










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista Colombiana de Psiquiatría
versão impressa ISSN 0034-7450
rev.colomb.psiquiatr. v.39 n.1 Bogotá jan./mar. 2010
Validity and Reliability of the Abbreviated Barratt Impulsiveness Scale in Spanish (BIS-15S)*
Validez y confiabilidad de la versión abreviada de la escala de impulsividad de barratt (BIS-15S)
Luis Orozco-Cabal1 Maritza Rodriguez2 David V. Herin3 Juanita Gempeler4 Miguel Uribe5
1 Physician. PhD in Neuroscience. General Psychiatry Resident, Departamento de Psiquiatría y Salud Mental, Facultad de Medicina, Pontificia Universidad Javeriana, Bogota, Colombia. Former Chair Neuroscience Department, Facultad de Medicina, Universidad de Los Andes, Bogota, Colombia.
2 Psychiatrist and Clinical Epidemiologist, Programa Equilibrio, Bogota, Colombia. Professor, Departamento de Psiquiatría y Salud Mental, Facultad de Medicina, Pontificia Universidad Javeriana, Bogota, Colombia.
3 PhD Neuroscience. Assistant professor, Department of Psychiatry, University of Minnesota, Twin Cities, Minneapolis, USA.
4 Psychologist. CBT Diploma, Programa Equilibrio, Bogota, Colombia.
5 Psychiatrist. Liaison Psychiatrist, Psychoanalyst. Professor, Departamento de Psiquiatría y Salud Mental, Facultad de Medicina, Pontificia Universidad Javeriana, Bogotá, Colombia.
Correspondencia: Luis Orozco-Cabal Departamento de Psiquiatría y Salud Mental Facultad de Medicina. Pontificia Universidad Javeriana Carrera 7 No. 40-62. Bogotá, Colombia l.orozco@javeriana.edu.co
Recibido para evaluación: 2 de diciembre del 2009 Aceptado para publicación: 2 de marzo del 2010
Abstract
Objective: This study determined the validity and reliability of a new, abbreviated version of the Spanish Barratt Impulsiveness Scale (BIS-15S) in Colombian subjects. Method: The BIS-15S was tested in non-clinical (n=283) and clinical (n=164) native Spanish-speakers. Intrascale reliability was calculated using Cronbach's a, and test-retest reliability was measured with Pearson correlations. Psychometric properties were determined using standard statistics. A factor analysis was performed to determine BIS-15S factor structure. Results: 447 subjects participated in the study. Clinical subjects were older and more educated compared to non-clinical subjects. Impulsivity scores were normally distributed in each group. BIS-15S total, motor, non-planning and attention scores were significantly lower in non-clinical vs. clinical subjects. Subjects with substance-related disorders had the highest BIS-15S total scores, followed by subjects with bipolar disorders and bulimia nervosa/binge eating. Internal consistency was 0.793 and test-retest reliability was 0.80. Factor analysis confirmed a three-factor structure (attention, motor, nonplanning) accounting for 47.87% of the total variance in BIS-15S total scores. Conclusions: The BIS-15S is a valid and reliable self-report measure of impulsivity in this po pulation. Further research is needed to determine additional components of impulsivity not investigated by this measure.
Key words: Personality assessment, validation studies, Colombia.
Resumen
Objetivo: Determinar la validez y confiabilidad de una nueva versión abreviada de la Escala de Impulsividad de Barratt (BIS-15S) en la población colombiana. Método: El BIS- 15S fue aplicado a sujetos hispanoparlantes no clínicos (n=283) y clínicos (n=164). Sus propiedades psicométricas se establecieron con pruebas estadísticas estandarizadas y sus factores principales se analizaron para determinar la estructura de los factores del instrumento. Resultados: 447 sujetos participaron en el estudio. Los sujetos clínicos fueron mayores y más educados que los sujetos no clínicos. Los puntajes estuvieron distribuidos normalmente en las dos poblaciones. Los puntajes total, motor, de no planeación y atención del BIS-15S fueron significativamente menores en sujetos no clínicos, comparados con sujetos clínicos. Los puntajes de los sujetos con abuso/dependencia a drogas fueron los más altos, seguidos de aquellos de sujetos con trastornos bipolares y bulimia nerviosa/trastorno por atracones. La consistencia interna del BIS-15S fue 0,793; su confiabilidad prueba-reprueba, 0,80. El análisis de factores confirmó tres factores principales (motor, no planeación y atención) responsables de 47,87% de la varianza del puntaje total del BIS-15S. Conclusiones: El BIS-15S es una medida válida y confiable del rasgo impulsividad en la población colombiana. Son necesarios estudios adicionales para establecer otras dimensiones del rasgo no medidas por el instrumento.
Palabras clave: Determinación de la personalidad, estudios de validación, Colombia.
