










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkColombia Médica
On-line version ISSN 1657-9534
Colomb. Med. vol.42 no.2 suppl.1 Cali June 2011
Factors associated with breastfeeding in children less than one year of age in the city of Cartagena, Colombia
Factores asociados con la lactancia materna en niños menores de un año en la ciudad de Cartagena, Colombia
Carmen Elena Díaz, MSc1, Rossana López, MSc2, Indira Herrera, Nurs3, Diana Arena, Nurs4, Carolina Giraldo, Nurs5, Laura Gonzáles, Nurs4
1Full Professor, Line Mental and Family Health, Group Care the Colective, Universidad de Cartagena, Cartagena, Colombia. e-mail: caeldimo_@hotmail.com2Full Professor, Line Women and Child Health, Group Women and Child, Universidad de Cartagena, Cartagena, Colombia. e-mail: Rolopsa@yahoo.com
3Nurse, Clinica AMI, Cartagena, Colombia. e-mail:indira_herrera0908@hotmail.com
4Nurse, Clinica Laura Carolina, Cartagena, Colombia. e-mail: diana0186@hotmail.com yayigo-9@hotmail.com
5Nurse, Clinica Cartagena del Mar, Cartagena, Colombia. e-mail:carolina.girado@hotmail.com
Received for publication June 25, 2009 Accepted for publication August 17, 2010
SUMMARY
Introduction:The practice of breastfeeding represents multiple benefits to children; however, several studies show that there has been a gradual loss of breastfeeding habits in industrialized and developing countries, mainly because the great diversity of types of milk. Additionalliy, there was the presence of biological and socio-cultural factors, which influence and modify this practice and generate a negative impact on the health of the infant population. In Colombia, in 2005, it was reported that the median duration of exclusive breastfeeding was 2.2 months and the median duration was 14.9 months total; likewise, the department of Bolivar reported a median slightly over a month.Objective: To determine the relationship between social and biological factors in the prevalence of exclusive breastfeeding in children under one year of age in Cartagena, Colombia.
Materials and methods: Cross-sectional study, the population consisted of the mothers of 23,109 children less than one year of age, the sample was 562 mothers. The probability sampling was stratified by clusters of three locations in the city where every neighborhood was a cluster. After selecting the neighborhood, a simple random sampling was conducted by city blocks. Mothers of children under one year of age were sought in their homes in the city blocks selected. The information was collected through the survey «Breastfeeding and complementary feeding» used by PROFAMILIA, demographic characteristics were demographic characteristics were also investigated.
Results: The median for breastfeeding was 2 months, social factors associated were: not using a feeding bottle (CI: 2.37-5.38), nuclear family membership (CI: 1.29-2.72), not being a mother head of household (CI: 0.27-0.62), and the biological factor showing association was temporary suspension of breastfeeding (CI: 0.23-0.70).
Conclusion: The duration of the exclusive breastfeeding practice among women turned out to be very short and the practice until the sixth month of life for their children was low. It was found that children born through caesarean section had a higher prevalence of maternal of maternal breastfeeding than those born vaginally.
Keywords:Prevalence; Breast feeding; Biological factors; Socioeconomic; Factors.
RESUMEN
Introducción: La práctica de la lactancia materna representa múltiples beneficios en los niños; sin embargo, diversos estudios muestran que ha existido una pérdida paulatina del hábito de la lactancia en los países industrializados y en vía de desarrollo, debido sobre todo a la gran diversidad de tipos de leche, además de la presencia de factores biológicos y socioculturales que influyen y modifican esta práctica y generan un impacto negativo en la salud de la población infantil. En Colombia, en el año 2005, se informó que la mediana de duración de la lactancia materna exclusiva fue de 2.2 meses y la duración mediana total 14.9 meses; igualmente, el departamento de Bolívar informó un poco más de medio mes.Objetivo: Determinar la relación de los factores sociales y biológicos en la prevalencia de la lactancia materna exclusiva en niños menores de un año en Cartagena.
