











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
In Mexico, obesity in adults has increased by 42.2% over the last 30 years, resulting in a major public health concern [1]. In 2022, the national survey reported that 36.9% of the Mexican adult population had obesity, with the rate being higher in women than in men [2]. Additionally, individuals with obesity have an increased risk of developing diabetes, hypertension, and dyslipidemia compared with those of normal weight [3,4]. As a consequence, there is an increasing prevalence of diabetes and hypertension in Mexico, which are some of the main causes of mortality. In 2022, the prevalence of diabetes was 18.3%, including 12.6% for diagnosed and 5.8% for undiagnosed diabetes [5], being the second cause of death and the first of disability in Mexico [6]. It was reported that 10.5% of the world’s population (536 million people) were living living with diabetes, and this figure is estimated to rise to 12.2% (783 million) by 2045 [7].
On the other hand, hypertension is the leading of cardiovascular mortality globally, and mortality from this condition has increased in recent years, reaching 10.8 million deaths in 2019 [8]. It has been estimated that the prevalence of hypertension in adults is 35.4% worldwide and the age-standardized prevalence in Latin America is between 20.7-56.4% [9,10]. In Mexico, the prevalence of hypertension in 2019 was 32.1% [9] and 70% of adults with this disease were unaware of their diagnosis in 2020 [11]. Given that hypertension may be asymptomatic initially or its symptoms can be confused with other diseases, its diagnosis is often delayed.
It has been estimated that in about a fifth of localities in Mexico, mostly dispersed rural areas, almost half of the inhabitants are Indigenous, resulting in 21.5% of the overall population [12]. In these populations, deficiencies in outpatient services, which are the entry point to the health system, represent a problem determined by social and cultural factors [13], in addition to the changing pattern of use of outpatient services due to the epidemiological transition [14]. Additionally, the Indigenous and rural Mestizo populations exhibit unique aspects due to genetic predispositions, socioeconomic factors, and distinct dietary patterns, which may increase their risk for metabolic disorders, including obesity, diabetes, and hypertension [15]. However, few investigations have explored the presence of cardiovascular risk factors in Indigenous Mexican populations, which have specific genetic and environmental factors [15,16]. Hence, the objective of this study was to describe the prevalence of obesity, diabetes, hypertension, and cardiovascular risk factors in the Indigenous populations of Northwest Mexico.
Method
This study was carried out in accordance with the Declaration of Helsinki and with the approval of the Research Ethics Committee of the Durango General Hospital of the Mexican Health Ministry (CI-HG450-24/165). Also, written and informed consent was obtained from all participants.
Subjects from different Indigenous groups and rural Mestizo populations of Northwest Mexico were eligible to participate in a cross-sectional study. A routine clinical examination was performed on enrolled men and nonpregnant women aged 18 years and older, with no upper age limit. The participants corroborated their indigenous ancestry and indicated that their parents and grandparents belonged to the same ethnic group. Additionally, the Indigenous ancestry of the studied groups was ratified by the analysis of 15 short tandem repeats (STRs) loci [17]. Demographic aspects, medical status, and dietary habits were evaluated. Trained personnel conducted the following procedures: administration of questionnaires, collection of medical history, and blood sampling and processing.
Definitions
Weight and height were measured using a standard stadimeter. Body mass index (BMI) was calculated as weight (kg)/height (m)2. Waist circumference was measured in centimeters at the umbilical level. Blood pressure was obtained using a mercury sphygmomanometer, following standard recommendations [18].
After 10-12 hours of overnight fasting, the biochemical parameters such as glucose, high-density lipoprotein-cholesterol (HDL-C), and triglyceride plasma levels were determined by enzymatic methods, according to the manufacturer’s procedures (BioSystems, Reagents & Instruments; Analyzer A15 ( Biosystems, Barcelona).
Obesity was defined by as a body mass index (BMI) ≥30 kg/m2 [19].
Diabetes was considered present if there was a diagnosis and/or ongoing antidiabetic treatment, or fasting plasma glucose ≥126 mg/dl at the time of the study [20].
Hypertension was defined by a previous diagnosis and/or the use of antihypertensive drugs, or values of systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg at the time of the study [21].
The cardiovascular risk factors were considered according to the following criteria: waist circumference ≥94 cm in men and ≥80 in women, fasting glucose ≥100 mg/dL or previous diagnosis of diabetes, systolic blood pressure (SBP) ≥130 mmHg or diastolic blood pressure (DBP) ≥85 mmHg or pharmacological treatment for hypertension, triglyceride concentrations ≥150 mg/dL, and HDL-C levels <40 mg/dL in men and <50 mg/dL in women [22].
