











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Electronic sports (esports) are a form of digital sports whose main aspects are facilitated by electronic devices such as mobile phones, computers, and consoles [1,2]. The popularity of esports has grown rapidly and spread globally [3], including Indonesia, with the number of players reaching 52 million in 2021 [4]. In recent years, esports has also been increasingly recognized as an official competition, such as in the Hangzhou 2022 Asian Games, which featured eight games, which included FIFA, the Asian Games version of PUBG Mobile, Arena of Valor, Dota 2, League of Legends, Dream Three Kingdoms 2, Hearthstone, and Street Fighter V [5,6]. In addition, the gaming industry is projected to continue to experience significant growth, with market revenues estimated to reach $455.60 billion by 2024 [7]. This global trend is also reflected in the rising number of national and international esports tournaments, which attract thousands of spectators and offer prize pools of up to millions of dollars.
This global trend is also reflected in the rising number of national and international esports tournaments or events, which attract thousands of spectators and offer prize pools of up to millions of dollars [8-10]. However, behind this growing popularity, there is increasing concern about its health impacts, particularly musculoskeletal disorders such as neck and back pain, as well as psychological issues like stress and sleep disturbances, which can negatively affect players’ quality of life and career sustainability [11-13]. Previous studies have found the prevalence of pain in esports players, with the most commonly affected areas being the neck (40%), followed by fingers (38%) and head (32%). Pain was also reported in the lower back (20%) and upper back [14], as well as in the shoulder by 49.4% [15].
Musculoskeletal disorders in esports players are generally caused by activity characteristics such as long playtime, digital game addiction, and non-ideal craniovertebral angles due to poor neck posture [16,17]. Long playtime will cause increased strain on the back muscles and hips and over-compression of the intervertebral discs [18,19]. Most esports players spend 3-10 hours per day playing games, and previous studies have shown that playtime of more than 35 hours per week increases eightfold the risk of experiencing musculoskeletal symptoms such as wrist, lower back, shoulder, elbow, and finger pain [2,20].
Esports players who experience digital game addiction tend to play excessively, resulting in repetitive movements of more than 500 times per minute [21]. These activities can cause spasms and inflammation in the finger and hand muscles, increasing the risk of musculoskeletal disorders such as carpal tunnel syndrome, De-Quervain's tenosynovitis, and epicondylitis [22]. In response, the World Health Organization (WHO) included digital game addiction behavior as a gaming disorder in the International Classification of Diseases (ICD-11) in 2018 [23]. In addition, esports players often maintain unergonomic postures with non-ideal craniovertebral angles, such as bowing their heads toward the game screen, triggering a forward head posture that increases the risk of musculoskeletal disorders [24,25]. Previous studies have shown the prevalence of forward head posture in 55.6% of female and 44.4% of male mobile gamers [26], as well as in esports players in Makassar with an average craniovertebral angle of 41.59°, which, although classified as, has caused mild strain on the neck muscles [27].
Although several studies have investigated musculoskeletal disorders in esports players [2,14,28,29], research integrating the correlations between digital game addiction, playtime, and craniovertebral angle with musculoskeletal disorders remains limited. However, theoretical perspectives suggest that these three factors may be correlated with the risk of musculoskeletal disorders. Most previous studies have focused on prevalence without explaining the causal correlation between the main risk factors [9,30]. A more comprehensive understanding is needed to support the development of effective intervention strategies, both in curative and preventive contexts. Unlike previous studies, this research involves a sample of esports enthusiasts, including amateur, semi-professional, and professional players and different gaming platforms (mobile, computer, and console), which allows for a more comprehensive understanding of the variations in musculoskeletal disorders that have not been extensively explored. This study aims to analyze the correlation between digital game addiction, playtime, and craniovertebral angle and musculoskeletal disorders in esports players in Indonesia. The study is expected to be baseline for developing prevention strategies, improving player performance, improving quality of life, and extending players' careers in the competitive world of esports.