Material y método: Estudio transversal con población constituida por las madres de 23,109 niños menores de un año, la muestra fue 562 madres. El muestreo fue probabilístico estratificado por conglomerados de las tres localidades de la ciudad, donde cada barrio representaba un conglomerado. Una vez seleccionado el barrio se realizó un muestro aleatorio simple por manzanas. En las manzanas que resultaron seleccionadas se buscaron en sus domicilios las madres de los niños menores de un año. La información se recolectó a través de la encuesta «Lactancia y alimentación complementaria» utilizada por PROFAMILIA; también se indagó acerca de las características sociodemográficas.
Resultados: La mediana de la lactancia fue 2 meses, los factores sociales que se asociaron fueron no usar biberón (IC: 2.37-5.38), pertenecer a familia nuclear (IC: 1.29-2.72), no ser madre jefe de hogar (IC: 0.27-0.62), y el factor biológico que mostró asociación fue suspensión temporal de la lactancia materna (IC: 0.23-0.70).
Conclusión: La duración de la práctica de lactancia materna exclusiva en las mujeres resultó muy corta y la práctica hasta el sexto mes de vida de sus hijos fue baja. Se encontró que los niños nacidos por cesárea tuvieron mayor prevalencia de lactancia materna que los nacidos por vía vaginal.
Palabras clave: Prevalencia; Lactancia materna; Factores biológicos; Factores socioeconómicos.
Maternal milk is considered the best and most important nutritional source for the child during the first six months of life. It is a unique process that in addition to supplying the ideal nutrition for lactating infants, contributes to their healthy growth and development. Among the numerous advantages attributed to this practice, there is the prevention of disease; furthermore, its protective role has been shown in infectious processes1, above all in gastroenteritis, respiratory infections, as well as in otitis and urinary infections2 and other general infections3. Likewise, it protects against chronic, non-infectious disease, especially those related to the metabolism and immune disorders (e.g., diabetes type I and II diabetes, allergies), as well as sudden infant death, hypertension, and some types of cancer3. Maternal breastfeeding diminishes the risk of malnutrition, including protein-energy malnutrition in low-income populations and overweight and obesity in low- and high-income populations3. It also prevents the risk of dental maloclusion4,5, and diminishes infant morbidity and mortality, promotes the mother’s health by reducing the risk of breast and ovarian cancer; and by increasing the interval between pregnancies6-8, it fosters in most women a sense of satisfaction when this practice is successfully carried out because of the mother-child bonding taking place.
Bearing in mind the benefits discussed, the International Pediatric Association (IPA) and the World Health Organization (WHO) have recommended exclusive maternal breastfeeding for at least six months, as well as mixed breastfeeding from the sixth month to two years of age7. Although this period was standardized for operational purposes, in this research exclusive breastfeeding is assumed as the act in which the lactating infant is only fed maternal milk and no other liquid or complementary nutrition except for drops or syrups consisting of vitamins, minerals, or medications until the moment the mother engages in breastfeeding.
In recent years, multiple studies have shown a gradual loss of the habit of breastfeeding in industrialized and developing nations, above all because of the great diversity of types of milks and their industrial derivations, as well as their mass commercialization, added to the presence of biological and socio-cultural factors that increase the likelihood of abandoning this practice; hence, becoming a social fact of incalculable projections for the future of infant populations8-10.
Romero et al.8 reported that 93.1% of the mothers began breastfeeding after childbirth, but this activity diminishes at six months by 55.7%. Likewise, Suárez et al. 9 indicated a 51.4% prevalence, decreasing to 14.9% at 90 days and to 8.7% at 120 days. In this sense, Zarzalejo et al.10 reported that 80% of the children received maternal breastfeeding and only 16% received it exclusively.
Among the socio-cultural and biological factors associated with the loss of the practice of maternal breastfeeding, there are: anxiety, post-partum depression11, breast pain, trauma to the nipple, loss of appetite by the baby, low production of maternal milk, and using a pacifier12,13. Among other factors reported, we found: inadequate family environment, poor schooling, family income, occupation, being a housewife, and having little information on maternal breastfeeding14.