Sample size
The sample size was calculated based on the prevalence of diabetes (18.3%) [5], considering a precision of 5%, the estimated sample size was 226 subjects.
Statistical analysis
Numerical variables are provided as mean ± standard deviation and categorical variables as proportions.
The prevalence of obesity, diabetes, and hypertension among Mexican Indigenous groups (Mestizos, Coras, Huicholes, Mexicaneros, Tarahumaras, and Tepehuanos) was presented as proportions.
Differences between the Indigenous groups (anthropometric and biochemical parameters) were determined by a one-way ANOVA test for numerical variables and the χ2 test for categorical variables.
The statistical significance was established with a p value <0.05 and 95% confidence interval (95% CI). The Statistical Package for the Social Sciences (SPSS) for Windows version 20.0 (SPSS Inc., Chicago, IL) was used for the statistical analysis.
Results
A total of 472 subjects were enrolled in the study, including Mestizos (n=48), Coras (n=73), Huicholes (n=93), Mexicaneros (n=74), Tarahumaras (n=81), and Tepehuanos (n=103). The ethnic groups showed significant differences in all parameters except sex (Table 1). The prevalence of obesity in the overall population was 11.2%, while specifically in Mestizos, Coras, Huicholes, Mexicaneros, Tarahumaras, and Tepehuanos was 35%, 18%, 7.5%, 9.4%, 7.4%, and 1.9%, respectively (Figure 1). For diabetes, the prevalence in the total population was 3.8%, which in Mestizos, Coras, Huicholes, Mexicaneros, Tarahumaras, and Tepehuanos was 2.0%, 7.8%, 0.0%, 4.0%, 9.8%, and 0.0%, respectively (Figure 1). Regarding hypertension, the prevalence in the overall population was 12.7, whilst in Mestizos, Coras, Huicholes, Mexicaneros, Tarahumaras, and Tepehuanos was 39%, 11.8%, 8.6%, 9.4%, 18.5%, and 1.9%, respectively (Figure 1).
Table 1 Anthropometric and biochemical characteristics of the Indigenous groups. n = 472.
| Mestizos | Coras | Huicholes | Mexicaneros | Tarahumaras | Tepehuanos | p-value | |
|---|---|---|---|---|---|---|---|
| N | 48 | 73 | 93 | 74 | 81 | 103 | |
| Age, years | 49.9 ± 14.3 | 47.7 ± 20.7 | 38.3 ± 17.0 | 38.5 ± 13.6 | 41.4 ± 12.9 | 36.3 ± 13.3 | <0.001 |
| Women, n (%) | 23 (47) | 50 (68) | 58 (62) | 44 (59) | 57 (70) | 69 (66) | 0.44* |
| Body mass index, kg/m2 | 28.4 ± 6.6 | 25.4 ± 5.3 | 23.9 ± 5.0 | 24.5 ± 3.4 | 23.7 ± 4.4 | 22.2 ± 3.3 | <0.001 |
| Waist circumference, cm | 101.8 ± 18.3 | 87.9 ± 12.9 | 89.4 ± 11.6 | 86.6 ± 9.8 | 83.2 ± 9.6 | 80.0 ± 8.3 | <0.001 |
| Systolic blood pressure, mmHg | 120.6 ± 14.5 | 119.7 ± 14.8 | 110.1 ± 18.9 | 113.6 ± 15.8 | 121.1 ± 18.1 | 104.9 ± 16.1 | <0.001 |
| Diastolic blood pressure, mmHg | 82.7 ± 11.8 | 77.6 ± 10.3 | 70.2 ± 11.2 | 73.1 ± 10.5 | 78.3 ± 9.6 | 69.0 ± 11.4 | <0.001 |
| Fasting glucose, mg/dl | 74.9 ± 20.9 | 89.6 ( 47.1 | 66.8 ± 13.8 | 86.4 ( 25.0 | 84.3 ± 15.6 | 78.6 ± 14.3 | <0.001 |
| HDL cholesterol, mg/dL | 59.3 ± 12.5 | 37.2 ( 10.7 | 44.7 ± 8.8 | 41.1 ( 11.2 | 42.0 ± 10.8 | 51.2 ± 12.6 | <0.001 |
| Triglycerides, mg/dL | 107.4 ± 79.1 | 177.4 ( 101.5 | 142.4 ± 75.7 | 176.7 ( 92.4 | 162.3 ± 89.9 | 110.6 ± 62.7 | <0.001 |
| Total cholesterol, mg/dL | 158.1 ( 39.9 | 164.9 ( 37.0 | 165.6 ( 31.9 | 184.9 ( 48.0 | 145.4 ( 30.8 | 154.0 ( 41.2 | <0.001 |
Notes. Values are expressed as mean ± standard deviation. P-value was estimated using one-way ANOVA with the Bonferroni post hoc test. * p-value was estimated using the χ2 test.