Introduction
Impulsivity is a multidimensional personality trait related to the control of emotions and behavior (1). Numerous studies suggest that high levels of impulsivity are associated with deficits in regulating behavioral and physiological responses associated with reward, behavioral inhibition, and decisionmaking processes (2). Accordingly, impulse control disorders, such as violent outbursts, substance- related problems, accidental and self-inflicted injuries, are prevalent in impulsive subjects and significantly impact society (3). Similarly, impulsivity has been implicated in numerous psychiatric disorders including cluster B personality disorders (e.g. borderline and antisocial personality disorders), substance abuse, bipolar disorders, attention deficit hyperactivity disorder, eating disorders (i.e. bulimia nervosa and binge eating disorder) and suicide (2). More specifically, high levels of impulsivity seem to increase subject's vulnerability to develop these disorders, or if already symptomatic, high impulsivity decreases zreatment-adherence, predates or coexists with symptomatic exacerbations, and increases the likelihood of complications or co-morbid conditions (2,3). Thus, an assessment of impulsivity levels should be incorporated to the clinical evaluation of individuals with these conditions.
The Barratt Impulsiveness Scale (11th version, BIS-11) is one of the most commonly used self- report measures of impulsivity; its psychometric properties have been determined in both clinical and non-clinical subjects (4,5). During the past decade, multiple translations of the BIS-11 have been published (6-11), and neuroimaging studies indicate that BIS-11 scores correlate to prefrontal integrity and function, as well as central serotoninergic function.This instrument comprises 30 items that assess three independent sub-dimensions of impulsivity: (a) the ability to focus and be vigilant (attention); (b) living for the moment (non-planning); (c) acting without thinking (motor). Collectively, the three sub-dimensions represent a total impulsivity score (5).
Recently, Oquendo et al. (6) adapted the BIS-11 to Spanish using a sample of 29 dominant Spanish- speaking psychiatric outpatients from the Caribbean. Their analyses showed adequate linguistic, conceptual, and scale equivalence between the English and Spanish version of the BIS-11. More recently, Spinella (13) reported normative and demographic influence on BIS-11 scores in a large community sample (n=700) in the US. The results of this study are in agreement with previous studies in restricted populations: the factor analyses confirmed a three-factor structure for the personality construct impulsivity; the reliability of the instrument was high (Cronbach's a=0.81). Importantly, the five items with the highest loading on the factor analysis for each sub-dimension were extracted to conform a shorter (15 items) version of the BIS-11. The short form (BIS-15) correlated well with the original instrument (r=0.94, p<0.01) and retained a three-factor structure. Also, factor analysis demonstrated that items 14 and 30 of the original instrument had to be included in the motor, and planning, groups, respectively, to improve the characteristics of the instrument.
Unfortunately, the psychometric properties of the Spanish adaptation of the BIS-11 have not been determined in South American populations, thus limiting its application in clinical practice. In order to mend this shortfall and based on the f ndings of Spinella (13) and Oquendo et al. (6), we have constructed an abbreviated version of the BIS-15 in Spanish (BIS-15S) and determined its validity and reliability in non-clinical and clinical samples of Colombian male and female subjects. The results of this study are critical to improve the assessment of impulsivity in Spanish- speaking communities.Methods
BIS-15S
The BIS-15S (Table 1) consists of 15 items (BIS11 items No. 15, 18, 2, 12, 21, 11, 30, 8, 1, 10, 29, 9, 7, 19, 16) extracted from the Spanish adaptation of the BIS-11 by Oquendo et al. (6). These15 items were selected
Pretesting BIS-15S
Initially, a preliminary version of the BIS-15S was administered to 30 subjects who were randomly selected from a sample of 800 undergraduate students at Los Andes University (Bogota, Colombia). Subjects were instructed to answer the instrument and indicate any items that were formulated ambiguously or difficult to understand. All data was collected and analyzed by a research assistant external to the study. Based on these results of this preliminary assessment, the investigators refined the instrument to improveits comprehension and application procedure. None of the items were modified in the instrument, however it was necessary to emphasize the time frame of the items: "Esta es una prueba para medir algunas de las formas en que usted actua o piensa en distintas situaciones a lo largo de su vida".
Validity and Reliability Assessment of the BIS-15S
Following preliminary assessment and refinement of the BIS-15S, validity and reliability of the instrument were determined.
SUBJECTS
Male and female participants in this subsequent study included non-clinical and clinical subjects. The non-clinical sample group was comprised of 283 undergraduate and graduate students attending Los Andes University (Bogota, Colombia) that were selected according to a randomized sampling method. Non-clinical subjects were included if the were ages 18 through 65 and Spanish literate. However, they were excluded if the reported a history of moderate to severe head trauma or epilepsy. The clinical sample group was comprised of 164 psychiatric outpatients attending Equilibrio Program and Clinica La Inmaculada outpatient psychiatry clinics in Bogota (Colombia) between June 2007 and July 2009. Clinical subjects were selected by convenient sampling. Clinical subjects were included if they were ages 18 through 65, were Spanish literate, and were currently receiving medical treatment for major depression, dysthimia, any bipolar disorder, anxiety disorders, substance abuse or dependence, eating disorders or impulse control disorders according to DSM-IV criteria. Clinical subjects were excluded if they hada history of moderate to severe head trauma, mental retardation, epilepsy, psychotic disorders or were in a dissociative state during testing.
