











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
1. Introduction
The Covid-19 pandemic has affected healthcare workers (HCW), outcomes and performance. This reality has been studied in private healthcare institutions with similar social context [1,2] but just little research has explored this situation in local public hospitals (30 beds or less) with the same sample. Mitigation measures imply interventions at individual and organizational levels. [3]
Due to Health Care National Office regulations [4], a cross-sectional study started on February 2021. Increasing psychosocial hazards were identified in 20 nurses of local hospital in Daule (Ecuador), exhibiting different leadership styles and moderate psychosocial work environment indicators. Research consistently supports the positive relationship between transformational leadership style and psychosocial work during biological crisis [5-7]. The hospital, placed to 43 km from Guayaquil, is currently serving 120,326 inhabitants (87,508 living in urban areas and 32,818 in rural zones) with 139 health workers (68.3% women and 31.7% men).
A possible relation between leadership styles (F1), psychosocial hazard perception (F2) and work climate (F3) could lead interventions empowering leadership behavior to employee well-being.
1.1. Conceptual framework
After Bass leadership dimensions (transformational, trans-actional and laissez fire) research [8], other works have emphasized the influence of leadership within healthcare organizational climate [9, 10]. Leadership in nursering is the ability to take care about other people need and transform performance and motivation in an organizational behavior standard [11].
Based on House’s Path-Goal Theory [12], Solano et al. [13] proposed the CAMIN-S: a path-Goal questionary to evaluate self-perception of leadership styles of nursing professionals an estimate a relationship with psychosocial risks. 4 leadership styles (directive, supportive, participative, and achievement-oriented) can be identified through 12 dimensions.
Psychosocial hazard perception (F2) refers to those conditions that directly affect the organization well-being and job performance during critical situations [14]. According to the research leaded by T. Meirum [15], previous works have revealed several psychological impacts on nurses. Job demands and job and personal resources theory [16] divided the psychosocial variable in two groups: job demands, including physical, psychological, social, or organizational aspects; and job resources, gathering the facilities that make employees meet their goals [17].
ISTAS21 [18] proposed a 7-step questionary to evaluate psychosocial risk in institutions having 50 workers or less, that is widely used in Ecuador (national regulatory frame- work does not require the use of specific instruments). The instrument gathers 5 dimensions: 1) psychosocial demands, 2) active work and skill development, 3) social support and leadership quality, 4) rewards, 5) double presence, and 19 categories.
Other works have demonstrated that leadership styles is positively associated with level of organizational commitment. A thematic analysis made by Broetje, S. et al. [19] identified three job demands and six job resources in the practice of nursing, most related with work climate aspects. Moreover Muhammad S. et al. [20] also demonstrated that work environment has a significant influence on employee's subjective well-being.
Work climate (F3) is a background to study and address characteristics influencing behavior in the workplace. Nurse subjective satisfaction with the working environment are well-known factors empowering nursing staff. [21]
To evaluate work climate, a questionary proposed by Guaminga [22] was used. The instrument has 21 categories grouped into 4 dimensions: 1) Collaboration; 2) Communications; 3) working conditions and 4) job satisfaction.
The aim of this study was to identify leadership determinants for nurses’ well-being and their influence on psychosocial work environment in local public hospital, by using data of cross-sectional studies from the same sample. A leadership model based in participatory virtual group strategy is proposed to enhance nurse’s well-being. The relation between hypothesis and expected results is depicted in Fig. 1.
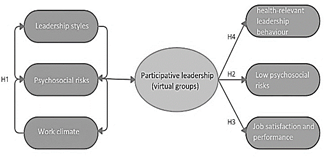
H1 Significant relationship between leadership styles and psychosocial risks exists.
H2 The leadership style in nursering produces significant differences in the dimensions of psychosocial risks.
H3 Participative leadership influences the dimensions of climate work.
H4 Participative leadership has a positive impact of the self-perception of leadership in nurses.
H0 There is no significant relationship among variables.