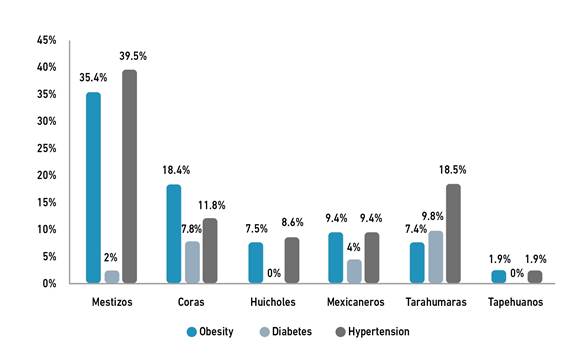
Table 2 presents the prevalence of cardiovascular risk factors among Indigenous groups. Specifically, the frequency of high waist circumference was elevated in all Indigenous groups, except among Tepehuanos. The prevalence of elevated blood pressure was greater in Mestizos, Tarahumaras, and Coras. According to hyperglycemia, it was higher in Coras, Mestizos, and Tarahumaras. With respect to hyperglycemia, higher rates were observed in Coras, Mestizos, and Tarahumaras. Concerning low HDL-C, the frequency was greater in Coras, Mexicaneros, and Tarahumaras (Table 2).
Table 2 Prevalence of cardiovascular risk factors among Indigenous groups. N=472.
| Mestizos N=47 | Coras N=73 | Huicholes N=93 | Mexicaneros N=74 | Tarahumaras N=81 | Tepehuanos N=103 | |
|---|---|---|---|---|---|---|
| High waist circumference, n (%) | 37 (78) | 44 (60) | 62 (66) | 45 (61) | 43 (53) | 36 (35) |
| Elevated blood pressure, n (%) | 30 (63) | 20 (27) | 16 (17) | 15 (20) | 26 (32) | 9 (9) |
| Hyperglycemia, n (%) | 7 (14) | 13 (18) | 1 (1) | 6 (8) | 9 (11) | 10 (10) |
| Hypertriglyceridemia, n (%) | 25 (53) | 37 (50) | 34 (36) | 39 (53) | 40 (49) | 18 (17) |
| Low HDL-cholesterol, n (%) | 23 (48) | 58 (79) | 56 (61) | 54 (73) | 54 (66) | 41 (40) |
Discussion
In the overall population, the prevalence of obesity and hypertension, as well as the frequencies of cardiovascular risk factors, were elevated in some Mexican Indigenous groups. To the best of our knowledge, this is the first study to report the prevalence of obesity, diabetes, hypertension, high waist circumference, elevated blood pressure, hyperglycemia, hypertriglyceridemia, and low HDL-C in Mestizos, Coras, Huicholes, Mexicaneros, Tarahumaras, and Tepehuanos.
Interestingly, the prevalence of obesity, diabetes, and hypertension in Mexican Indigenous populations was considerably lower compared with the last National survey, reporting 36.9% for obesity, 18.3% for diabetes, and 47.8% for hypertension [2]. These findings may be explained because some Indigenous communities remain isolated from urban areas by the distance, inaccessible roads, low income, traditional lifestyle, and language [23]. Given that they live in small and dispersed places of remote regions and retain traditional language, marginalization contributes to limited access to public health services and, therefore, timely diagnosis and treatment of non-communicable diseases, including hypertension, is deficient [23].
