











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Obesity is an excess of body fat relative to height and is commonly evaluated using the Body Mass Index (BMI). According to established classifications, an adult is considered overweight if their BMI ranges from 25 kg/m² to 29.9 kg/m², while older adults are classified as overweight with a BMI between 27 kg/m² and 29.9 kg/m². An individual is categorized as obese if their BMI is equal to or greater than 30 kg/m² [1-3].
The World Health Organization (WHO) estimates that more than one billion adults worldwide are classified as overweight, with approximately 300 million considered clinically obese. In 2022, it was reported that approximately 16% of adults worldwide aged 18 and over met the criteria for obesity. The global prevalence of this condition increased by more than 100% between 1990 and 2022 [3]. In Colombia, in 2016, 56.4% of the youth and adult population was overweight [4].
This condition is multifactorial and affects multiple aspects of health, with significant variability in the presence of comorbidities [1]. Excess weight is a risk factor for the development of cardiovascular diseases, diabetes mellitus, dyslipidemias and other metabolic disorders. This is because adipose tissue, especially visceral tissue, contributes to an alteration called adipopathy, which generates a mild to moderate chronic inflammatory state in the body and is related to other comorbidities [2,5].
Although obesity is an independent risk factor for heart failure (HF), the incidence and prevalence of obesity and HF are high and it is common to find these conditions coexisting in the same patient. According to the WHO, it is estimated that worldwide there are around 26 million people suffering from heart failure and some studies have shown that 15-35% of patients with HF are obese and 30-60% are overweight [6,7]. Therefore, the objective of this study was to describe the prevalence and risk factors associated with excess weight in patients with heart failure.
Materials and methods
Type of study
This was an observational study that included a case-control analysis component: patients with excess weight were identified as cases and those without excess weight served as controls. Data were collected between June 2022 and May 2023. The research adhered to the ethical principles of the Declaration of Helsinki and Resolution 008430 of 1993 of the Colombian Ministry of Health and Social Protection. In addition, it was approved by the Ethics Committee of the National Sports School University Institution (Approval No. 17,115). The patients expressed their participation voluntarily by signing the informed consent form.
Population and sample
The population consisted of patients diagnosed with HF who entered a Cardiac Rehabilitation (CR) program at a clinic in the city of Cali, Colombia. A non-probabilistic convenience sample was carried out of all patients who entered the CR program.
Criteria
The inclusion criteria were patients with a diagnosis of HF determined by a cardiologist adopting the recommendations of the European Society of Cardiology (ESC) of the year 2021 [8] and patients who entered a CR program for the first time. Exclusion criteria included patients with New York Heart Association (NYHA) functional class IV and symptoms of discomfort or angina at rest, who had no clinical indication for CR.
Variables
Sociodemographic variables such as age, sex, marital status, health status, occupation, education level and socioeconomic status were considered (in Colombia, socioeconomic strata 1, 2, and 3 correspond to lower-income groups that receive subsidies for public utilities, whereas strata 4, 5, and 6 correspond to higher-income groups).
Clinical variables included risk factors, symptoms, anthropometry (body mass index, abdominal circumference, fat percentage, water percentage, and lean mass), left ventricular ejection fraction (LVEF), total cholesterol, high-density lipoprotein (HDL), low-density lipoprotein (LDL), and triglycerides.
Quality of life questionnaires were used, specifically the Minnesota Living with Heart Failure Questionnaire (MLFHQ) [9], the Depression Patient Health Questionnaire-9 (PHQ-9) [10], and the Hospital Anxiety and Depression Scale (HAD) [11]. The sit-to-stand test was used to assess lower limb endurance, while functional aerobic capacity was measured by the distance covered in the 6-minute walk test (6MWT) [12,13].
Procedure
Measurements were conducted at the onset of a CR program, and some sociodemographic and clinical variables were collected through a structured interview and review of medical history.
Data analysis
The database was initially processed using Microsoft Office® Excel® 2010 and then exported to Stata V.16 (Statistical Software for Data Science) for analysis.
Descriptive analysis was performed using frequency tables and percentages for qualitative variables. The Kolmogorov-Smirnov test was used for quantitative variables presented as means and standard deviations.
