











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
People with muscle dysmorphia (MD), as a variant of body dysmorphic disorder, present distortion (based on their perception of being insufficiently muscular) and extreme body preoccupation, which results in clinically relevant discomfort.1 In addition, as a behavioural expression, the person adopts extreme behaviours for bodily change. Among the most characteristic are: weightlifting, drastic changes in diet and ergogenic substance use (ESU).2-4 Generically, the term ergogenic substances (ES) is applied to all products that improve a body's performance5 and are usually classified as: nutritional (such as proteins), pharmacological (such as amphetamines) or hormonal (such as anabolic androgenic steroids [AAS]). Meanwhile, the reasons for use can be classified as: psychophysiological, psychoemotional and social.6
In the literature on MD, ESU, and more specifically AAS use, are often referred to but are not considered relevant when diagnosing MD,1,7 with the functional relationship between the same also remaining unclear. This situation led Rohman8 to conduct a narrative review of the relationship between MD and AAS use, and he concluded that, although there is sufficient evidence that AAS use is more frequent in the presence of the disorder, it is not true that MD can predict the use of AAS. However, given the epidemiological, nosological and clinical relevance underlying the understanding of this relationship, the general objective of this research is to conduct a systematic review of the studies that, during the last decade, have analysed the relationship between MD and ESU, considering the following premises: (a) interest on the topic has increased over the last decade, so the spectrum of existing evidence will be greater; (b) the study of this relationship is not limited to that of a predictive approach, but will involve evidence of different levels and scopes, and (c) ES that lead to an increase in muscle mass are not limited to AAS, so it has therefore been deemed appropriate to broaden the spectrum of substances to be taken into account.
Methods
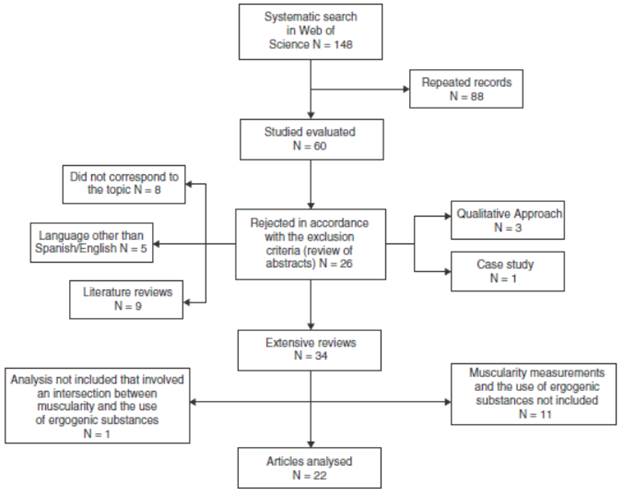
In general, the procedure for searching and selecting articles was guided by the principles of the PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analyses) statement.9,10 The search period ranged from January 2004 to December 2014, and the search was performed from 26 to 30 March 2015, on the Web of Science database, with the terms: muscularity and muscle dysmorphia, in combination with: anabolic androgenic steroids, ergogenic, supplement and performance enhancing substances, in the title, abstract and keywords. Articles were selected based on the fulfilment of four inclusion criteria: (a) that they were empirical; (b) that they were written in English or Spanish; (c) that they included at least one measure and/or indicator of MD and another of ESU, and (d) that some of the data analyses performed involved an intersection between MD and ESU. In addition, three exclusion criteria were considered: (a) dissertations, conferences and presentations; (b) reviews, meta-analyses, case studies or studies with a purely qualitative methodological approach, and (c) studies aimed at the psychometric evaluation of a measure (Fig. 1). The 22 articles retained were analysed based on the following axes: source, purpose, methodology and main findings.
Results
Source
The year with the highest number of published articles (5) was 2012, while the journal with the most inclusions was Body Image, with five. Regarding the country of origin, the United States featured most heavily (77.3%), one article is multinational11 and only one corresponds to Latin America.12 As for authors who have followed the topic, Tom Hildebrandt is worth noting, with five articles.11,13-16
Purpose
Only 13 articles (59.1%) explicitly state the authors' interest in analysing the relationship between MD and ESU, whether in objectives, questions or hypotheses, and although this interest is not explicit in the remaining articles, they included results related thereto.