Method
Design and Participants
This article adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement [31]. An observational design with a cross-sectional approach was employed to analyze the condition of esports players in Indonesia. The study aimed to analyze the correlation between digital game addiction, playtime, and craniovertebral angle (independent variables) and musculoskeletal disorders (dependent variable). Data were collected simultaneously at one point in time without intervention or follow-up with the respondents. This research was approved by the Research Health Ethics Commission (KEKP) of the Faculty of Health Sciences, Muhammadiyah University of Surakarta and received an Ethical Feasibility Letter No.625/KEPK-FIK/X/2024.
This study employed a non-probability sampling method using a convenience sampling technique to recruit esports enthusiasts who met the inclusion criteria. This technique was selected for its accessibility in reaching active esports players across various competitive levels and gaming platforms. Such an approach facilitated the collection of relevant data aligned with the study’s context and objectives [32]. In this study, the term esports enthusiast refers to individuals actively engaged in competitive gaming, categorized as follows: (1) amateur players, those who play recreationally without participating in tournaments; (2) semi-professional players, those who actively participate in esports tournaments but are not under professional contracts; and (3) professional players, those affiliated with professional esports teams, holding official contracts, and regularly competing at national or international levels. Participants were drawn from various gaming platforms, including mobile, computer, and console.
The research population consisted of esports enthusiasts in Indonesia. Since the population size was unknown, the sample size was calculated using the Lemeshow formula, with a 5% margin of error and a proportion of 31.3% [32], which represents the most commonly reported site of musculoskeletal pain -the back region- among esports athletes. As a result, a minimum sample of 329 respondents was obtained. The forms were distributed in eight provinces: Central Java, East Java, West Java, North Borneo, East Borneo, Bengkulu, Jambi, and Lampung. A total of 415 esports players were willing to fill out the research questionnaire. After data screening, 338 respondents who fit the inclusion criteria were included. Inclusion Criteria: 1) 16-30 years old; 2) male and female gender; 3) status as an esports enthusiast, defined as an individual actively engaged in competitive gaming activities, whether recreationally or in formal tournaments, across various levels of participation (amateur, semi-professional, professional) and platforms (mobile, computer, or console); 4) actively practicing or playing video games every day for more than six months; 5) and willing to be a respondent. Exclusion Criteria: 1) have a history of previous musculoskeletal injuries such as scoliosis, herniated nucleus pulposus, entrapment of vertebral nerves, and fractures of fingers, wrist, hand, elbow, shoulder, or back within the past six months; 2) medical disorders such as neurological disorders and autoimmune diseases.
To minimize potential biases and confounding variables related to musculoskeletal disorders, exclusion criteria were established based on medical conditions that directly affect the musculoskeletal system. Musculoskeletal symptoms were assessed using a questionnaire that specifically evaluated complaints experienced during, after, or as a result of gaming within the past 12 months, thereby reducing the influence of temporary health conditions or unrelated physical activities. The questionnaire also collected data on occupation and education level to identify potential involvement in physically demanding activities outside of esports. Although a convenience sampling technique was employed, efforts were made to include a diverse range of respondents across different levels of participation and gaming platforms to enhance representativeness and reduce selection bias. To ensure data accuracy, the researcher provided assistance during questionnaire completion when needed and used an Indonesian-language instrument to improve clarity and comprehension.
Procedure
Prior to the current study, a trial was carried out on 10 respondents to ensure that the research instrument could be understood correctly and aligned with the research objectives. The research was conducted through virtual and in-person meetings from October to December 2024 using a virtual form platform. Digital game addiction and playtime data were collected online through the form. Craniovertebral angle measurements were taken offline to ensure the accuracy of the photographs. If offline measurement was not possible, participants were asked to upload photos online according to the guidelines and examples provided in the form. Inappropriate photos were reviewed, and participants were contacted for correction. The data were not included in the analysis if there was no response.