It is crucial to highlight that the vulnerability of the Coras and Tarahumaras to metabolic disorders is vinculated to several factors. In Mexico, these groups often live in conditions of poverty and marginalization with limited access to healthcare, which predisposes them to chronic degenerative diseases [23]. On the other hand, some indigenous communities have adopted lifestyles and dietary habits more closely aligned with urban areas, increasing their risk of developing diseases such as diabetes, obesity, and hypertension [24]. This trend is further exacerbated by the nutritional transition, marked by a decline in the consumption of traditional, fiber-rich foods and an increase in the intake of processed foods high in saturated fats and added sugars [25]. Social behavior patterns, which vary based on geographical location and educational disparities among different ethnic groups in Mexico [26,27], also play a central role in the prevalence of chronic diseases. Communities that maintain traditional practices and remain partially isolated tend to exhibit lower rates of metabolic disorders [28]. This could explain, at least in part, the relatively low prevalence of obesity, diabetes, and hypertension observed in the Tepehuanos group. Despite facing social disadvantages, this group displays protective factors, as evidenced by metabolic and biochemical differences that suggest a reduced risk of obesity [29,30].
Interestingly, the frequency of cardiovascular risk factors (high waist circumference, elevated blood pressure, hyperglycemia, hypertriglyceridemia, and low HDL-C) varied among the groups studied, which may be attributed to the interaction of genetic predispositions, dietary habits, lifestyle, and environmental factors specific to each group [31,32]. In this regard, Mestizos exhibited the highest frequencies of cardiovascular risk factors among the Indigenous communities, likely due to habits related to urbanization and lifestyle changes, such as high-calorie diets and sedentary behavior [29,30]. In contrast, Tepehuanos had the lowest prevalences, which may be attributed to protective factors such as a traditional diet low in fat and high in fiber, greater physical activity, and potential genetic differences that confer protection for the development of cardiovascular disease [33]. These variations between groups also highlight the critical role of ancestral genetics in developing metabolic diseases [34]. Specifically, the Mestizos and Huicholes presented significantly higher waist circumference values compared to other groups. However, the Coras and Mexicaneros showed an unfavorable lipid profile, characterized by lower HDL-C and elevated triglyceride levels. Interestingly, the prevalence of hyperglycemia was low across all the ethnic groups. From a biochemical perspective, central obesity, leads to excessive lipid accumulation in organs such as the liver and muscles, in addition to subcutaneous adipose tissue [35]. This phenomenon can cause an increase in fatty acids entering the mitochondria of these cells [36]. When mitochondrial oxidative capacity is exceeded, free fatty acids accumulate, contributing to the development of insulin resistance [35]. Normally, insulin facilitates glucose uptake by cells by binding to specific receptors on their membranes. However, insulin resistance impairs this function, disrupting normal glucose metabolism and reducing its storage as hepatic glycogen [37]. This abnormal glucose metabolism also causes an imbalance between fatty acid oxidation and absorption, which could explain the observed link between hypertriglyceridemia and reduced fasting glucose levels in these populations [38]. Additionally, another factor that may be related to these findings is the type of diet followed by these ethnic groups and the prolonged fasting periods they often undertake [39]. These habits could explain why blood glucose levels rarely rise, leading to a low prevalence of hyperglycemia [40]. However, this condition can increase the activation of hepatic and muscular glycolysis, mobilizing lipid reserves to maintain adequate glucose levels for the body’s basic energy needs [41], causing a reduction in subcutaneous fat with increased lipid mobilization to other tissues [40,42].
The main strength of our study is the inclusion of several Mexican Indigenous communities. Although our study provides valuable insights, several limitations should be acknowledged. First, the cross-sectional design precludes establishing a causal relationship between Indigenous groups and cardiovascular risk factors. Future longitudinal studies would be necessary to confirm our results, including exploration of genetic, dietary, and environmental factors, which could deepen our understanding of their influence on metabolic abnormalities. These studies could help uncover the specific biological and socio-cultural mechanisms driving the differences in metabolic health across different ethnic groups. However, it is important to note that not all ethnic groups were included; therefore, our results cannot be generalized to the whole Mexican population of the Northwest. Second, the influence of potential confounders such as diet and physical activity cannot be entirely excluded; however, each Indigenous group was analyzed separately for cardiovascular risk factors to minimize the influence of habits among communities.
Conclusions
The results of our study revealed that Mexican Indigenous groups exhibit a high prevalence of obesity and hypertension, as well as cardiovascular risk factors. Particularly, the prevalence of obesity was high in Mestizos and Coras, the prevalence of diabetes only was high in Tarahumaras, and the prevalence of hypertension was high in Mestizos, Coras, and Tarahumaras. Therefore, these findings warrant the need for further investigation into the underlying factors contributing to ethnic disparities. Understanding how genetic predispositions, lifestyle changes, and socio-economic conditions interact in these populations could lead to more effective prevention and treatment strategies.