Methodology
Study type and design. All of the studies are non-experimental and predominantly cross-sectional in nature (95.4%), with only one longitudinal study after 6 weeks.17
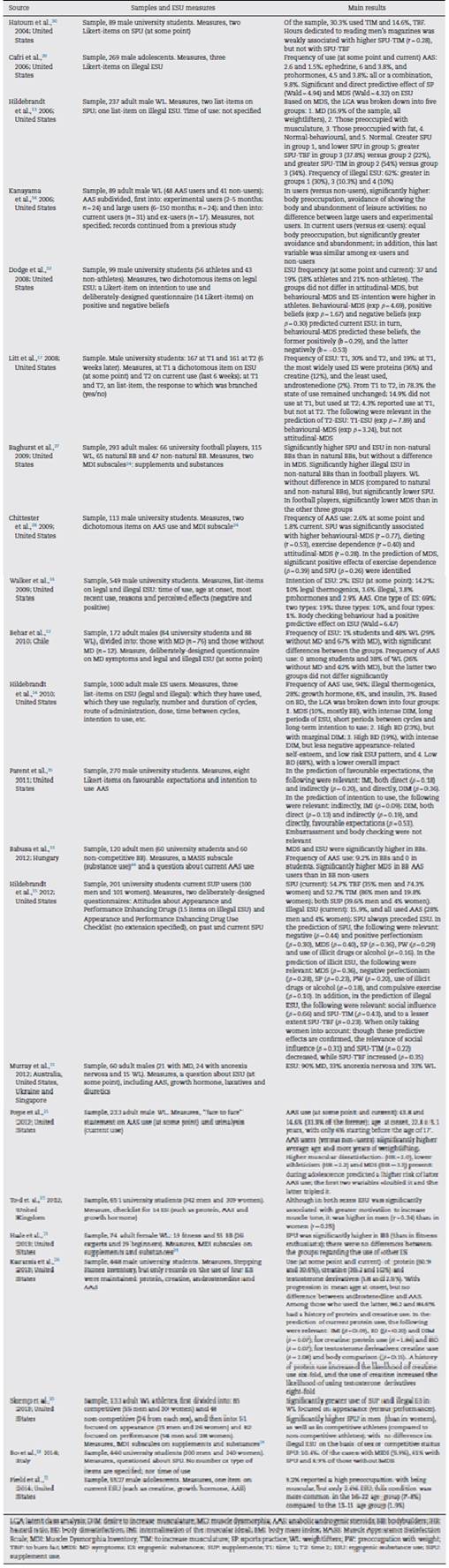
Samples. All are non-probability samples of the intentional or incidental type. The number of participants ranged from 60 to 5527 (Table 1), although the most common size was 101-500, and mainly 201-300 (27.3%); however, three studies (13.6%) included a group with less than 25 participants, of which two included participants diagnosed with MD12-through a self-administered interview-or anorexia nervosa (AN).11 Although five studies included women,15,18-21 only one focused on them.19 As for the type of participants, university students were predominant (59.1%), followed by weightlifters (45.4%). It is important to note that only five studies mentioned the sample recruitment process, which was: through advertisements placed in gyms or nutritional product stores13,28 or through electronic media, such as websites,14,27,28 forums27 or email.32

Instruments and/or measures. In general, the greater use of self-applied scales, mainly the Likert-type, stands out. To evaluate the correlates of MD, the most widely used instruments were: Drive for Muscularity Scale (DMS) (31.8%),22 Muscle Dysmorphic Disorder Inventory (MDDI) (27.3%)23 and Muscle Dysmorphia Inventory (MDI) (18.2%).24 As for another type of scale, in one study13 a silhouette scale was used, the Bodybuilder Image Grid (BIG)23 and two conducted diagnostic interviews for MD: one based on the Body Dysmorphic Disorder Modification of the Yale-Brown Obsessive Compulsive Scale (BDD-YBOCS)25 and another designed for that purpose.12 In order to evaluate ESU or its correlates (as current or past use, intention to use), 13 studies (63.6%) used deliberately-designed items and, of these, nine only used 1-3 items (Table 2). As for specific measures of ESU, only the Stepping Stones Inventory is identified.26 However, it is worth noting the fact that the MDI24 was used in four articles,19,20,27,28 fulfilling two tasks: on the one hand, to measure the presence of MD symptoms and, on the other, to evaluate ESU with two of its subscales (supplements and pharmacological substances). Therefore, the heterogeneity of indicators used in the measurement of ESU is remarkable, a situation that could respond to: (a) the aspect examined: use (17 items), intention to use (3), positive effects of use (4) and negative effects of use (1); (b) excessive specificity or lack of specificity as to the substances considered, which can range from evaluating specific ES (such as protein) to more or less specific sets (such as supplements), but in any case the most widely examined ES are illegal (9 items), and in particular AAS (8); (c) the multiplicity of ESU temporality indicators: at some point (10 articles), current (9) or not specified (5), and (d) the variability in the criterion for defining current use, which was only specified in three articles, ranging from in situ measurement (by urine analysis),25 to the last 30 days29 or the last 6 weeks.17