The sample size was determined using data (means, SD) from previous BIS-11 normatization studies in clinical and non-clinical populations andBIS-15S pre-test results (5,9,14). In addition, sample size recommendations for principal component analysis were followed (15,16); a significance level of 0.05 and power of 80% were used.
TESTING AND DATA COLLECTION
The study purpose and procedures were presented in written format and explained verbally to all interested subjects. Prior to participation, all subjects gave informed consent on forms approved by the Research and Ethics Committee at all participating institutions in compliance with resolution No. 8430/1993 of the Ministerio de Salud de Colombia regarding research with human subjects. Once enrolled in the study, each participant received a numeric identification code. Subsequently, demographic information was collected with standardized forms and the BIS-15S was administered to all participants. Research assistants external to the study verified subjects' responses and calculated BIS-15S scores.
STATISTICAL ANALYSES
Descriptive statistics for demographic variables and BIS-15S scores (total and sub-dimension scores) were calculated for non- clinical subjects. Extremes values in this sample group were identified and excluded from final analyses. Kolmorogov-Smirnov tests were employed to confirm normal distribution. Linear regression analyses were performed to identify possible associations between selected demographic variables (sex, age and education) and BIS-15S scores. Intra-scale reliability (Cronbach's a) and test-retest reliability were also calculated. For test-retest reliability, 20 participants were randomly selected to re-take the BIS-15S two weeks after the first evaluation. Pearson correlations were used as a measure of test-retest reliability since two evaluators were responsible for data collection (17).
Concurrent validity for the BIS-15S was determined against clinical criterion, as there is no "gold standard" to assess the personality trait impulsivity. For the clinical sample, experienced psychiatrists made diagnoses with the Structured Clinical Interview for DSM-IV (SCID) (18). Stratified data analyses were performed according to primary diagnostic categories including: anorexia nervosa (AN), bulimia nervosa and binge eating disorders (BUL), anxiety disorders (ANX), bipolar disorders (BD), and substance-related disorders (SRD). Descriptive statistics were used to calculate demographic variables and BIS-15S scores in the total clinical sample group and each diagnostic category. Kolmorogov-Smirnov tests were employed to conf rm normal distribution. Linear regression analyses were conducted to identify possible associations between selected demographic variables (sex, age and education) and BIS-15S scores. Student t-tests and non-parametric tests were employed to test for significant differences among genders and in demographic variables between clinical and non-clinical sample groups, respectively. ANOVAS and post hoc tests were performed to test for significant differences for all BIS-15S scores (total and subdimensions scores) among clinical and non-clinical sample groups. BIS-15S total scores were subject to factor analysis by principal components using an orthogonal (Vari- max) rotation to confirm the factor structure of the instrument (7,10). Statistical analyses were performed using SAS® (Version 9) and SPSS® (Version 14.5).
Results
Subjects
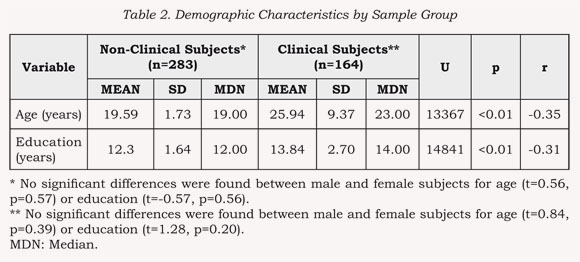
447 subjects participated in the study (non-clinical sample group n=283, clinical sample group n=164). Demographic characteristics for each sample group are indicated in Table 2. Kolmogorov- Smirnov tests indicated that age and education values were not normally distributed within non- clinical [Age: D(283)=0.199, p<0.01; Education: D(164)=0.186, p<0.01] and clinical [Age: D(283)=0.257, p<0.01; Education: D(164)=0.117, p<0.01] sample groups. Generally, clinical subjects were older and more educated compared to non- clinical subjects.
These findings were expected as subjects drawn from students attending colleges or universities tend to be younger and exhibit less variability across demographic characteristics compared to community samples. Also, clinical subjects included in our study were expected to show a greater, but restricted, variability across demographic characteristics compared to non-clinical subjects, as these mental diseases typically affect young adults (2). In fact, 78.66% of our clinical sample group is composed by subjects 32 years of age or younger.