In Colombia, the prevalence for exclusive and total maternal breastfeeding in spite of being on the rise remains low in comparison to international standards of 6 and 24 months. In 2005, the National Health and Demographics Survey (ENDS for its name in Spanish) informed that the median duration of exclusive maternal breastfeeding was 2.2 months and the median of total breastfeeding was of 14.9 months; the department of Bolívar reported slightly over half a month15. Currently, there is no information reporting on the incidence of the practice of exclusive maternal breastfeeding in the city of Cartagena in Colombia; the data found are related to a study conducted with mothers of children under the age of five from impoverished populations. Said study only had the participation of 14% of the mothers of the study’s total population; it reported high duration in the time of maternal breastfeeding (4.5 months)16.
Bearing in mind that infant health and nutrition are contemplated as priorities in the National Public Health Plan, setting the goal of increasing by a month the median duration of exclusive maternal breastfeeding, it becomes important to conduct this research because it will enable establishing the biological and social factors associated to the prevalence of exclusive maternal breastfeeding in women from Cartagena, which will allow designing strategies aimed at strengthening support programs for maternal breastfeeding.
MATERIALS AND METHOD
This was a cross-sectional study carried out in October 2008; targeting mothers of children less than one year of age in the city of Cartagena. The population was made up of the mothers of 23,109 children less than one year of age registered in the three sectors of the city of Cartagena de Indias.
The sample corresponded to 562 mothers of children less than one year of age who resided in the city of; bearing in mind a prevalence of maternal breastfeeding of 40%, a 4% margin of error and a 95% level of confidence.
The mothers of the children were selected through a probabilistic sampling stratified by clusters, where each neighborhood represented a cluster; these were selected in proportion to the total number of neighborhoods in each location. The number of women was proportional to the neighborhoods according to the general population of children less than one year of age. Once the neighborhood was selected, a random sampling was conducted by city blocks in each neighborhood; in the city blocks selected, the domiciles of the mothers with children less than one year of age were identified until completing the number of women per neighborhood to which the instruments were applied. The limitations of this study were related to the lack of interest of mothers from the upper (5th and 6th) socioeconomic strata in participating in the research, even when these strata were initially included in the sampling. Upon this negativity, these strata were replaced by the other strata.
Methods and instruments for data gathering. The participants were contacted in their homes, where they were made aware of the objectives and reach of the investigation and were also asked to sign an informed consent form. The information was collected via two structured surveys; the first was titled Breastfeeding and complementary nutrition (BCN) used in the PROFAMILIA health and demographics survey, which inquires on aspects like: number of months of exclusive breastfeeding, mixed breastfeeding, biological factors inherent to the child, the mother, and some social aspects; the second instrument inquired on the socio-demographic characteristics. The BCN survey was subjected to an appearance validity process through an evaluation by five experts, who assessed the questions in the instruments and made respective recommendations. Also, a test pilot was carried out consisting of the application of 50 surveys to the population object of study.
The variables considered in the study were: biological factors inherent to the child and the mother such as: illness, death of the child, suckling problems, use of baby bottle, prematurity, general illness of the mother, breast illness, parity, lack of lactic secretion, and problems with the nipple, and temporary suspension of the maternal breastfeeding. Social factors: family typology and structure, attendance to prenatal control, having received information and training on maternal breastfeeding, having designated spaces for breastfeeding, prior experience with breastfeeding. Other variables kept in mind were socio-demographic characteristics: age, schooling, income, socioeconomic level, occupation, and marital status, among others.
This study was classified as minimum risk for the individuals making up the population of the study according to that established in resolution 008430 of 1993 from the Colombian Ministry for Social Protection.
Procedure and information Aanalysis. For information processing, we used the Stata 9.2 statistical package; for the descriptive analysis, we found frequencies, percentages, means and standard deviation. For the Odds Ratio bi-variate and multivariate analysis a logistic regression was conducted; explicative variables were those with a value below 0.05 in the chi-square test.