Measurement of musculoskeletal disorders and correlated factors in esports Players
Musculoskeletal disorders were measured using the Indonesian version of the Nordic Musculoskeletal Questionnaire (NMQ), which has validity between 0.501-0.823 and reliability (α = 0.78) [33] by adding the context of gaming to the question: “Have you ever felt aches, pains, or discomfort in any of the following body parts in the past 12 months: upper neck, lower neck, back, waist, buttocks, shoulders, upper arms, elbows, forearms, wrists, hands, pelvis, thighs, knees, lower legs, or ankles?” The level of impairment in each body part was rated using a scale: 1 (no impairment), 2 (mild), 3 (moderate), and 4 (severe). The cumulative impairment scores were then categorized into four risk levels: 28-49 as (low risk), 50-70 as (moderate risk), 71-91 as (high risk), and 92-112 as (very high risk). In this study, video game addiction is defined as a form of behavioral addiction characterized by a compulsive or repetitive urge to engage in excessive gaming, thereby impairing an individual’s social, emotional, or academic functioning [34]. To identify the level of addiction among participants, the Indonesian version of the Video Game Addiction Test (VAT) was used. This instrument consists of 14 statements rated on a 5-point Likert scale (0 = never to 4 = very often) and has demonstrated strong validity and reliability (KMO = 0.861; Cronbach’s α = 0.846; factor loading = 0.344-0.747) [35]. Scores were classified as follows: 0-14 = Normal (non-problematic), 15-28 = Mild (possibly unproductive gaming habit), 29-42 = Moderate (some degree of addiction), and 43-56 = Severe (significant gaming addiction) [36]. Playtime was measured based on the duration of play in hours/day and classified as low (<3 hours/day), medium (3-7 hours/day), and long (>7 hours/day) [37]. The craniovertebral angle was determined by measuring the angle made between the horizontal line drawn from the cervical spinous process 7 to the ear tragus [38], using the Kinovea application (ICC 0.920-0.995) and marking the cervical spinous process seven and the ear tragus. Classification of craniovertebral angle (normal ≥ 50°), (mild group 45.5°-49.9°), (moderate-to-severe group < 45.5°) [39].
Statistical analysis
The research data were processed using the IBM SPSS Statistics 24 application through several stages of testing. First, samples were checked for normality of distribution using the Kolmogorov-Smirnov method. Based on the normality test results, the data showed a non-normal distribution (p < 0.05), so the analysis was carried out using non-parametric methods. The testing stages included (1) univariate analysis to describe data characteristics, (2) bivariate analysis using Spearman's rank correlation test to evaluate the relationship between independent and dependent variables, and (3) multivariate analysis using an ordinal regression analysis to examine the correlation between independent variables and the ordinal-scaled dependent variable. The validity of the analysis results was tested using statistical indicators such as correlation coefficient, p-value, and pseudo R-squared to ensure model consistency and accuracy.
Results
The following flowchart provides a visual representation of the respondent eligibility assessment for this study as a guide to conducting statistical analysis of subjects who have completed the stages of the study, as shown in Figure 1.
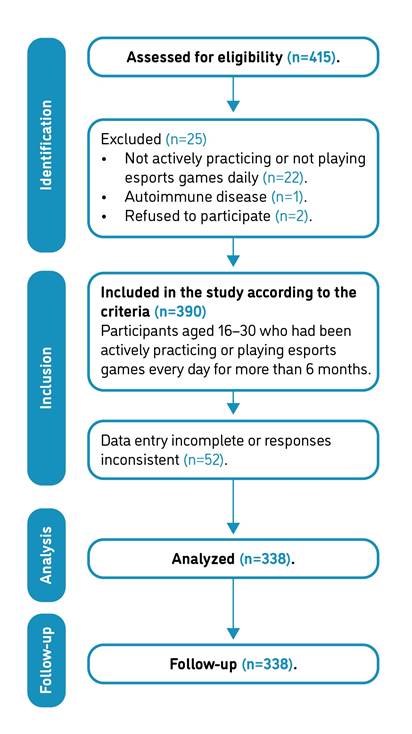
Descriptive analysis based on Table 1 indicates that the majority of respondents were aged 21-25 years (51.5%, n = 174), with an average Body Mass Index (BMI) of 22.07. Most were amateur (recreational) esports players (69.5%, n = 235), had been engaged in esports for ≥5 years (52.4%, n = 177), and predominantly used mobile devices (79.3%, n = 268). In terms of gender, male respondents constituted the majority (69.5%, n = 235), while females accounted for 30.5% (n = 103). Regarding digital game addiction, 26.3% (n = 89) were classified as normal, 55.6% (n = 188) as mild, 17.8% (n = 60) as moderate, and 0.3% (n = 1) as heavy, based on the Video Game Addiction Test (VAT) scores. For playtime, most respondents reported playing less than 3 hours per day (68.3%, n = 231), followed by 3-7 hours/day (28.7%, n = 97), and more than 7 hours/day (3%, n = 10), with an average playtime of approximately 3 hours/day. In terms of posture, 55.9% (n = 189) of respondents had craniovertebral angles within the normal category (≥50°). Most participants reported low-risk levels of musculoskeletal disorders (89.6%, n = 303).