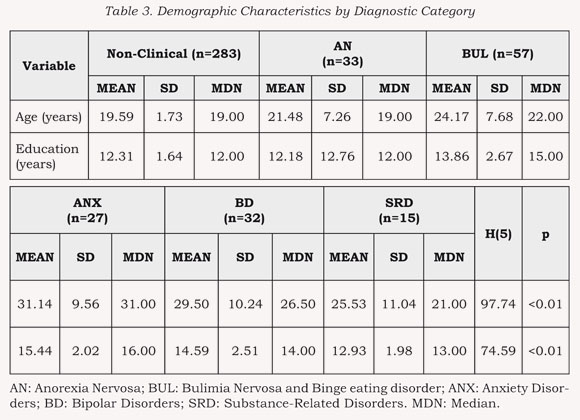
Of the clinical group, age and education were compared across each diagnostic category (See Table 3). Post hoc tests with Bonferroni correction (Significance p<0.003) revealed that subjects in the BUL (p<0.001), ANX (p<0.001) and BD (p<0.001) groups were older and more educated than non-clinical subjects. No significant differences were found between the latter group and subjects in AN and SRD groups. Similarly, subjects in the ANX (p<0.001) and BD (p<0.001) groups were older than subjects in AN and BUL groups, but only more educated than AN (p<0.001). Finally, subjects in the SRD (p<0.001) group were significantly more educated compared to subjects
BIS-15S Scores
NON-CLINICAL SUBJECTS
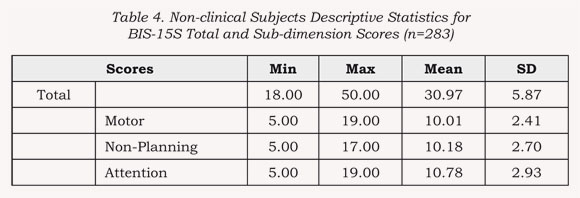
Descriptive statistics for BIS- 15S total and sub-dimension scores are indicated in Table 4. A one- sample olmogorov-Smirnov test indicated that BIS-15S total scores were normally distributed (Z=1.31, p=0.06, two-tailed). Linear regression analysis indicated that age, sex and educationdid not predict BIS- 15S total scores (F(3,282)=0.427, p=0.73).CLINICAL SUBJECTS
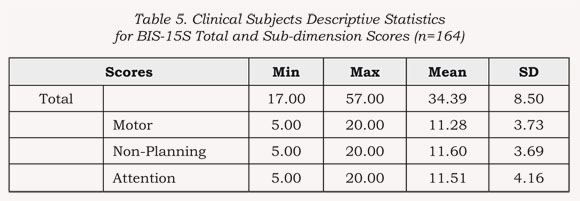
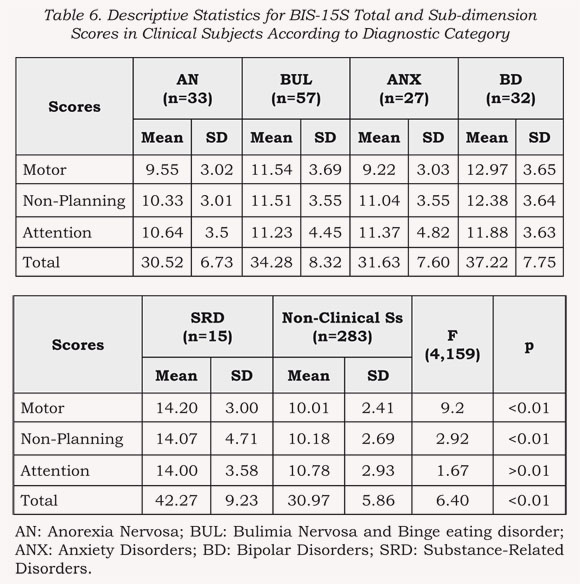
Descriptive statistics for BIS- 15S total and sub-dimension scores for all the clinical sample and according to diagnostic categories are indicated in Tables 5 and 6. A one-sample Kolmogorov-Smirnov test demonstrated that total scores from clinical subjects were normally distributed (Z=0.85, p=0.45, two tails). Linear regression analyses indicated that age, sex and education did not predict BIS-15S total scores was (F(2,161)=0.533, p=0.58).
Descriptive statistics for BIS- 15S total and sub-dimension scores according to diagnostic categories in the clinical sample are indicated in Table 6. One-way ANOVAS demonstrated signif cant differences for BIS-15S total, motor and nonplanning impulsivity scores among diagnostic categories (see Table 6). Subjects in the SRD group had the highest BIS-15S total scores, followed by BD and BUL groups. Specifically, post hoc tests demonstrated that the SRD group had the highest BIS-15S total scores compared to all other groups (p<0.01 for all comparisons); BD group total scores were only significantly higher than those in the AN group (p<0.01); BUL scores were significantly smaller that SRD group scores (p<0.01), but not significantly different from BD (p>0.01), ANX (p>0.01) or AN (p>0.01) scores. Total impulsivity scores for subjects with AN and ANX were very similar (p>0.01). This is in agreement with the observation that lower impulsivity levels and increased risk-aversion usually characterize subjects with these disorders (14). Similar tendencies were found for BIS-15S motor and non-planning sub-dimensions. SDR and BD groups motor impulsivity scores were significantly higher compared to ANX and AN group scores (p<0.01 for all comparisons), while BUL scores were only significantly higher than ANX group score (p<0.01). Non-planning scores for the SRD group were signif cantly higher compared to AN (p<0.01) group scores only. No significant differences were found among groups for attention impulsivity scores. These data support a significant role for impulsivity in substance-related disorders.