RESULTS
Of the 562 mothers who participated in the study, it was established that 287 (51%) of their children were males and 275 (49%) were females, with a mean age of six months and a 3-month standard deviation. Most of the mothers interviewed were between 15-38 years of age, with a mean age of 23 years and a 5.5-year standard deviation; 8.4% had attended elementary school, 72.4% attended secondary school, 9.3% had technical schooling, and 9.9% had professional schooling. We also found that 69.4% were housewives, 13.2% students, 14.1% were employed, and only 3.4% were unemployed. It was noted that 17.6% of the mothers were single, 66.5% had common-law marriages, 14.2% were married, and 1.6% were divorced mothers.
The ages of the fathers ranged between 16 and 46 years with a mean age of 27 years and a 7.5-year standard deviation; regarding the level of schooling, 8.5% attended elementary school, 66.9% attended secondary school, 12.8% had technical schooling, and 12.5% had professional schooling. In 40.7% of the homes the income was below the minimum wage; with 86.4% being from low socioeconomic level.
Exclusive maternal breastfeeding. The median for exclusive maternal breastfeeding (EMB) was of two months, with 36.1% prevalence and a 2.4-month average. Regarding the percentage distribution of exclusive maternal breastfeeding, such diminishes as the child’s age increases; the study shows that only 30% practiced it during the first month-gradually decreasing every month until reaching 2.7% on the sixth month (Figure 1). Of all the children between 0 and 3 months of age 71.8% received EMB, 15% between 4 and 6 months, and 0.9% between 6 and 9 months, indicating that as they abandoned exclusive maternal breastfeeding they began complementary nutrition (cereals and other types of milks), as well as ingesting water prior to six months of age.

FACTORS ASSOCIATED TO EXCLUSIVE MATERNAL BREASTFEEDING
Social factors. Regarding attendance to prenatal control, 90.9% had attended; 62.9% attended postnatal control. As far as the information received by some family member on maternal breastfeeding, 72.5% reported having received information, 58.2% of the mothers received training from health personnel on EMB, while 39.7% reported not having received any training from health personnel. The factor on family structure revealed that 56% belonged to extended families and 44% to nuclear families.
With regard to the place of baby bottle initiation, 61% of the children began at home, 15% started at the hospital, and 24% had not begun with the baby bottle. In relationship to the perceptions of the mothers on the benefits of EMB for the infant, it was noted that 12% of the mothers responded that it offers more defenses against disease, creates immunity, fosters security, increases tenderness and love; 2% state that it is the best nutrition. Some 15.1% of the mothers said that EMB is less expensive than other milk formulas, 6.2% expressed that it enhances the relationship with the baby, 16.4% said it protects the mother against disease, 3.7% said that they did not have to prepare baby formula, 14.2% manifested that it avoids getting pregnant again and that it is less expensive than other milk formulas, 30.8% stated not knowing how it was beneficial. In consideration of the disadvantages of maternal breastfeeding (MB) for the mother, 5% responded that it damages the body figure, 3% said it is troublesome, 3% stated that it takes too much time.
In this study, 89.1% of the mothers were not heads of household. Regarding spaces for breastfeeding, 79.4% had spaces to carry out this activity, 49.3% had some experience with MB, and 82.7% took their children to growth and development controls.
BIOLOGICAL FACTORS
Conditions inherent to the child. Regarding factors inherent to the infant, it was noted that 7% of these were ill and 4% had suckling problems. About 82% of the children were full-term births and 18% were pre-term births; 59% were born via caesarian section and 41% were born through vaginal parturition. Nearly 94.8% were breastfed within the first 24 hours.
Conditions inherent to the mother. As for the number of children, it was observed that 47.8% of the mothers were multiparous and 52.3% were primiparous. With respect to problems arising during the breastfeeding period, 4% referred to problems with the nipple, 4% reported mastitis, 1% of the mothers presented general illness, and 1% of them said they had no milk. Temporary suspension of breastfeeding was reported by 26.1% of the mothers.