1.2. Team theory and social cognitive theory
Leadership can improve work performance in a reflexive way. The definition of Social Cognitive Theory (SCT) started in the 1960s by Albert Bandura [23], considering the interaction of personal states, characteristics, and external conditions within a context whether behavioral action will occur, meanwhile Reflexivity Theory explain leadership based on the work team perceptions of reality. [24]
Both theories have been successfully applied in social media research to reinforce the work team participative effect. [25].
1.3. The participative leadership and virtual groups
According to Castellano et al [26], "virtual team members interact primarily using technology, rather than face-to-face, and may be geographically dispersed". As a result, most professional employees now interact in virtual teams. [27]
Team collaboration is increasingly becoming virtual during the Covid pandemic and is expected to have post-pandemic impact in the long-term. Virtual interaction enhances work relationships through mentoring team dynamic initiatives [28], affecting various attributes of leadership and work climate in a public organization.
Currently, the role of leadership in the health and employee’s well-being has increased [29]. Virtual team strategy could improve the organizational climate through leadership based on recognition of achievement, effective interaction, information sharing and teamwork.
Functional Team Leadership Theory [30] requires bring together all participants to meeting team needs, tasks distribution and further instructions to enhance team effectiveness. The second phase implied control and supervision. Relationship-focused leadership facilitates the interaction among team members meanwhile task-focused leadership empowers effective task accomplishment [31], considering categories showing low or moderate perceptions.
1.4. The role of social media in self-perceived leadership
The power of social media rests in the scalability and participatory nature. Forte and Pires [32] illustrated the role of social media as a medium for self-expression and interaction. Abuhammad, M. and Mukattash, T. [33] highlighted the "nursering constructive role when acting as the first-line health provider, having a public awareness role and providing care for patients".
In the last years, three nodes about the interaction of nursing and social media have been identified [34]: social media as a tool for learning, social media promoting communication and social media conducting people’s behavior. Nurses used social media to gain government official information and share breaking news about COVID-19, and to support training and delivery for disease prevention. Moreover, social media enables the nurses to link with colleagues and share research findings and worries, even heroic self-representations during crisis. Finally, they also use social media for health education.
2. Methodology
On February 2021, a cross-sectional study design was started using ISTAS21, Work Climate and CAMIN-S instruments. A total of 60 forms were distributed (three for each participant) and fulfilled by the same sample after the intervention for comparison purposes. The Hospital is currently serving 120,326 inhabitants of Daule (87,508 living in urban areas and 32,818 in rural zones) with 139 health workers (68.3% women and 31.7% men). Instruments were given according to:
Initial questionnaire includes 8 items-demographic predictors related with sex, age, work activity, job roles, work- place and housing. The remaining sections contain 105 items as follows: 12 items-Leadership style (directive, supportive, participative and achievement-oriented), 69 items-Psychosocial hazard perception: 16 items-psychological demands, 19 items-skill development, 25 items-leadership quality, 8 items-reward and 4 items-double presence, and 23 items-work climate grouped into 4 dimensions: (a) collaboration; (b) communications; (c) working conditions and (d) job satisfaction. Items were measured by using 5-point Likert scale with categories ranging from 1="strongly disagree" to 5="strongly agree" based on items worded positively, so the higher score represents a strong perception of any variable. The instruments comprised 112 items, alpha = .903 (p-value≤ 0.05) [35].
A group of 20 nursing graduated professionals aged 25 to 34 years old (60%), 35 to 44 years old (20%), less than 25 years old (15%) and more than 54 years old (5%) exhibited moderate to high levels of psychosocial distress. 75% were female and 5% male, and 85% do operational activities and 15% performed mixed tasks. This group was chosen to implement the virtual group strategy.
Variants of leadership style were presented in the initial state: cooperative leadership (83%), directive leadership (83%), participative leadership (79%), collaborative leadership (72%).