The adjusted odds ratio (OR) was calculated by logistic regression using the backward method, which allows the selection of variables with the lowest significance (p-value < 0.10). The following goodness-of-fit tests were used: Hosmer and Lemeshow, Cox and Snell's R-squared, and Nagelkerke's R-squared. Each model was compared to the previous one to identify the best explanatory model for excess weight based on the included variables.
Results
Initially, 328 participants were enrolled in the study; however, 25 individuals were excluded due to prior enrollment in a cardiac rehabilitation program, and an additional 3 individuals were excluded because they presented with symptoms of angina at rest during the initial assessment. Consequently, 300 participants were evaluated, including 152 individuals without excess weight and 148 individuals with excess weight. The participants had a mean age of 66 ± 12 years without excess weight and 60 ± 13 years with excess weight, were predominantly male (62.5% and 66.9%, respectively), and were covered by a health care contributory regime (98.0% and 97.3%), were in a common-law marriage (56.6% and 62.2%), and were from a middle socioeconomic stratum (56.4% and 58.1%) (Table 1).
Table 1 Sociodemographic variables of patients enrolled in the study.
| Variable | Without excess weight N=152 | With excess weight N= 148 |
|---|---|---|
| Age* | 66 ± 12 | 60 ± 13 |
| Sex | ||
| Male | 95 (62.5%) | 99 (66.9%) |
| Female | 57 (37.5%) | 49 (33.1%) |
| Health system | ||
| Subsidized | 3 (2.05%) | 4 (2.7%) |
| Contributory | 149 (98.0%) | 144 (97.3%) |
| Marital status | ||
| Non-stable union | 66 (43.4%) | 56 (37.8%) |
| Stable union | 86 (56.6%) | 92 (62.2%) |
| Occupation | ||
| Disability | 28 (18.4%) | 27 (18.2%) |
| Retired | 42 (27.6%) | 29 (19.6%) |
| Unemployed | 52 (34.2%) | 43 (29.1%) |
| Employed | 30 (19.7%) | 49 (33.1%) |
| Level of education | ||
| No formal education | 3 (2.0%) | 4 (2.7%) |
| Graduate degree | 6 (3.9%) | 6 (4.1%) |
| Completed primary education | 22 (14.5%) | 23 (15.5%) |
| Incomplete primary education | 9 (5.9%) | 8 (5.4%) |
| Completed secondary education | 48 (31.6%) | 57 (38.5%) |
| Incomplete secondary education | 10 (6.6%) | 7 (4.7%) |
| Technical education | 29 (19.1%) | 13 (8.8%) |
| Technologist certification | 8 (5.3%) | 11 (7.4%) |
| University education | 17 (11.2%) | 19 (12.8%) |
| Socioeconomic stratum | ||
| High | 28 (18.4%) | 19 (12.8%) |
| Medium | 83 (54.6%) | 86 (58.1%) |
| Low | 41 (27.0%) | 43 (29.1%) |
Note. * Values are reported as mean and standard deviation.
The main risk factors for patients without excess weight and with excess weight were history of smoking (98.7% and 97.3%, respectively), sedentary lifestyle (94.1% and 92.6%), hypertension (63.8% and 70.3%), and family history of related health conditions (53.3% and 56.1%). Patients without excess weight had a BMI of 22.0 ± 2.6 and a mean weight of 61.8 kg ± 9.7, whereas patients with excess weight had a BMI of 29.3 ± 3.8 and a mean weight of 79.5 kg ± 12.2. In addition, LVEF was 46% ± 13.2 in patients with excess weight and 43.2% ± 13 in patients without excess weight. Among patients without excess weight, 52 (34.2%) had reduced LVEF, whereas 66 (44.6%) had preserved LVEF (Table 2).