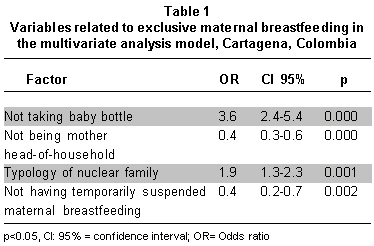
Twenty-eight variables were reported in the bi-variate analysis, of which seven showed association: having received information from a family member about maternal breastfeeding (p:0.002), not taking the baby bottle (p:0.0000001), belonging to a nuclear family (p:0.00078), followed by attending postnatal control (p:0.002) and not being a mother head-of-household (p:0.0048). The biological factor showing association was temporary suspension of maternal breastfeeding (p:0.00006). The previous variables were included in the logistic regression model to observe which were best adjusted; with the following resulting in order of explanation as greatly significant (Table 1).
DISCUSSION
In this study, the prevalence of exclusive maternal breastfeeding yielded low values (36.1%). But above the prevalence (13.5%) reported in Colombia for 200515. Likewise, a study conducted by Gamboa et al.17 in the department of Santander, Colombia reported low prevalence (20%) of EMB. In contrast to these studies, Arroyo et al.14 in México, found a prevalence of EMB 67.6% for infants six months old, higher than 50%, considered the goal by the WHO and UNICEF with programs supporting breastfeeding.
The present study revealed a median of two months of exclusive maternal breastfeeding, higher than that reported by the ENDS data, from the department of Bolívar with a median of 0.7 month of age15 and lower than the national median. The average 2.4-month duration of EMB resulted lower than that reported by Rodríguez and Acosta16, who reported an average 4.5-month duration of EMB. Also, Gamboa et al.17 reported an average of 5.7 months for EMB. Internationally, guidelines are being conceived to be adopted by all nations to increase the practice of maternal breastfeeding and, thus, contribute to decreasing infant malnutrition18.
With respect to educational level, 72.4% of the mothers had attended secondary school; however, this aspect did not show any association with the breastfeeding practice; in contrast, Pérez19, in a study of seven Latin American nations showed that women with the least schooling breastfed their children for the longest time, compared to mothers with advanced levels of schooling.
Regarding biological problems presented by the mothers during maternal breastfeeding, 22% had problems when breastfeeding, 7% reported a child’s illness, 4% complained about mastitis, 4% had problems with the nipple, and 4% had suckling problems. This was similar to a study conducted in the United States, which reported that 23% of the mothers presented problems with the baby when breastfeeding and 14% stated they had pain on the breasts. Another problem identified was the belief that the baby was not hungry or that the mothers were not producing enough milk (27%)12. Contradicting results found by this study; in the department of Santander it was found that 42.7% of the women with children less than one year of age had difficulties with breastfeeding, among which the study found; pain and cracking of the nipples (21.3%), mastitis (8%), inverted nipple (5.3%), insufficient milk production (5.3%)17.
The current study revealed that 66.5% of the mothers received information from several sources on maternal breastfeeding, and of these 62% engaged in EMB, 65.9% of these breastfed until the fourth month22, which permits inferring that receiving information will guarantee a high possibility of the mothers engaging in EMB for some period of time, an aspect that ratifies education as a protective factor for maternal breastfeeding. Prenatal controls are the optimal moments to receive true and scientific information to assure permanence of the mothers in the controls and good breastfeeding practices, which is why thefindings of this study are worrisome in that only 58% of the mothers received training on maternal breastfeeding and pregnancy controls. This does not permit availing of the opportunity of educating the mothers and creating awareness in them of the valuable practice, which goes against national policies of promoting maternal breastfeeding. The impact of education is not merely focused on the prenatal period; a study conducted in the city of Cartagena16 revealed that with 69% of the mothers who were advised on breastfeeding during the puerperium, 83% engaged in EMB. In this study, attending postnatal controls is positively associated (0R:0.58 CI: 0.40-0.83), becoming a factor in favor of maternal breastfeeding because it is during these controls that health personnel can reinforce education on the adequate nutrition required by the newborn.