Leadership strategies empowering nurse workforce included rewards, mentoring objectives and expectations, teaching managers to give support and guidance rather than instructions and providing a safe environment to say what they think and not feel attacked. [36]
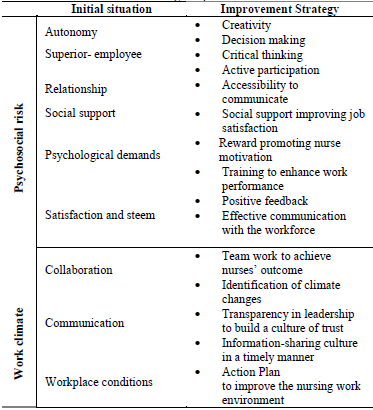
To create a healthy work environment, a new Facebook group page called “Teambuilding Hospital de Daule” was implemented to communicate ideas (relationship-focused leadership), and concerns and solutions (task-focused leadership) to the institution middle managers. Table 1 resumes the effective strategic planning. Rewarding positive actions of nurses, entertainment and lifelong learning, were also part of the strategy to enhance participative leadership in nurses.
A meeting with the nurse sample, the hospital head, the psychologist, and the occupational doctor was carried out to explain the participatory methodology and components (leadership style theory, critical thinking, decision-making, rewards among others). The initial process for the intervention is described below:
Signature of free, prior and informed consent by participants.
Sharing invitation link from the Facebook virtual platform to conform the "Teambuilding Hospital de Daule" group.
Sharing the Facebook group basic rules and additional information about activities.
2.1. Intervention: virtual group strategy
The challenge of social media is motivating the user engagement in online forums like the well-known Facebook (FB). FB posts and content were designed considering the Subjective Well-being Perception of users [37], Team Reflexivity Theory and Social Cognitive Theory [38]. Both theories promote shared task representation conducting team performance based on individual autocratic leadership control, influenced by environmental factors and the interaction with colleagues.
Activities were organized to enhance psychosocial dimensions and work climate emotional outcomes:
2.1.1. Communication dimension
Regular virtual meeting among team members and middle managers were scheduled to check all comments and suggestion made in a virtual form. Live audience was used.
2.1.2. Leadership dimension
Professional obligations and responsibilities within the hospital were displayed in the home page. Each participant was invited to post a summary of weekly strategies to accomplish the work settings. A short-form video reinforcing job tasks and skills were also part of the activity.
2.1.3. Satisfaction and self-esteem dimension
The effects of organizational rewards on participative strategy were considered. A small list of relevant attitude questions about coworkers was available for all participants. Workers having the highest score received an incentive determined by performance levels.
2.1.4. Social support dimension
According to Shearer, D.A. [39] and Shearer, D.A. et al. [40] supervisor support and coworkers support may be the most important factors affecting workers public service motivation. Completion of FB activities to hindrance stress were included into the methodology with presential meetings for birthdays and contingent rewards to maximize their effectiveness on employees.
2.1.5. Psychological demands dimension
A QR code printed on the walls was used to facilitate communication with psychologist and share information through a mobile phone. When work-related problems, stress and anxiety become evident, the ’panic button’ allow them to reach occupational psychologist to schedule a virtual appointment for healthcare.
2.1.6. Cooperation dimension
As mentioned previously, healthcare professionals were forced to answer short questions after watching interactive video lessons reinforcing job tasks and skills on EdPuzzle app. Answers were public and ready to receive constructive coworkers’ feedback.
Colleagues were also responsible for rewarding to those who maximize their performance goals on daily activities.