Table 2 Description of the clinical variables of the patients enrolled in the study.
| Variable | Without excess weight N=152 | With excess weight N= 148 |
|---|---|---|
| Risk factors | ||
| Dyslipidemia | 83 (54.6%) | 77 (52.0%) |
| Hypertension | 97 (63.8%) | 104 (70.3%) |
| Diabetes | 54 (35.5%) | 53 (35.8%) |
| Hypothyroidism | 26 (17.1%) | 29 (19.6%) |
| Postmenopausal | 50 (32.9%) | 36 (24.3%) |
| Current smoker | 2 (1.3%) | 4 (2.7%) |
| Ex-smoker | 150 (98.7%) | 144 (97.3%) |
| Family history | 81 (53.3%) | 83 (56.1%) |
| Sedentary lifestyle | 143 (94.1%) | 137 (92.6%) |
| Symptoms | ||
| Angina | 43 (28.3%) | 48 (32.4%) |
| Syncope | 3 (2.0%) | 4 (2.7%) |
| Dyspnea | 77 (50.7%) | 83 (56.1%) |
| Fatigue in lower limbs | 99 (65.1%) | 91 (61.5%) |
| Palpitations | 50 (32.9%) | 63 (42.6%) |
| LL edema | 35 (23.0%) | 40 (27.0%) |
| Claudication | 8 (5.3%) | 10 (6.8%) |
| Weight* (Kg) | 61.8 ± 9.7 | 79.5 ± 12.2 |
| Height* (m) | 1.7 ± 0.1 | 1.6 ± 0.1 |
| Abdominal circumference * (cm) | 88.1 ± 8.4 | 100.3 ± 10.1 |
| Fat* (%) | 24.4 ± 9.2 | 32.4 ± 7.7 |
| Water* (%) | 51.5 ± 6.1 | 47.8 ± 6.2 |
| Mass* (Kg) | 43.3 ± 8.9 | 45,8 ± 11,6 |
| LVEF* (%) | 43.2 ± 13 | 46 ± 13.2 |
| HFpEF | 51 (33.6%) | 66 (44.6%) |
| HFmrEF | 49 (32.2%) | 44 (29.7%) |
| HFrEF | 52 (34.2%) | 38 (25.7%) |
| Total cholesterol levels* | 167.6 ± 45.7 | 167.8 ± 41.2 |
| Out-of-target cholesterol | 35 (23%) | 28(18.9%) |
| HDL* (mg/dL) | 40.2 ± 9.4 | 37.6 ± 9.1 |
| Out-of-target HDL | 106(69.7%) | 114 (77.0%) |
| LDL* (mg/dL) | 84.3 ± 35.9 | 85.7 ± 28.4 |
| Out-of-target LDL | 38 (25%) | 42 (28.4%) |
| Triglycerides* (mg/dL) | 144.6 ± 54.2 | 151.7 ± 65.5 |
| Out-of-target Triglycerides | 48 (31.6%) | 68 (45.9%) |
| 6MWT * (meters) | 262.4 ± 66.7 | 271.3 ± 71 |
| Less<200 m | 20 (13.2%) | 12 (8.1%) |
| Sedentary | 144 (94.7%) | 139 (93.9%) |
| HAD anxiety* | 4.8 ± 3.4 | 4.4 ± 3.2 |
| HAD depression* | 3.3 ± 2.9 | 2.9 ± 2.8 |
| MLHFQ Total* | 34.6 ± 20.8 | 38.3 ± 24.2 |
| MLHFQ Physical* | 14.7 ± 10,0 | 15.7 ± 10.7 |
| MLHFQ Emotional* | 7.4 ± 6,2 | 8.2 ± 6.8 |
| PHQ 9* | 54 ± 4.8 | 6.4 ± 5.1 |
Note. * Values are reported as mean and standard deviation. BMI: body mass index; LVEF: left ventricular ejection fraction; 6MWT: 6-minute walk test; HDL: high-density lipoproteins; LDL: low-density lipoproteins. MLHFQ: Minnesota Living with Heart Failure Questionnaire; HAD: Hospital Anxiety and Depression Scale; PHQ-9: Depression Patient Health Questionnaire 9.
According to the HAD scale, patients without excess weight had a mean score of 3.3 ± 2.9, while patients with excess weight had a mean score of 2.9 ± 2.8. Regarding quality of life, the MLHFQ total score for patients without excess weight was 34.57 ± 20.8, while patients with excess weight had a higher mean score of 38.27 ± 24.2. Furthermore, the PHQ-9 showed a mean score of 5.38 ± 4.8 for patients without excess weight and 6.36 ± 5.1 for patients with excess weight (Table 2).