This study showed correlation between EMB and receiving information from a family member (OR: 1.90 CI: 1.23-2.29). Likewise, Ingram and Jonson20 reported greater association in maintaining maternal breastfeeding (OR 37.2; IC 17.3, 80.2) when support is received from a mate By six weeks, in addition to these factors, the encouragement from a supportive partner, other family members and health professionals in enabling women to continue to breastfeed was found to show the largest associations with the maintenance of breastfeeding [(OR 37.2; CI 17.3, 80.2) for all three encouraging (327/817; 40% of breastfeeders) compared with no encouragement (67/817; 8% of breastfeeders)], other family members, and health professionals.
As far as the benefits of EMB for the child, 14% of the mothers responded that it offers more protection against disease, creates immunity, as well as giving the child security, tenderness, and love. Yaque21 also observed a higher percentage of maternal breastfeeding in mothers who were aware of the advantages of maternal breastfeeding for their offspring; they stated that it is «nourishment without rival» (21.9%), «avoids disease» (55%), and «aids the growth of teeth and bones» (12.3%). In the same vein, Gamboa et al.17 revealed that 97.9% of the mothers considered that maternal breastfeeding offers benefits for their children, such as: helping with the baby’s growth (44.7%), avoiding disease (43.6%), favoring the mother-child affective bond (7.4%), and others (4.3%).
Regarding the disadvantages of maternal breastfeeding for the mother, 5% responded that it ruined their figure, 3% said it was burdensome, 3% stated it took too much time. Similar data were reported in a study22 carried out in the department of Valle del Cauca where 18% of the mothers believe that breastfeeding does not offer benefits; on the contrary, they claim it generates decalcification, fatigue, drudgery, sagging breasts, and overall wear on the body. For this reason, it is vitally important to offer education during pre- and post-natal controls to allow mothers to understand the importance and benefits of maternal breastfeeding in the healthy growth and development of children.
The study revealed a relationship between EMB and birth by caesarean section (OR: 1.67 CI: 1.65-2.37), unlike that found by Chávez et al.23 who reported no association between EMB and mode of birth. This may be attributed to the fact that in the city of Cartagena, the hospitalization for women who have had vaginal childbirth is from 12 to 18 hours, while women who have given birth via caesarean section remain hospitalized over 24 hours, which enables reinforcing education on maternal breastfeeding. Additionally, the greatest number of women participating in this study belonged to socioeconomic levels I and II, and in most cases they are attended in institutions that favor maternal breastfeeding.
In the multivariate analysis, the variables that best explain the model were: not using the baby bottle was significantly associated with breastfeeding (OR: 3.57 CI: 2.37-5.38 p:0.000); these results agree with those reported by Rodríguez and Acosta16 who found that not using the baby bottle favored the time of EMB (OR: 1.29 IC: 1.06-1.59), as well as Barrios et al.13 in Brazil who observed that children who used a baby bottle stopped EMB by the end of the second month of life (OR: 2.63 CI: 1.70-4.06). In spite of the education offered by health professionals on promoting maternal breastfeeding, there is still low prevalence for this practice, which could be influenced by marketing in mass media by infant milk formula companies favoring the use of baby bottles.
With mothers who were head-of-household, we found a relationship between EMB and not being the head of the household (OR: 0.41 CI: 0.23-0.72). Espinosa24 in Nicaragua, found the same relationship (P: 0.05). Women who assume the family leadership are responsible for guaranteeing the basic needs of their families, which is why they are forced to generally seek work outside of the home, obligating them to leave their children in the care of a family member, friends, or elderly siblings; thus, favoring early weaning and early onset of complementary nutrition, or even the total suspension of breastfeeding.
The results obtained show that the nuclear family promotes maternal breastfeeding (OR: 1.82 CI: 1.26-2.63); likewise, a study conducted in México found that exclusive maternal breastfeeding is most common in nuclear families (59.2%)25. Similar in India (66%) families were nuclear26. Cultural practices are consolidated within the family nucleus, hence, promoting the practice of breastfeeding by replicating positive experiences, reinforced on the young girls through games with dolls in which they are taught to be caregivers.