3. Data analysis
3.1. Instruments application
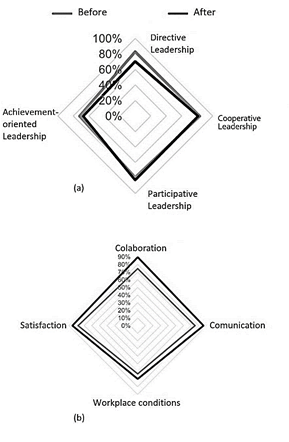
As mentioned previously, Cooperative Leadership (83%) and Directive Leadership (83%) were the main leadership styles leading nurses before the intervention. Participative Leadership (79%) and Collaborative Leadership (72%) were secondary roles (alpha = .903; p-value < 0.05). A perceived new transformational attitude in superiors is believed to have influence on directive leadership perception and subsequently the level of organizational commitments among nursing staff is increased. [41]
The same instrument validated the results after two months of virtual group strategy implementation. CAMIN-S questionnaire analysis (alpha = .911; p-value < 0.05) showed difference in self-perceived leadership styles. A positive Participatory (83%) and Collaborative (81%) performance is depicted in Fig. 2(a). Directive leadership (70%) decreased after the intervention, while achievement-oriented leader- ship remained low (68%). Participative and collaborative leadership address team needs that result from collaborating virtually, based in two common categories: relationship-focused and task-focused styles, influencing team performance. [42]
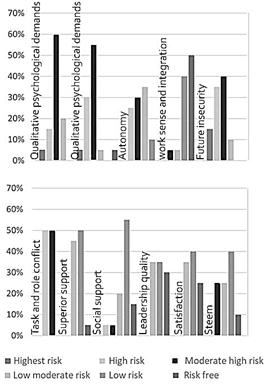
Negative dimensions of psychosocial risk before the intervention showed a moderate 60% of high risk in quantitative psychological demands (QnPD). Highest risk and high risk undergo 5% and 15% respectively. Recent insights [43] suggest that high demands for cognitive, emotional work and work peace have a positive impact in the nursing routine performance. Social support had a positive
impact in a successful strategy to enhance autonomy, and self-perception of participative and collaborative leadership as depicted in Fig. 3. FB virtual group promoted cognitive connections with learning activities, and emotional work with social relationship and leadership.
Source: the authors
Figure 3 Assessment of Psychosocial Risks according to COPSOQ- ISTAS, in the previous stage
The qualitative psychological demands (QcPD) assessed hiding emotions, hard decision-making and emotional stress exhibited high risk (30%) and moderate high risk (55%). Insecurity in the future: very high risk (15%), high risk (35%) and moderate high risk (40%) due to uncertainty in task assignments. The task-role conflict: high risk (50%) and moderate-high risk (50%) because the job insecurity and lack of performance expectations.
Fig. 3 also shows that positive dimensions were mainly associated with autonomy sense, showing a high (25%) and moderately high (30%) risk value due to the perception of having no influence on the work process and degrees of freedom at work [43]. Other dimensions showed good assessment: development and meaning of job satisfaction: Low risk (40%) and no risk (50%); superior support: low (40%) and low moderate risk (50%); social relationship: low moderate risk (20%) and low risk (55%); leadership quality: low Moderate Risk (35%), low risk (30%); satisfaction: low
moderate risk (35%), low risk (40%); esteem: low moderate risk (35%), low risk (40%). All dimensions support the commitment to the workplace, collaboration and relationship with coworkers and superiors.
Results in Fig. 2b suggest a well-lead work climate dimensions before intervention and have the following perception levels depicted in Fig. 2b: collaboration (75%), communication (75%) and satisfaction (78%). However, working conditions related to physical factors reached moderate levels (63%).
3.2. The Wilcoxon signed-rank test
Wilcoxon signed rank is a nonparametric test used to study 15 paired of psychosocial hazard data with non-normal distribution on a single sample.
The analysis of data depicted in Table 2 considers the magnitude and sign of the observed differences. Quantitative (QnPD) and qualitative (QcPD) psychological demands, work sense and integration (Ws&I), future insecurity (Fins), and task and role conflict (T&Role) dimensions showed lower magnitudes (negative ranges). Meanwhile, positive differences were found in autonomy (Auto), superior support (SupS), social support (SocS), quality of leadership (Lship), satisfaction (Sfac) and esteem (Stm).
Table 2 Wilcoxon test-perception of psychosocial risk and Hedge’s g statistic: pre and post virtual group intervention.