Table 1 Demographic characteristics and playing patterns of Indonesian esports players.
| Demographic | Categories | N | (%) | Min | Max | Median | 𝐱 | S |
|---|---|---|---|---|---|---|---|---|
| Age (years) | 16-20 | 158 | 46.7 | 16 | 26 | 20.0 | 19.32 | 1.860 |
| 21-25 | 174 | 51.5 | ||||||
| 26-30 | 6 | 1.8 | ||||||
| BMI (kg/m2) | <18.5 | 76 | 22.5 | 14.6 | 44.5 | 21.1 | 22.07 | 4.603 |
| 18.5-22.9 | 149 | 44.1 | ||||||
| 23-24.9 | 32 | 9.5 | ||||||
| 25-29.9 | 66 | 19.5 | ||||||
| ≥30 | 15 | 4.4 | ||||||
| Esports participation | Amateur | 235 | 69.5 | NA | NA | NA | NA | NA |
| Semi-Professional | 85 | 25.1 | ||||||
| Professional | 18 | 5.3 | ||||||
| Duration of engagement | ≥ 6 Months | 81 | 24 | NA | NA | NA | NA | NA |
| ≥ 2 Years | 80 | 23.7 | ||||||
| ≥ 5 Years | 177 | 52.4 | ||||||
| Device | Mobile | 268 | 79.3 | NA | NA | NA | NA | NA |
| Computer | 43 | 12.7 | ||||||
| Console | 27 | 8.0 | ||||||
| Gender | Male | 235 | 69.5 | NA | NA | NA | NA | NA |
| Female | 103 | 30.5 | ||||||
| Digital game addiction | Normal | 89 | 26.3 | 0 | 44 | 20.0 | 19.41 | 9.377 |
| Mild | 188 | 55.6 | ||||||
| Moderate | 60 | 17.8 | ||||||
| Heavy | 1 | 0.3 | ||||||
| Playtime (hours/day) | <3 hours | 231 | 68.3 | 1.0 | 12.0 | 3.00 | 3.027 | 1.791 |
| 3-7 hours | 97 | 28.7 | ||||||
| >7 hours | 10 | 3 | ||||||
| CVA (degrees°) | ≥ 50 | 189 | 55.9 | 40 | 60 | 50.5 | 50.77 | 4.603 |
| 45,5-49.9 | 104 | 30.8 | ||||||
| < 45,5 | 45 | 13.3 | ||||||
| MSDs | Low risk | 303 | 89.6 | 28 | 62 | 36.0 | 37.31 | 7.736 |
| Medium risk | 35 | 10.4 | ||||||
| High risk | - | - | ||||||
| Very high risk | - | - |
Note. Key: BMI: Body Mass Index (underweight <18.5, ideal 18.5-22.9, overweight 23-24.9, obese I 25-29.9, obese II ≥30) CVA: Craniovertebral Angle (normal ≥ 50°, mild group 45,5°-49.9°, moderate-to-severe group < 45,5°) MSDs: Musculoskeletal Disorders, Playtime (low: <3 hours, medium: 3-7 hours, long: >7 hours), N: sample size, NA: not applicable, S: standard deviation, x ̅: mean.
Based on Table 2, the body part that experiences the most musculoskeletal disorders in e-sport players in Indonesia is back (65.1%), followed by the lower back (55%), upper neck (54.7%), right hand (48.8%), right wrist (47.3%), lower neck (46.2%), and buttocks (36.1%). The average musculoskeletal disorder was in the mild category based on the Nordic Musculoskeletal Questionnaire (NMQ) assessment.