One way ANOVAS also demonstrated significant differences for BIS-15S total, motor impulsivity, non-planning and attention impulsi- vity scores between clinical and non- clinical subjects (BIS-15S TOTAL: F(1,445)=25.16 p<0.01; BIS-15S Motor: F(1,445)=19.05 p<0.01; BIS- 15S Non-Planning: F(1,445)=21.71 p<0.01; Attention F(1,445)=4.75 p<0.05). Overall, non-clinical subjects exhibited lower BIS-15S total, motor, non-planning and attention impulsivity scores compared to clinical subjects.
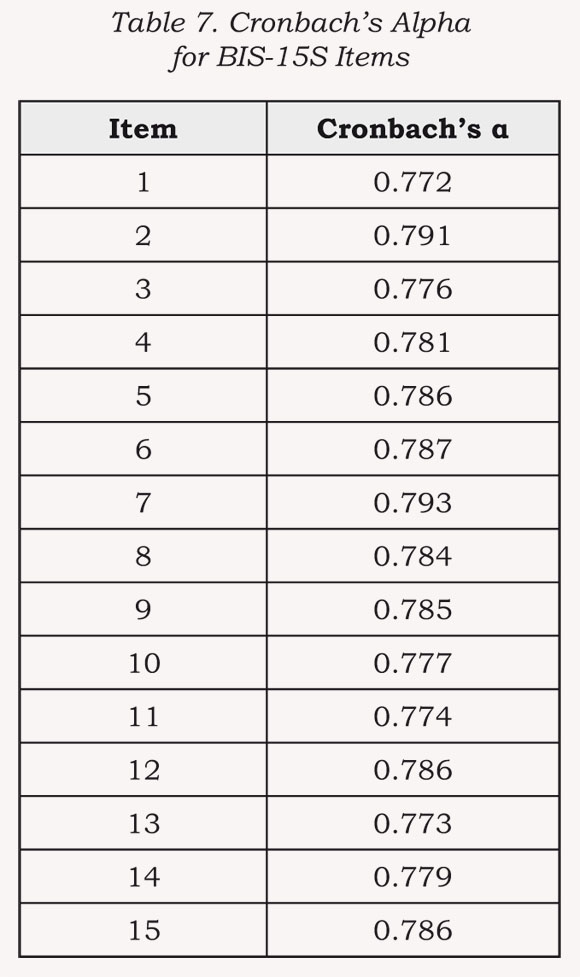
Internal consistency as measured by Cronbach's a was 0.793 overall. Cronbach's a values for each item are shown in Table 7. Test-retest reliability as measured by Pearson correlation coefficient was 0.80, p<0.01.
Factor Analysis
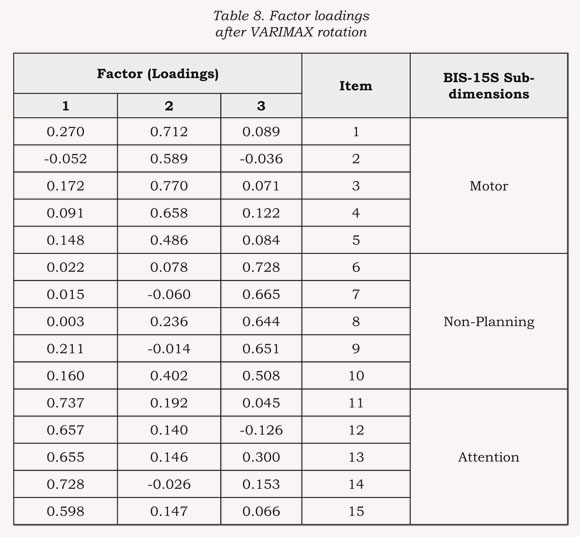
All items on the BIS-15S were subject to factor analysis (see Table 8). A three-factor structure was defined a priori based on reported solutions (4,5). The Kaiser-Meyer-Olkin measure of sampling adequacy and Bartlett's Test were adequate (0.801 and 0.000, respectively). All items had sampling sufficiency values greater than 0.70 (16).
Factor analysis confirmed a three-factor structure for the BIS- 15S. The first factor (attention) accounted for 25.54% of the total variance. A second factor named "motor" accounted for 11.79% of the total variance. A third factor, named "non-planning" accounted for 10.54% of the total variance. Collectively these three factors accounted for 47.87% of the total variance in BIS-15S total scores. Factor loadings after VARIMAX rotation are given in Table 8.
Discussion
This study describes an abbreviated form of BIS-15S. We report normative data obtained from Colombian subjects, with the instrument's properties tested in non-clinical and clinical subjects. Compared to non-clinical subjects, clinical subjects were older, more educated and more widely distributed across age ranges. Linear regression failed to show significant associations between demographic characteristics and impulsivity scores. Impulsivity scores were normally distributed in each sample group. BIS-15S total, motor, nonplanning and attention impulsivity scores were signif cantly lower in non-clinical subjects compared to clinical subjects. Similarly, BIS- 15S total, motor and non-planning impulsivity scores were significantly different among
Specifically, subjects in the SRD group exhibited greater BIS-15S total scores compared to all other groups, followed by subjects in the BD and BUL groups. Motor impulsivity scores were significantly greater for the SDR and BD groups compared to ANX and AN groups. Motor impulsivity scores in the BUL group were greater compared to those from the AN group. Non-planning impulsivity scores were also greater for the SDR group compared to AN. No additional differences were demonstrated among diagnostic groups. The internal consistency, as measured by Cronbach's a, was 0.776 and test-retest reliability, as measured by Pearson correlation coeffi cient, was 0.80, p<0.01. The factor analysis confirmed a three-factor structure (attention, motor, non-planning) accounting for 47.87% of the total variance in BIS-15S total scores.