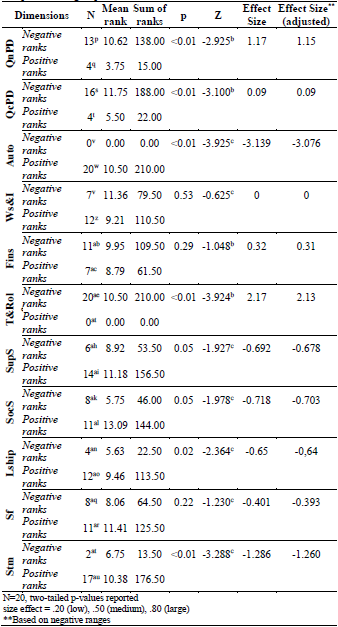
Source: the authors
Significant differences can be found in the quantitative psychological demands: Mdn=3,000; Range=3,3 (before) and Mdn=2,251; Range=2,0 (after) with Z= -2,925; p= < .01, also in qualitative demands: Mdn=3,125; Range=3,3 (before) and Mdn=2,25; Range=2,4 (after) Z= -3,100; p=< .01, and autonomy, showing no similarities in the statistic: Mdn=2.375; Range=3.0 (before) and Mdn=4.5; Range=1.8 (after), Z= - 3.925; p=< .01.
Work sense and integration (Ws&I), Future Insecurity (Fins) and satisfaction (Sfac) dimensions are not quite significant at the 5% level. Other dimensions were also affected after the intervention like task and role conflict (Z= -3,924; p< .01), quality of leadership (Z= -2,364; p< 0.02), and esteem (Z= -3,288; p<. 01).
Results of three work climate dimensions were statistically significant: collaboration (Z= -2,520; p=< .01), communication (Z= -2,184; p= 0.03), satisfaction (Z= -2,057; p= 0.04), and the workplace conditions dimension remained constant.
3.3. The Hedge’s g statistic
The Hedge’s g statistic determined how much one group differs from another. Values >.80 indicated a ’large’ effect size: quantitative psychological demands (QnPD), g: 1.17; autonomy (Auto), g: -3.139; task and role conflict (T&Role), g: 2.17; esteem (Stm), g: -3.288. Values >.50 that indicated a ’medium’ effect size: superior support (SupS), g: -0.692; social support (SocS), g: -0.717; and quality of leadership (Lship), g: -0.65. Effect sizes were slightly larger than they should if no intervention wouldn’t take place, suggesting that FB virtual group results were statistically significant.
4. Spearman’s rank correlation
The strength of the association between paired variables measured for the same individuals is necessary to identify dimensions affecting psychosocial hazard perception.
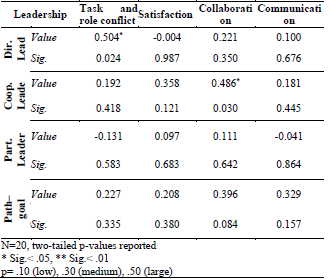
Two dimensions of psychosocial risk have a significant relationship with two leadership styles. In Table 3, correlations range from .486 to .504 (p <.05). Directive leadership has a positive relationship with task-role conflict (to major directive leadership self-perception, nurses know what’s expected from them within the group and have a sense of mission).
Table 3 Spearman Test: Leadership Styles & correlated dimensions post FB virtual group intervention
Source: the authors
Main correlated dimension in Table 3 adjusted well results showed by Contreras et al. [44]. Collaboration and communication became a priority to attend for most superiors with transformational behavior due to the influence on psychosocial risks, and the quality of the nurse’s performance.
Table 4 revealed a lack of work activities information or getting contradictory instructions from your superiors during postpandemic period had less impact while collaborative individual behaviors being adopted after the intervention as depicted in Table 3.
5. Discussion
The Wilcoxon comparison test showed that the indicators of qualitative and quantitative psychological demands im- proved, reducing the indicators of psychosocial risk. The participation of workers has generated a greater relationship between colleagues, better communication and therefore, less psychological burden.
