-15 | 1.00 | 1.00 |
| 5-9 | 1.45 (1.14 - 1.84), 0.002 | 1.48 (1.16 - 1.89), 0.001 |
| < 5 | 2.83 (2.26 - 3.55), < 0.001 | 2.86 (2.27 - 3.60), < 0.001 |
| Identified influenza virus subtypes | ||
| A(H1N1)pdm09 | 1.00 | 1.00 |
| A(H1) | 1.18 (0.33 - 4.26), 0.797 | 0.88 (0.24 - 3.21), 0.850 |
| A(H3) | 0.93 (0.73 - 1.19), 0.581 | 0.97 (0.76 - 1.25), 0.838 |
| B | 0.99 (0.78 - 1.28), 0.996 | 1.10 (0.85 - 1.42), 0.474 |
| A(non-subtyped) | 1.60 (1.03 - 2.49), 0.037 | 1.41 (0.89 - 2.24), 0.142 |
| Coinfection with other respiratory viruses | ||
| No | 1.00 | 1.00 |
| Yes | 2.50 (1.65 - 3.78), < 0.001 | 1.95 (1.27 - 3.00), 0.002 |
| Self-identified as an indigenous person | ||
| No | 1.00 | 1.00 |
| Yes | 1.69 (0.85 - 3.36), 0.135 | 1.48 (0.73 - 3.01), 0.274 |
| Personal history of: | ||
| Obesity | ||
| No | 1.00 | 1.00 |
| Yes | 1.58 (0.79 - 3.19), 0.199 | 2.24 (1.07 - 4.71), 0.033 |
| Type 1 diabetes mellitus | ||
| No | 1.00 | 1.00 |
| Yes | 2.14 (0.65 - 7.05), 0.209 | 2.46 (0.68 - 8.85), 0.169 |
| Immunosuppression (any cause) | ||
| No | 1.00 | 1.00 |
| Yes | 2.97 (1.71 - 5.16), < 0.001 | 2.97 (1.68 - 5.27), < 0.001 |
Note 1. Abbreviations: OR, odds ratio; CI, confidence interval.
Note 2. 1) Unconditional logistic regression models were used to estimate OR with 95% CI; 2) Estimates from the multivariable model were adjusted for all variables listed in the table; 3) Body mass index Z-scores were used to identify obesity in children and adolescents, defined by a Z-score of +2 or higher.
Discussion
Our findings suggest that coinfection with respiratory viral pathogens in pediatric influenza patients may increase pneumonia risk. After adjusting for sociodemographic characteristics and comorbidities previously linked to pneumonia risk, coinfection was associated with a higher likelihood of pneumonia diagnosis (adjusted OR = 1.95, 95% CI 1.27 - 3.00). This aligns with prior studies demonstrating that viral coinfections can exacerbate clinical outcomes in respiratory illnesses [12,13].
The observed viral coinfection frequency of nearly 5% in pediatric influenza patients is consistent with some recent studies, though reported rates vary significantly depending on clinical setting and diagnostic methodology. Our estimate closely aligns with a 2014-2017 Spanish pediatric study reporting a 6.0% coinfection frequency [14] but is notably lower than a more recent study in which viral coinfections were detected in 18-26% of children with laboratory-confirmed influenza [15,16]. This variability likely reflects differences in regional viral circulation patterns and potential alterations in respiratory pathogen epidemiology following the COVID-19 pandemic [17,18].
The study's results indicate that younger children, particularly those under 5 years of age, are at a heightened risk for pneumonia, with an adjusted OR of 2.86 (95% CI 2.27 - 3.60). This finding is consistent with previously published studies identifying the vulnerability of this age group to severe respiratory illnesses [19].
The higher prevalence of pneumonia in younger children may be attributed to their developing immune systems, which are less capable of effectively combating multiple viral infections simultaneously [20]. Additionally, the presence of immunosuppression significantly increased the odds of pneumonia diagnosis (OR = 2.97, 95% CI 1.68 - 5.27), reinforcing that underlying health conditions can influence the severity of viral respiratory infections [21].