Table 2 The degree of musculoskeletal disorders in specific areas was assessed using the 4-point Nordic Musculoskeletal Questionnaire (NMQ) (nil 1, mild 2, moderate 3, severe 4).
| No | Region | Case (N) | Prevalence (%) | Mild | Moderate | Severe | x | x |
|---|---|---|---|---|---|---|---|---|
| 2 | 3 | 4 | ||||||
| 2 | 3 | 4 | ||||||
| 1. | Upper neck | 185 | 54.7 | 134 | 47 | 4 | 2.30 | 2.31 |
| 2. | Lower neck | 156 | 46.2 | 95 | 54 | 7 | 2.44 | |
| 3. | Back | 220 | 65.1 | 133 | 70 | 17 | 2.47 | |
| 4. | Lower back | 188 | 55 | 112 | 59 | 15 | 2.45 | |
| 5. | Buttocks | 122 | 36.1 | 79 | 36 | 7 | 2.41 | |
| 6. | Right shoulder | 143 | 42.3 | 103 | 34 | 6 | 2.32 | |
| 7. | Left shoulder | 114 | 33.7 | 99 | 12 | 3 | 2.16 | |
| 8. | Right upper arm | 108 | 32 | 87 | 17 | 4 | 2.23 | |
| 9. | Left upper arm | 97 | 28.7 | 81 | 15 | 1 | 2.18 | |
| 10. | Right elbow | 60 | 17.8 | 53 | 7 | 0 | 2.12 | |
| 11. | Left elbow | 55 | 16.3 | 47 | 7 | 1 | 2.16 | |
| 12 | Right lower arm | 97 | 28.7 | 81 | 14 | 2 | 2.19 | |
| 13 | Left lower arm | 80 | 23.7 | 67 | 12 | 1 | 2.18 | |
| 14. | Right wrist | 160 | 47.3 | 114 | 43 | 3 | 2.31 | |
| 15. | Left wrist | 135 | 39.9 | 99 | 34 | 2 | 2.28 | |
| 16. | Right hand | 165 | 48.8 | 110 | 44 | 11 | 2.40 | |
| 17. | Left hand | 142 | 42 | 103 | 33 | 6 | 2.32 | |
| 18. | Pelvic | 88 | 26 | 70 | 14 | 4 | 2.25 | |
| 19. | Right thigh | 44 | 13 | 38 | 6 | 0 | 2.14 | |
| 20. | Left thigh | 38 | 11.2 | 33 | 5 | 0 | 2.13 | |
| 21. | Right knee | 3 | 0.9 | 3 | 0 | 0 | 2.00 | |
| 22. | Left knee | 3 | 0.9 | 3 | 0 | 0 | 2.00 | |
| 23. | Right lower leg | 1 | 0.3 | 1 | 0 | 0 | 2.00 | |
| 24. | Left lower leg | 1 | 0.3 | 1 | 0 | 0 | 2.00 | |
| 25. | Right ankle | 2 | 0.6 | 2 | 0 | 0 | 2.00 | |
| 26. | Left ankle | 1 | 0.3 | 1 | 0 | 0 | 2.00 | |
| 27. | Right feet | 3 | 0.9 | 2 | 1 | 0 | 2.33 | |
| 28. | Left feet | 3 | 0.9 | 2 | 1 | 0 | 2.33 |
Note. Key: The NMQ score reflects the severity of musculoskeletal symptoms in each body region: 1 = no discomfort, 2 = mild, 3 = moderate, 4 = severe. A higher score indicates more intense or frequent symptoms. Cumulative scores across all body regions were used to categorize musculoskeletal disorder risk levels: 28-49 = low risk, 50-70 = moderate risk, 71-91 = high risk, and 92-112 = very high risk.