With relation to suspending maternal breastfeeding, it was noted that 71% of the mothers had not suspended such, revealing a protective association for EMB (OR: 0.41 CI: 0.23-0.72); similarly, Barrios et al.13 determined that the main problems for suspending maternal breastfeeding were related to maternal problems (55.5%), trauma to the nipple (29.0%), and mammary regurgitation (19.5%) (OR: 1.57 IC: 1.02-2.41). Which could lead to partially or totally abandoning the maternal breastfeeding practice; thereby, requiring education and permanent accompaniment of the mother and her immediate family during pre- and post-natal controls. The education should be reinforced towards the most common problems during breastfeeding, paying attention to any sign and/or symptom that may affect this practice.
CONCLUSION
The duration of the EMB practice in women turned out to be very short with respect to current global and national recommendations. This study revealed the low percentage of women in Cartagena who kept to the practice until the child’s sixth month of life, which is considerably higher than that reported by the National Health and Demographics Survey (ENDS).
Social factors associated to exclusive maternal breastfeeding were: belonging to a nuclear family, not using a baby bottle, and not being a mother head-of household. The biological factor showing association with the EMB practice was the temporary suspension of maternal breastfeeding. With regards to children born via caesarean section, it was found that these were more prone to greater prevalence of maternal breastfeeding than those born vaginally.
Colombian legislation has norms that facilitate exclusive maternal breastfeeding for working women during the 86 days of maternity leave,and the breastfeeding practice until the sixth month of the child’s life. It should also be mentioned that legislation also contemplates the paternal inclusion in the María Law,as well as in projects seeking to extend the maternity leave; however, we still need further discussion and formulation of public policies to broaden coverage and State participation to solidify and reinforce this healthy and cost-effective practice, which in economic terms enhances diminished health costs. The practice can curtail costs by advancing in the early detection of illnesses like: acute diarrhea disease, acute respiratory infection, among others. Said initiatives may be aimed at subsidizing women who are heads of households during the post-natal period to enable their dedicating more time to breastfeeding, the generation of incentives through food bonuses for the lactating mother,protection to paternity to ensure that the father cannot be fired from work during the first six months of life of their children,the creation of a support network for breast feeders with the added value of conserving this practice within cultural terms.
Conflict of interest. None of the authors has conflicts of interest related to this study.
REFERENCES
1. Betrán AP, de Onís M, Lauer JA, Villar J. Ecological study of effect of breast feeding on infant mortality in Latin America. BMJ. 2001; 323: 303-6. [ Links ]
2. Marild S, Hansson S, Jodal U, Oden A, Svedberg K. Protective effect of breastfeeding against urinary tract infection. Acta Paediatr. 2004; 93: 164-8. [ Links ]
3. American Academy of Pediatrics Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics. 2005; 115: 496-506. [ Links ]
4. Labbok MH, Hendershot GE. Does breast-feeding protect against malocclusion? An analysis of the 1981 child health supplement to the National Health Interview Survey. Am J Prev Med. 1987; 3: 227-32. [ Links ]
5. Viggiano D, Fasano D, Monaco G, Strohmenger L. Breast feeding, bottle feeding, and non-nutritive sucking; effects on occlusion in deciduous dentition. Arch Dis Child. 2004; 89: 1121-3. [ Links ]