The viral pathogens identified in this study, particularly enterovirus, adenovirus, and RSV, are consistent with previous findings that document their prevalence in pediatric pneumonia cases [12,13]. The detection of these viruses in coinfected patients highlights the complexity of respiratory viral infections and the need for comprehensive diagnostic approaches that can identify multiple pathogens simultaneously. This is particularly important given that viral coinfections have been associated with more severe clinical manifestations and increased hospitalization rates [22].
We also observed an increased risk of pneumonia among children with obesity. This latter is recognized as a state of chronic low-grade inflammation that can impair immune responses, making individuals more susceptible to infections, including influenza and its complications [23,24]. The mechanisms by which obesity increases the risk of pneumonia during influenza include alterations in immune function, such as impaired antibody responses to vaccinations and reduced activation of T cells, which are crucial for fighting viral infections [25]. This was documented even when the obesity prevalence in the study sample (1.6%) was lower when compared to national estimates [26]; thus, this finding should bed with caution.
This research may be relevant in the context of Sustainable Development Goals (SDGs), specifically Goal 3: Good Health and Well-being, which aims to ensure healthy lives and promote well-being for all ages. The presented results emphasize the necessity of enhanced clinical practices, including the screening for coinfections. Even at low prevalence, viral coinfections can strain healthcare systems by increasing diagnostic complexity and elevating risks such as pneumonia and prolonged hospitalization, in clinically vulnerable children.
During the 2024 influenza season in Mexico, surveillance data indicated predominant circulation of influenza A(H3N2) and A(H1N1)pdm09 [27] and, mirroring the strain distribution observed in our study sample. This aligns with the 2023 - 2024 Northern Hemisphere influenza vaccine composition [28].
A major strength of this study is its large sample size of influenza patients, all confirmed through molecular testing. Additionally, these patients were screened for concomitant viral infections using RT-PCR. This robust methodology not only enhances the reliability of our findings but also allows for a comprehensive assessment of viral coinfections, providing valuable insights into their impact on pneumonia risk.
Limitations
A major limitation of this study is that the analyzed publicly available data do not include information on the influenza vaccination status of registered patients. While this data is recorded in the web-based system, it is not transferred to the anonymized public database.
In addition, although all 2,057 samples were screened for viral coinfections per surveillance protocols, our analysis relied on reported system data and thus cannot independently verify the completeness of testing procedures for every case. The audited surveillance system does not capture data on coexisting non-viral respiratory infections (e.g., bacterial or fungal), which may limit our understanding of the full spectrum of coinfections and their interactions with influenza on clinical outcomes.
Another limitation of using surveillance data is the risk of incomplete or inaccurate reporting. As previously described in other health-related events [29], discrepancies in reported cases can lead to an underestimation of the true incidence of diseases.
Variability in interpretation of chest X-rays across participating centers is indeed an important limitation to consider. While all centers followed standardized protocols for pneumonia diagnosis, differences in imaging availability and radiologist expertise may have influenced the consistency of findings.
Finally, epidemiological surveillance systems encounter challenges related to confounding factors that may influence observed associations. Factors such as underlying health conditions, socioeconomic status, and access to healthcare can all impact disease outcomes but may not be sufficiently controlled in the analysis. Aakjær et al. emphasized the importance of employing robust methodologies to account for these confounding variables in surveillance studies [30].
Conclusions
Our findings suggest that viral coinfections substantially increase the pneumonia odds in children with influenza, highlighting an important clinical challenge. From a clinical and epidemiological perspective, the increased pneumonia odds underscores the major relevance of two complementary approaches: routine influenza vaccination, and systematic coinfection screening to guide appropriate management. Together, these measures could significantly improve outcomes for pediatric patients.