Our study significantly contributes to the assessment of impul- sivity by clinicians in this country. The BIS-15S is a novel and short, easy to use, self-report measure of the trait impulsivity. The items included in the instrument are easy to understand by native Spanish- speaking Colombians and can be answered in less than 10 minutes. These characteristics are important because language variations among Spanish-speaking communities can modify item comprehension; consultation times have been restricted to 20 minutes or less in most health services in this country; and, subjects with high levels of impulsivity exhibit deficits in sustaining attention on continuous tasks (1). Thus, shorter instruments are more likely to be thoroughly and accurately completed by impulsive subjects.
Significant differences in demographic variables among non- clinical and clinical subjects were anticipated in this study. First, clinical subjects were included in the study to test the concurrent validity of the instrument against clinical criteria. Thus, it was essential to assure heterogeneity within clinical subjects and between clinical and non-clinical subjects to correctly assess the behavior of the BIS-15S across subjects with various types of impulsivity-related psychiatric conditions. Second, it is expected that samples drawn from students attending colleges or universities exhibit less variability across demographic variables compared to community samples as they have already been preselected from the general population according to institutional enrollment policies. Finally, sample size differences among groups may also account for the observed results as sample size significantly affects variability distribution within sample groups (19).
Spinella (13) has previously shown that BIS-15 score decrease with age and education, although the model in his study only accounted for 10.7% of the variance. Conversely, in our study linear regression analyses for demographic variables as predictors of BIS-15S total scores were not significant. Sample size differences between studies and variability restrictions imposed by the type of subjects participating in our study may account for the observed findings (17). Thus, based on our data we cannot exclude a significant association between age and education and BIS-15S scores.
Consistent with Patton et al. (5) and Stanford (4) our analyses failed to show significant gender differences for either the BIS-15S total or sub-dimension scores. However, Stanford (4) did f nd a signif cant gender difference for the firstorder subscale perseverance, being lower in women compared to men. However, firs-order factors were not determined in this study as BIS- 15 (13) has only three first-order factors. Thus, we cannot exclude a gender difference in these factors if present in the BIS-15S.
Non-clinical subjects exhibited BIS-15S total, motor, non-planning and attention impulsivity scores significantly lower than clinical subjects. These findings are in agreement with previous reports of overall low impulsiveness in non- clinical subjects vs. subgroups of subjects diagnosed with antisocial personality disorder (20), borderline personality disorder (21-23), substance abuse/dependence (24), bipolar disorders (25,26), attention deficit/hyperactivity disorder and conduct disorders (2, 27,28), eating disorders (14), suicide (29) and impulse control disorders (30).
In general, our findings indicate that subjects with SRD, BD and BUL compared to subject with AN or ANX have elevated total impulsivity scores as measured by the BIS-15S. More specifically high impulsivity appears to be mediated by motor and non-planning components in SRD and BD groups, but only by motor components in the BUL group. This finding is in agreement with previous studies demonstrating that impulsivity is an important component in bipolar disorders (3133), substance abuse/dependence and eating disorders (14). In fact, high levels of impulsivity are associated with an increased vulnerability to suffer from these disorders, significantly modify their clinical presentation and worsen clinical outcomes (2). Specifically, elevated BIS-11 scores are associated with early onset, more frequent episodes of illness, and a history of suicide attempts in bipolar subjects. Preclinical and clinical studies have demonstrated that impulsivity is a significant vulnerability factor for substance abuse/dependence. Importantly, BIS-11 scores have shown to be exquisitely sensitive to distinction within substance abuse disorders (4). For example, BIS-11 score are predictive of the level of an individual's cocaine use (36). Finally, impulse control disorders frequently coexist in patients with bipolar disorders and patients with substance abuse, indicating a common substrate in theses subjects that may be related to affective instability, automaticity, response inhibition, and decision making deficits (33,37). Thus, it is desirable that impulsivity may be correctly assessed in these individuals using similar this or similar self-report instruments and behavioral measures of impulsivity as suggested by Barratt et al. (1, 38).
The factor analysis confirmed a three-factor structure (attention, motor, non-planning). This factor structure only accounted for 47.87% of the total variance in BIS-15S total scores. Although a three subscale substructure for the BIS-11 has been consistently demonstrated in the literature, the amount of variability explained by the solution is below 50%. The latter suggests that there might be other dimensions relevant to impulsivity, which have not been included in the BIS or characterized to date. Nonetheless, BIS has become one of the most widely used self-report measures of impulsivity in the world and reflects our current understanding about this phenomenon.