Based on Table 3, the Spearman correlation test results show that digital game addiction (p = 0.00), playtime (p = 0.00), and craniovertebral angle (CVA) (p = 0.00) have a significant correlation with musculoskeletal disorders in Indonesian’s esports players. The r value shows that digital game addiction (r = 0.503) and playtime (r = 0.405) have a strong correlation, while the craniovertebral angle (r = -0.378) has a moderate correlation with musculoskeletal disorders [40]. The results of the ordinal regression analysis indicated that digital game addiction, playtime, and craniovertebral angle (CVA) showed significant correlations with musculoskeletal disorders (p = 0.000) in Indonesian esports players. Collectively, these three variables explained 32.7% of the variance in musculoskeletal disorders. The remaining 67.3% may be attributed to other factors not examined in this study. Among these, digital game addiction had the strongest correlation (p = 0.000), followed by craniovertebral angle (p = 0.001) and playtime (p = 0.038).
Table 3 Correlation and ordinal regression analysis of musculoskeletal disorders with digital game addiction, duration of gameplay, and craniovertebral angle.
| Variables | MSDs | ||||
|---|---|---|---|---|---|
| Spearman’s Correlation | Ordinal Regression | ||||
| Sig (p) | r | Sig (p) | R2 | ||
| Digital Game Addiction | .00 | .503 | .000 | .000 | .327 |
| Playtime | .00 | .405 | .038 | ||
| CVA | .00 | -.378 | .001 | ||
Note. * Significant at p < 0.05. Key: r: Correlation Coefficient, R2: Coefficient of Determination, CVA: Craniovertebral Angle, MSDs: Musculoskeletal Disorders.
These results indicate that high levels of game addiction, prolonged playtime, and craniovertebral angles suggestive of a forward head posture show a positive correlation with an increased risk of musculoskeletal disorders, particularly in the upper body regions. These findings emphasize the importance of concrete preventive measures, such as postural education, early ergonomic interventions, and raising awareness among esports players to mitigate the risk of musculoskeletal disorders.
Discussion
The findings of this study indicate that digital game addiction, playtime duration, and craniovertebral angle, reflecting a tendency toward forward head posture, show significant correlations with musculoskeletal disorders among esports players in Indonesia. Digital game addiction and playtime demonstrated strong positive correlations with musculoskeletal disorders, while a smaller craniovertebral angle, indicating forward head posture, demonstrated a moderate negative correlation [40]. Data analysis revealed that higher levels of addiction and longer playtime, along with a smaller craniovertebral angle, were associated with increased musculoskeletal disorder risk. Although this study focused on a limited set of variables, the results highlight their theoretical relevance in understanding the risk of musculoskeletal disorders. It is also important to consider that other theoretically relevant factors, such as physical activity level, stress, sleep quality, sedentary behavior, and seating ergonomics, were not included in this study and warrant further investigation [13,41,42].
Several factors not analyzed in this study are both theoretically and empirically relevant. Ndongo et al. [43] reported that poor sleep quality is associated with increased pain sensitivity (hyperalgesia) and impaired muscle recovery. Yadegaripour et al. [44] highlighted that the use of non-ergonomic equipment, such as chairs without lumbar support or monitors positioned too low, can lead to excessive tension in the back and neck muscles. Lack of physical activity outside gaming sessions has also been linked to reduced muscle endurance and flexibility, increasing the risk of injury due to prolonged static postures [45]. Additionally, Kha et al. [42] found that individuals with sedentary behavior tend to experience a higher prevalence of musculoskeletal disorders across various body regions. Theoretically, this may be explained by reduced blood flow to muscles and increased static muscle tension resulting from extended periods of sitting or lying down with low energy expenditure (<1.5 METs) [46]. Most musculoskeletal disorders in this study occurred in the back region, with a prevalence of 65.1%. Similar results were also found by Sinatra [5], who reported a prevalence of musculoskeletal disorders in the back of 66.7%. The findings of Lindberg et al. [30] also identified the back as the main complaint but with a prevalence of 31.3%. This difference in prevalence indicates the presence of complex risk factors, mainly due to the variety of playing devices, namely computers, consoles, and mobile devices, with the latter dominating at 79.3%. Meanwhile, Lindberg et al. [30] focused on computer-based devices, which may explain this difference, as computer use tends to involve static sitting positions with ergonomic adjustments, such as screens, chairs, and tables [47]. In contrast, mobile device use more often involves a slouched posture, excessive pressure on the hands, and additional strain on the neck [48].