The influence of two leadership styles slightly reducing psychosocial risk took a behavioral approach to superior transactional leadership providing no less than satisfactory short-term results, while transformational leadership can generate long-term effort, creativity, and productivity in followers. [41]
Results in Table 3 showed positive but non-significant correlation between the leadership style and the task-role conflict leaded by the perception of the demand task category and the knowledge about what is expected of you at work, according to Table 4. This addressed individual (relationship focused) and organizational (task focused) levels following the Path-goal theory [12].
Table 4 Spearman Test: Leadership Styles & correlated Psychosocial Risks specific items - post FB virtual group intervention
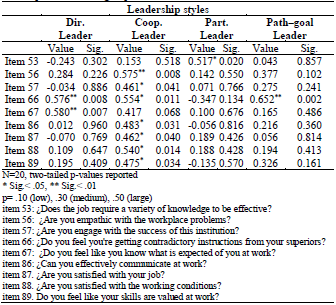
Source: the authors
The increased perception that nurses can make their own informed decisions and the positive outcome for all involved within the healthcare institution (questions 56 and 57), positively moderates relationship between collaborative leadership, sense and integration and communication, ranged from .461 to .575 (p <.05). The synergistic intervention promoted the sense that effective implementation of practices and processes achieve outcomes that are greater than the sum of individual efforts.
Psychosocial risks and work climate expressed a positive interest for cooperative leadership. Three categories ’empathy with the workplace problems’, ’engagement with the success of this institution’ and ’effectiveness of communication at work’ specifically enhance sense of commitment and interpersonal interactions with co-workers. Despite E-leadership less influential in virtual teams. However, there is evidence that virtual team leaders can engage in behaviors that are interpreted by team members as relationship-focused [42]. This encloses most part of what a relationship-focused leadership promote, inspiring a sense of collective purpose to reach the final goal, and highlight reflexivity as a critical information-processing to facilitate performance [38].
6. Conclusions
The purpose of this study was to determine if any significant relationships among psychosocial risk factors, perceived work climate and perception of leadership styles was possible to improve the well-being, by using a virtual team model based on participatory leadership. Surveys were conducted with 20 nurses of a Basic Hospital in a rural area of Ecuador. 15 women (75%) and 5 men (25%), performing mixed activities. They were aged 25 to 34 years old (60%), 35 to 44 years old (20%), less than 25 years old (15%) and more than 54 years old (5%).
Previous study showed that social relations, autonomy, and psychological demands are prominent dimensions leading psychosocial risk. The leadership style of the nursing professional is defined by the ability to care about other people need (cooperative) and the wiliness to participate in decision-making for a better workplace (participative).
The Hedge’s g statistic approach within the Wilcoxon signed-rank test were applied to accomplish the hypotheses, supported by a Spearman’s Rank correlation analysis. Concluding remarks about this study implies the strong relationship that psychosocial hazard has with leadership styles mediated by the perception of the work environment. In particular, the cooperative leadership is empowered even slightly more than participative style after the FB virtual group implementation.
Variants of leadership style were present in the initial state: cooperative leadership (83%), directive leadership (83%), participative leadership (79%), collaborative leader- ship (72%). Functional Team leadership Theory required gathered participants to meeting team needs, tasks distribution and further instructions to enhance team effectiveness, while relationship-focused leadership facilitated interaction among team members within a virtual group strategy. After the intervention a positive participatory (83%) and collaborative (81%) performance was accomplished. Directive leadership (70%) decreased after the intervention, while achievement-oriented leadership remained low (68%). First, they perceive themselves as collaborative and directive leaders and later their self-perception changed to a more convenient participative and cooperative behavior in agreement with previous studies.
There are significant differences in the dimensions of psychosocial risks after the application of a virtual short-run group model in nurses, following the definition of Social Cognitive Theory and the Reflexivity Theory explaining leadership based on work team perceptions.
The mechanism of rewards empowered by a transactional leadership behavior in superiors, leaded to a participative attitude in nurses to enhance healthcare quality in a workplace where their skills are valued. New insights in transactional-transformational leadership models for middle managers could be a matter of interest within strategies to reduce psychosocial hazards.
A sample size that is small reduces the power of the study and increases the margin of error. Future work should include a wide health workers community to complement the findings.