6. Lawrence AR, Lawrence MR. Lactancia materna: una guía para la profesión médica. 6a ed. Madrid: Elsevier Mosby; 2007. [ Links ]
7. International Pediatric Association. 26th International Congress of Pediatrics of Internationals Pediatrics Association. [fecha de acceso 19 de agosto de 2009]http://www1.ipa-world.org/IPAcongress/ [ Links ]
8. Romero M, Algaba S, Albar M. Prevalencia de la lactancia materna y práctica hospitalaria en las maternidades de Sevilla. Rev Metas Enferm. 2003; 59: 18-23. [ Links ]
9. Suárez P, Alonso JC, López AJ, Martín D, Martínez M. Prevalencia y duración de la lactancia materna en Asturias. Gac Sanit. 2001; 15:104-10. [ Links ]
10. Zarzalejo Z, García M, Álvarez M. Hábitos de alimentación en niños desnutridos menores de dos años en una comunidad urbano marginal. An Ven Nutr. 2001; 14:60-9. [ Links ]
11. Forster DA, McLachlan HL, Lumley J. Factors associated with breastfeeding at six months postpartum in a group of Australian women. Int Breastfeed J. 2006; 1:18. [ Links ]
12. Taveras EM, Capra AM, Braveman PA, Jensvold NG, Escobar GJ, Lieu TA. Clinician support and psychosocial risk factors associated with breastfeeding discontinuation. Pediatrics. 2003; 112: 108-15. [ Links ]
13. De Barros M, García M, Plácido M. Factores asociados a la situación de la lactancia materna exclusiva en niños menores de 4 meses en Botucatu, SP, Brasil. Rev Latino-Am Enfermagem. 2007; 15: 62-9. [ Links ]
14. Delgado-Becerra A, Arroyo-Cabrales LM, Díaz-García MA, Quezada-Salazar CA. Prevalencia y causas de abandono de lactancia materna en el alojamiento conjunto de una institución de tercer nivel de atención. Bol Med Hosp Infant. 2006; 63: 31-9. [ Links ]
15. PROFAMILIA. Salud sexual y reproductiva en Colombia. Encuesta Nacional de Demografía y Salud 2005. Bogotá: PROFAMILIA; 2005. [ Links ]
16. Rodríguez J, Acosta R. Factores asociados a la lactancia materna exclusiva en población pobre de áreas urbanas de Colombia. Rev Salud Publica. 2008; 10: 71-84. [ Links ]
17. Gamboa EM, López N, Prada GE, Gallo KJ. Conocimientos, actitudes y prácticas relaciona dos con lactancia materna en mujeres en edad fértil en una población vulnerable. Colomb Med. 2007; 38: 75-84. [ Links ]
18. May V, Mesa redonda: Políticas públicas y lactancia materna. Tema: Historia y actualidad sobre luchas y logros por la recuperación de la lactancia materna a nivel mundial. Conflictos de intereses y mercadeo de alimentos infantiles. Rosario: 35º Congreso Argentino de Pediatría; 2009. http://www.sap2.org.ar/35conarpe/ [ Links ]
19. Pérez Escamilla R. La promoción de la lactancia materna en era del SIDA. Rev Panam Salud Publ. 2001; 9: 357-61. [ Links ]
20. Ingram J, Johnson D. Greenwood R. Breastfeeding in Bristol: teaching good positioning, and support from fathers and families. Midwifery. 2002; 18: 87-101. [ Links ]
21. Yaque M, Castillo E, Praena M, Sancho C, Fernández A, Herrera C, et al. Factores relacionados con el inicio de la lactancia materna en nuestro medio: diferencias entre cuatro zonas básicas de salud. Rev Pediatr Aten Primaria. 2000; 2: 35-46. [ Links ]
22. Carvajal R, Cabrera. GA, Mateus JC. Conocimientos acerca de la lactancia materna en el Valle del Cauca, Colombia, 2003. Rev Fac Nac Salud Publica. 2003; 21: 27-41. [ Links ]
23. Chávez MA, Sánchez GR, Hantz IO, Peña OB. Causas de abandono de la lactancia materna. Rev Fac Med UNAM. 2002; 45: 54-7. [ Links ]
24. Espinoza H. The relationship between family structure and exclusive breastfeeding prevalence in Nicaragua. Rev Salud Publica Mex. 2002; 44: 499-507. [ Links ]
25. Garfias A, Márquez E, Moreno F, Bazán Castro M .Factores de riesgo maternos y familiares que influyen en el abandono de la lactancia materna. Rev Esp Med Quir. 2007: 12: 53-7 [ Links ]
26. Chudasama RK, Patel PC, Kavishwar AB. Determinants of Exclusive Breastfeeding in South Gujarat Region of India. J Clin Med Res. 2009; 1: 102-8 [ Links ]