The results of this study are in line with previous theories and findings that digital game addiction, playtime, and craniovertebral angle have a significant correlation with musculoskeletal disorders in esports players. Ahmed et al. [49] reported that digital game addiction on mobile increased the risk of musculoskeletal discomfort two to three times higher for neck pain (OR 2.84, 95% CI 1.49-5.36; p = <0.001), upper back (OR 3.75, 95% CI 1.97-7.12; p = <0.001), elbow (OR 1.78, 95% CI 0.93-3.40; p = 0.083), and wrist (OR 3.38, 95% CI 1.34-8.50; p = 0.010) and hand (OR 2.14, 95% CI 1.00-4.57; p = 0.049). In addition, the results of the research by Heidarimoghadam et al. [50] also showed similar results that social network addiction and digital game addiction could increase the risk of neck disorders with (OR 2.45, 95% CI 1.65, 3.6) and (0.58 ROC). Another thing is also supported by the theoretical aspect that digital game addiction will create impaired control over the game and can result in musculoskeletal disorders due to overuse, spasms, and inflammation in the muscles [22,51].
Consistency of findings was also seen in the playtime factor. Based on a systematic review conducted by Tholl et al. [17], 11 out of 16 studies showed a negative impact on the musculoskeletal system due to excessive playtime (> 3 hours/day), with odds ratios (OR) ranging from 1.3 to 5.2 for the risk of developing disorders. Previous studies have also reported a significant correlation between computer and mobile device use and neck pain (p<0.05) [51], as well as a significant association between playtime and musculoskeletal disorders (OR = 8.0; 95% CI 1.4-44.6; p = 0.018) [2]. Theoretically, this finding is supported by the mechanism that esports players with long playtime tend to experience muscle fatigue in the trunk area. This fatigue weakens the spinal support function, increasing compression on ligaments and intervertebral discs, ultimately leading to musculoskeletal pain and discomfort [14].
Previous research showed that a non-ideal forward craniovertebral angle or forward head posture correlated with neck pain levels of 0.323, although the study focused on a group of university students [52]. Similar results were also reported by Mahmoud et al. [25] through a systematic review and meta-analysis of eight studies, which showed a significant negative correlation between non-ideal craniovertebral angle and neck musculoskeletal pain (r = -0.55; 95% CI = -0.69 to -0.36) and disability (r = -0.42; 95% CI = -0.54 to -0.28). However, these results were based on a sample of adults in general, not esports players. Static positions maintained during prolonged gaming sessions may cause craniovertebral angle changes and affect the activation patterns of the sternocleidomastoid and upper trapezius muscles. This muscle activation imbalance can lead to discomfort and pain [53].
This study fundamentally differs from previous research as it involves a sample of esports enthusiasts across various categories, amateur, semi-professional, and professional. Additionally, it includes a diverse range of gaming platforms, such as mobile phones, computers, and consoles. In contrast, most prior studies have focused primarily on professional esports players [14,28], whereas investigating non-professional players is also essential to understand the potential health impacts of gaming habits outside structured environments [54]. Some relevant studies have examined specific devices [15,30], particular game genres [55], or player populations with distinct characteristics and behaviors [51]. These differences may influence ergonomic behaviors among esports players of different levels. Professional players are generally better trained and more aware of ergonomic posture and equipment use due to performance demands and guidance from coaches or teams [56,57]. On the other hand, amateur players may have less awareness of optimal posture and are more prone to musculoskeletal disorders due to non-ergonomic gaming habits [13]. These factors may also explain variations in digital game addiction levels, playtime duration, craniovertebral angles, and the prevalence of musculoskeletal disorders observed in this study.
The findings of this study have practical relevance in the fields of physiotherapy and esports health. Health promotion strategies focused on playing posture ergonomics and playtime management can be developed as preventive measures to reduce the risk of musculoskeletal disorders in esports players [12]. Physiotherapists play a key role in designing stretching and muscle-strengthening programs, particularly for the back, neck, hands, and wrists, and in conducting periodic evaluations of the craniovertebral angle to detect early postural risks. Personalized interventions, such as posture correction, core strengthening exercises, and pain management strategies, may enhance players’ performance and quality of life [58].