Significant associations were found between the variables analyzed and excess weight as the dependent variable. Patients younger than 65 years had a reduced likelihood of excess weight (OR = 0.47; CI [0.25-0.88]; P value = 0.01). Regarding LVEF, both LVEF of 40-49% (OR = 0.49; CI [0.26-0.92]; P value = 0.02) and LVEF <40% (OR = 0.40; CI [0.21-0.76]; P value = 0.00) were associated with a reduced likelihood of excess weight. In contrast, hypertension (OR = 1.81; CI [1.23-3.85]; P value = 0.01), elevated triglyceride levels (OR = 1.84; CI [1.08-3.13]; P value = 0.02), and a mild score on the PHQ-9 (OR = 1.91; CI [1.04-3.49]; P value = 0.03) were associated with an increased likelihood of excess weight (Table 3 and Figure 1).
Table 3 Explanatory model of excess weight based on sociodemographic and clinical variables.
| Variable | Odds Ratio | Confidence interval | P value |
|---|---|---|---|
| Sex (female) | 0. 89 | [0.51 - 1.57] | 0.70 |
| Age <65 years | 0.47 | [0.25 - 0.88] | 0.01 |
| Occupation - Disability | 0.50 | [0.23 - 1.09] | 0.08 |
| Occupation - Retired | 0.43 | [0.18 - 1.00] | 0.05 |
| Occupation - Unemployed | 0.56 | [0.25 - 1.24] | 0.15 |
| LVEF 40-49% | 0.49 | [0.26 - 0.92] | 0.02 |
| LVEF <40% | 0.40 | [0.21 - 0.76] | 0.00 |
| AH | 2.18 | [1.23 - 3.85] | 0.00 |
| Dyspnea | 1.47 | [0.83 - 2.63] | 0.18 |
| Fatigue | 0.71 | [0.39 - 1.28] | 0.26 |
| SBP >120% | 0.68 | [0.40 - 1.16] | 0.16 |
| Distance <200 meters | 0.49 | [0.19 - 1.25] | 0.13 |
| HAD depression | 0.51 | [0.21 - 1.25] | 0.14 |
| Triglycerides | 1.84 | [1.08 - 3.13] | 0.02 |
| PHQ-9 mild | 1.91 | [1.04 - 3.49] | 0.03 |
Note. LVEF: left ventricular ejection fraction; AH: arterial hypertension; AH: arterial hypertension; HAD: Hospital Anxiety and Depression Scale; SBP: systolic blood pressure; PHQ-9: Depression Patient Health Questionnaire 9.
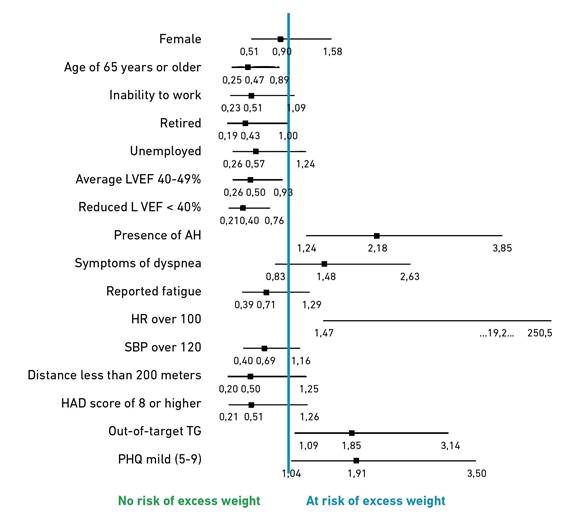
Note. LVEF: left ventricular ejection fraction; AH: arterial hypertension; SBP: systolic blood pressure; HAD: Hospital Anxiety and Depression Scale; TG: triglycerides; PHQ-9: Depression Patient health questionnaire 9. HR: heart rate.
Figure 1. Prevalencez of excess weight in people with HF and sociodemographic and clinical variables.