The internal consistency and test-retest reliability measures of the instrument are above acceptable levels (15), which suggests that the items included in the BIS-15S consistently measure the construct impulsivity and are highly reliable.
One particular strength of our study is the sample used. Participants include non-clinical and clinical subjects in sufficient number to detect significant differences among groups. In addition, including a clinically diverse or heterogeneous sample is necessary to determine the concurrent validity of the instrument as there is no "gold-standard" to measure impulsivity. The latter proves to be an important limitation of every study that examines the psychometric properties, validity and reliability of a novel self-report measure of impulsivity. Nonetheless, our study suggests that the BIS-15S can be applied to measure the trait impulsivity in non-clinical and clinical subjects in Colombia and perhaps, other Spanish speaking communities. The ease of its application and scoring procedures, plus the fact that the instrument can be applied by any physician at any primary care facility without using most of the 15 to 20 minute consultation time imposed by most health services in this country, are important characteristics that increase the attractiveness of the instrument. However, caution should be advised in the interpretation of the results as our data suggest that other subdimensions of impulsivity or factors related to its expression might not be accounted for in our current understanding of the construct impulsivity.
Although the BIS effectively measures the trait of impulsivity, determination of self-report measures of state-like impulsivity are problematic. For example, some participating subjects f nd it diff - cult to differentiate BIS item scores across various portions of their lifetime. Additionally, the time course of co-occurring psychiatric illnesses may affect the impact of impulsivity on cognition and behavior, potentially biasing impulsivity scores. Given these concerns, development of state-like impulsivity measures will be important in the future.
* Supported by SEMILLA grant from Los Andes University (LO-C), U. S. National Institute on Drug Abuse DA023548 (DVH), and Program Equilibrio (MR and JG).
References
1. Barratt ES, Orozco-Cabal LF, Moeller FG. Impulsivity and sensation seeking: a historical perspective on current challenges. En: Stelmack R (Editor). On the psychobiology of personality: essays in honor of Marvin Zuckerman. Amsterdam: Elsevier Science; 2004. p. 3-17. [ Links ]
2. Moeller FG, Barratt ES, Dougherty DM, Schmitz JM, Swann AC. Psychiatric aspects of impulsivity. Am J Psychiatry. 2001;158(11):1783-93. [ Links ]
3. Hollander E, Evers M. New developments in impulsivity. Lancet. 2001;358(9286):949-50. [ Links ]
4. Stanford M, Mathias C, Dougherty D, Lake S, Anderson N, Patton J. Fifty years of the Barratt Impulsiveness Scale: An update and review. Pers Indiv Dif. 2009;47(5):385-95. [ Links ]
5. Patton JH, Stanford MS, Barratt ES. Factor structure of the Barratt impulsiveness scale. J Clin Psychol. 1995;51(6):768-74. [ Links ]
6. Oquendo MA, Baca-Garcia E, Graver R, Morales M, Montalvan V, Mann JJ. Spanish adaptation of the Barratt impulsiveness scale (BIS-11). EurPsy- chiatry. 2001;15(3):147-55. [ Links ]
7. Bayle FJ, Bourdel MC, Caci H, Gorwood P, Chignon JM, Ades J, et al. Structure factorielle de la traduction Francaise de l'echelle d'impulsivite de Barratt (BIS-10). Can J Psychiatry. 2000;45(2):156-66. [ Links ]
8. Preuss UW, Rujescu D, Giegling I, Koller G, Bottlender M, Engel RR, et al. Factor structure and validity of a German version of the Barratt impulsiveness scale. Fortschr Neurol Psychiatr. 2003; 71(10):527-34. [ Links ]
9. Fossati A, Di Ceglie A, Acquarini E, Barratt ES. Psychometric properties of an Italian version of the Barratt impulsiveness scale-11 (BIS-11) in nonclinical subjects. J Clin Psychol. 2001; 57(6):815-28. [ Links ]
10. Someya T, Sakado K, Seki T, Kojima M, Reist C, Tang SW, et al. The Japanese version of the Barratt Impulsiveness Scale, 11th version (BIS-11): its reliability and validity. Psychiatry Clin Neurosci. 2001;55(2):111-4. [ Links ]
11. Chung YO, Lee CW. A study of factor structures of the Barratt impulsiveness scale in Korean university students. Korean J Clin Psychol. 1997;16:117-29. [ Links ]
12. Baca-García E, Salgado BR, Segal HD, Lorenzo CV, Acosta MN, Romero MA, et al. A pilot generic study of the continuum between compulsivity and impulsivity in females: the serotonin transporter promoter polymorphism. Prog Neuropsychopharmacol Biol Psychiatry. 2005;29(5):713-7. [ Links ]