These findings also pave the way for future research, including intervention and longitudinal studies to assess the effectiveness of corrective exercises, digital ergonomic education, and long-term monitoring of musculoskeletal symptoms in the context of esports. Consequently, the scientific evidence generated can strengthen the role of physiotherapy in sustainable strategies for musculoskeletal disorder prevention among esports players. Furthermore, these results highlight the need for health policy development within the esports industry, including the use of ergonomic devices and the implementation of regular physical training programs. Education on proper posture and ideal gaming duration is particularly relevant for amateur players to prevent musculoskeletal issues in the future.
This study has a notable strength in its participant diversity, involving 338 esports enthusiasts across varying levels of competence (amateur, semi-professional, and professional) and using various gaming platforms, including mobile phones, computers, and consoles. This diversity reflects the real-world conditions of esports players and provides valuable cross-group perspectives. Furthermore, this study helps fill a gap in the existing literature by exploring the correlation between digital game addiction, playtime, and craniovertebral angle with musculoskeletal disorders, an area that has rarely been investigated comprehensively. These findings provide a broader initial understanding of potential risk factors for musculoskeletal disorders among esports players. The results are relevant for developing multidimensional intervention strategies in esports health, particularly in preventing musculoskeletal injuries among Indonesian esports players.
Limitations and Recommendations
The main limitation of this study is the imbalance in sample proportions, with most respondents coming from the amateur player group and mobile device users. This imbalance may be attributed to the use of a convenience sampling technique, which, although effective in providing access to participants from various levels and platforms, does not ensure an even distribution of the sample. This condition may influence the interpretation of results and limit the generalizability of the findings to the broader esports player population. Different device types, such as mobile, computer, and console, lead to varied playing postures, and the dominance of mobile users in this study may restrict the diversity of postural patterns represented. Moreover, this study did not account for potential confounding factors, including neck muscle strength and endurance, or the duration of screen exposure for non-gaming activities such as academic or occupational tasks, which may be correlated with the occurrence of musculoskeletal complaints.
Given the findings and limitations of the present study, future research is advised to employ a stratified random sampling method to ensure a more proportionate representation of respondents based on esports participation levels (amateur, semi-professional, professional) and types of gaming devices (mobile, computer, console). This approach is expected to yield broader and more generalizable insights into gameplay patterns, training intensity, and musculoskeletal injury risks. Subsequent studies should further investigate the correlations and differences across various levels of esports engagement and device types by examining the interaction between digital gaming addiction, gameplay duration, and craniovertebral angle. Additional factors, such as psychosocial conditions, physical activity levels, and rest patterns based on game genre, may also be correlated with musculoskeletal disorders and should be considered. Moreover, potential confounding variables, including neck muscle strength and endurance, as well as screen exposure from non-gaming digital activities such as studying or entertainment, should be carefully controlled. Longitudinal study designs are highly recommended to assess the long-term biomechanical and postural consequences associated with prolonged use of different gaming devices.
Conclusions
This study demonstrates that digital game addiction, playtime, and craniovertebral angle have significant correlations with musculoskeletal disorders among esports players. These findings align with the study’s objective of exploring the correlations between these three variables and musculoskeletal disorders. Although the results suggest potential roles for these factors, it is important to note that the findings are correlational and cannot be interpreted as causal relationships due to the cross-sectional nature of the study design. Additionally, musculoskeletal disorders in esports players are likely multifactorial, with correlating factors such as prolonged static postures, extensive use of mobile devices, and limited ergonomics education, particularly among amateur players. Other factors, including psychological stress, physical activity habits, and the type of gaming device used, should also be considered in future research.
These findings also emphasize the importance of ergonomics education, playtime regulation, and postural awareness in preventing musculoskeletal disorders. Physiotherapists play a vital role in maintaining player health by providing practical advice, such as encouraging regular stretching, avoiding prolonged forward head posture, and limiting daily gaming time, while also conducting postural assessments and delivering evidence-based preventive interventions. Coaches or team staff can support these efforts by organizing ergonomic training and developing balanced practice schedules. These recommendations are relevant for both healthcare providers and the broader esports industry in fostering healthier and more sustainable gaming environments.