Discussion
The present study examined the prevalence and associated risk factors for excess weight in patients with heart failure. The results indicate that patients with hypertension, elevated triglyceride levels, and a mild score on the PHQ-9, which detects the possibility of presenting a depressive disorder, were significantly more likely to exhibit excess weight (p<0.05). Among the patients with excess weight, 70.3% had hypertension, and 45.9% had elevated triglyceride levels. These figures represent an increase of 6.5% and 14.3%, respectively, compared to patients without excess weight. Villar et al. [14] reported that the majority of heart failure patients with a BMI exceeding 25 had hypertension, with a prevalence of 71%, while Calle Crespo et al. [15] reported a prevalence of 63.5%.
The association between PHQ-9 scores and excess weight supports existing evidence linking depression with chronic inflammatory states, commonly observed in overweight individuals. Furthermore, cultural and social determinants, combined with the functional and health-related limitations associated with HF, adversely affect the quality of life of these patients [16,17]. According to Mascote et al. [18], the prevalence of depression in these patients is 4.1%. The present study shows that patients with excess weight scored higher on the MLHFQ than their counterparts without excess weight. These findings are consistent with a 2024 study of patients with HF, where patients who had higher scores on the PHQ-9 had lower adherence to rehabilitation programs [17].
In contrast, patients younger than 65 years and those with reduced LVEF demonstrated a lower likelihood of excess weight. This may reflect the tendency for body weight to increase with age. Although the results were not statistically significant, it was noted that male patients with HF exhibited a reduced probability of presenting with excess weight compared to female patients. In addition, the overall prevalence of a BMI of 25 kg/m² or greater increased significantly from 27.8% to 39.4% in females and 25.4% to 38.5% in males [19]. Currently, obesity is recognized as an independent risk factor for HF, as individuals with elevated BMI often have lower mortality rates, a phenomenon commonly referred to as the “obesity paradox” [20].
In this study, a lower likelihood of excess weight was observed among patients with reduced or midrange ejection fraction. This contrasts with findings from other contexts, where obesity is frequently associated with preserved ejection fraction (HFpEF) [1,19]. This discrepancy may be explained by the specific clinical and demographic characteristics of the Colombian population analyzed. Nevertheless, obesity remains a relevant factor associated with heart failure, especially due to its frequent co-occurrence with comorbidities such as hypertension, dyslipidemia, and insulin resistance. These conditions contribute to a chronic inflammatory state in which adipose tissue releases proinflammatory cytokines like TNF-α and IL-6, promoting endothelial dysfunction and the progression of heart failure [5,19]. Moreover, elevated levels of cortisol and catecholamines may exacerbate the hemodynamic burden and inflammatory response, ultimately affecting both the physical and psychological state of the patient, as well as treatment adherence and disease progression.
This study documented excess weight in 49.3% of patients, similar to that reported by Favini et al. (47.43%) [21]. The analysis indicated that excess weight (OR = 1.85; IC95%, 1.24-2.78) and increased abdominal circumference (OR = 2.16; IC95%, 1.10-4.24) were significantly associated with the occurrence of cardiovascular risk factors, as presented in this study, where the majority of patients had more than one cardiovascular risk factor [14,22,23].
The mean age of the study participants was 66 ± 12 years for the non-overweight group and 60 ± 13 years for the overweight group, with a predominance of males in both groups. Research suggests that excess weight generally increases with age until around 60 years of age in both sexes, a phenomenon closely related to sedentary behavior and independent of socioeconomic status [24]. These findings are similar to those reported by Calle Crespo et al. [15] in 2021, where 44.8% of participants were under 85 years of age, and most were male.
Clinical strategies should prioritize these risk factors to enhance quality of life and improve prognosis. This study highlights the relevance of identifying risk factors and clinical conditions linked to excess weight to design personalized prevention and management strategies. In addition, the importance of monitoring and managing excess weight in patients with HF is highlighted to significantly contribute to improving outcomes in this population.
Limitations and recommendations
The majority of participants were of medium socioeconomic status and covered by health care contributory regime, which limits the generalizability of the results to other populations. This demographic characteristic is due to the target population, which consisted of individuals eligible to participate in a cardiac rehabilitation program.
Conclusion
Patients with HF who are under 65 years of age and have a reduced or moderate LVEF are less likely to be overweight. Conversely, patients with HF who have comorbidities such as hypertension, elevated triglyceride levels, or a mild PHQ-9 score are more likely to be overweight. Early identification and intervention of these risk factors are essential to improve the care and quality of life of patients with HF.