13. Spinella M. Normative data and a short form of the Barratt Impulsiveness Scale. Int J Neurosci. 2007;117(3):359-68. [ Links ]
14. Rosval L, Steiger H, Bruce K, Israël M, Richardson J, Aubut M. Impulsivity in women with eating disorders: problem of response inhibition, planning, or attention? Int J Eat Disord. 2006;39(7):590-3. [ Links ]
15. Nunnally J, Bernstein I. Psychometric theory. 3rd ed. New York: McGraw- Hill; 1994. [ Links ]
16. Pett MA, Lackey NR, Sullivan JJ. Making sense of factor analysis: the use of factor analysis for instrumental development in health care research. Thousand Oaks: Sage; 2003. [ Links ]
17. Miles J, Shelvin M. Applying regression and correlation: a guide for students and Researchers. London: Sage; 2001. [ Links ]
18. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders IV- Text Revised. Washington: American Psychiatric Association; 2000. [ Links ]
19. Field A. Discovering statistics using SPSS. London: Sage; 2005. [ Links ]
20. Barratt ES, Stanford MS, Kent TA, Felthous A. Neuropsychological and cognitive psychophysiological substrates of impulsive agression. Biol Psychiatry. 1997;41(10):1045-61. [ Links ]
21. Dougherty DM, Bjork JM, Huckabee HC, Moeller FG, Swann AC. Laboratory measures of agression and impulsivity in women with borderline personality disorder. Psychiatry Res. 1999;85(3):315-26. [ Links ]
22. Koenisberg HW, Harvey PD, Mitro- poulou V, New AS, Goodman M, Sil- verman J, et al. Are interpersonal and identity disturbances in borderline personality disorder criteria linked to traits of affective instability and impulsivity? J Pers Disord. 2001;15(4):358-70. [ Links ]
23. Links PS, Heslegrave R, van Reekum R. Impulsivity: core aspect of borderline personality disorder. J Pers Disord. 1999;13(1):1-9. [ Links ]
24. De Wit H. Impulsivity as a determinant and consequence of drug use: a review of the underlying process. Addict Biol. 2009;14(1):22-31. [ Links ]
25. Swann AC, Anderson JC, Dougherty DM, Moeller FG. Measurement of interepisode impulsivity in bipolar disorder. Psychiatry Res. 2001;101(2):195-7. [ Links ]
26. Swann AC. Impulsivity in mania. Curr Psychiatry Rep. 2009;11(6):481-7. [ Links ]
27. Willcutt EG, Pennington BF, Chhabildas NA, Friedman MC, Alexander J. Psychiatric comorbidity associated with DSM-IV ADHD in nonreferred sample twin. J Am Acad Adoslec Psychiatry. 1999;38(11):1355-62. [ Links ]
28. Malloy-Diniz L, Fuentes D, Leite WB, Correa H, Bechara A. Impulsive behavior in adults with attention deficit/ hyperactivity disorder: characterization of attention, motor and cognitive impulsiveness. J Int Neuropsychol Soc. 2007;13(4):693-8. [ Links ]
29. Dougherty DM, Mathias CW, Marsh DM, Papageorgiou TD, Swann AC, Moeller FG. Laboratory measured behavioral impulsivity relates to suicide attempt history. Suicide Life Threat Behav. 2004;34(4):374-85. [ Links ]
30. Lojoyeaux M, Arbaretaz M, McLoughlin M, Ades J. Impulse control disoders and depression. J Nerv Ment Dis. 2002;190(5):310-4. [ Links ]
31. Henry C, Mitropoulou V, New AS, Koenigsberg HW, Silverman J, Siever LJ. Affective instability and impulsivity in borderline personality and bipolar II disorders: similarities and differences. J Psychiatr Res. 2001;35(6):307-12. [ Links ]
32. McElroy SL, Pope HG Jr, Keck PE Jr, Hudson JI, Phillips KA, Strakowski SM. Are impulse-control disorders related to bipolar disorder? Compr Psychiatry. 1996;37(4):229-40. [ Links ]
33. Najt P, Pérez J, Sanches M, Peluso MA, Glahn D, Soares JC. Impulsivity and bipolar disorder. Eur Neuropsy- chopharmacol. 2007;17(5):313-20. [ Links ]
34. Verdejo-García A, Lawrence AJ, Clark L. Impulsivity as a vulnerability marker for substance-use disorders: Review of findings from high-risk research, problem gamblers and genetic association studies. Neuroscience and Biobehav Rev. 2008;32(4):777-810. [ Links ]
35. Swann AC, Lijffijt M, Lane SD, Steinberg JL, Moeller FG. Increased traitlike impulsivity and course of illness in bipolar disorder. Bipolar Disord. 2009;11(3):280-8. [ Links ]
36. Lejuez CW, Bornovalova MA, Reynolds EK, Daughters SB, Curtin JJ. Risk factors in the relationship between gender and crack/cocaine. Exp Clin Psychopharmacol. 2007;15(2):165-75. [ Links ]
37. Adinoff B, Rilling LM, Williams MJ, Schreffler E, Schepis TS, Rosvall T, et al. Impulsivity, neural deficits, and the addictions: the "oops" factor in relapse. J Addict Dis. 2007; 26 Suppl 1:25-39. [ Links ]
38. Barratt ES, Felthous AR. Impulsive versus premeditated aggression: implications for mens rea decisions. Behav Scis Law. 2003;21(5):619-30. [ Links ]
Conflicto de interés: los autores manifiestan que no tienen ningún conflicto de interés en este artículo.