Scope of the study. Taking into account the type of data analysis performed, predictive (50%) and comparative (40.9%) studies were predominant, with only two correlational studies.21,30
Main results
Frequency of ergogenic substance use
Of the 22 articles, 66.7% estimated the frequency of ESU (Table 2). In university students, the percentage of ESU (at some point/legal and illegal) ranges from 1%12 to 30%,17 in8creasing in weightlifters (33-48%) and even more so in those with MD (67-90%).11,12 With regard to current ESU, in university students this was estimated at 19%,17 which is substantially higher than in adolescents (2.4-8%).31 Taking into account legal ESU (at some point), the frequency did not differ according to sports practice (18% of athletes versus 21% of non-athletes)32; however, it did differ based on the presence/absence of MD symptoms (61 vs 10.4%, respectively)18 or gender, since the use of supplements to increase musculature by men doubled that of thermogenics (30.3 vs 14.6%),30 a tendency that is inverted in women.15 Finally, for specific supplements, protein is the most commonly used substance (at some point), with a frequency among men that ranges from 36 to 60.9%, followed by creatine (12-36.2%). Moreover, a progression in the age of onset is identified, a condition that seems to extend to illegal ESU. (17,26 With respect to the latter, in male and female supplement users who, because of this condition, are considered to be at a higher risk, the frequency was 15.9%,15 and with regard to the use of specific substances, in adolescents and university students the following are reported: ephedrine, 3.8-6%29; testosterone derivatives, 2-5.8%,26 and prohormones, 3.8-4.5%.16,29 However, special mention should be made of AAS, and this is evidenced by the fact that they were taken into account in 60% of the articles that estimated an indicator of consumption frequency. In adolescent and university males, the percentage of use ranges from 0 to 3.3%,12,16,26,28,29,33 while in supplement users it can reach 4% of women and 28% of men.15 Finally, in weightlifters, it stood at between 9.2 and 43.8%.11,12,25,33
Characterisation-comparison between samples
In addition to frequency comparisons, the authors have also been interested in examining the intersection between MD and ESU, considering them as grouping variables. In this sense, 9 of the 22 articles show some comparison between groups (Table 2). In women, although the use of supplements was greater among bodybuilders than among fitness enthusiasts, there was no difference in the use of other ES.19 In male university students, on comparing athletes and non-athletes, it was found that although the former presented more behaviours aimed at muscle gain and a greater ESU intention, the groups did not differ in their desire to increase musculature.32 Moreover, although bodybuilders and university students differed (in the expected direction) regarding all symptomatic indicators of MD, including ESU, this was not the case in muscle satisfaction.33 In light of this, Skemp et al.20 underpinned the relevance of considering the motivation underlying the exercise, as they found that the use of supplements and illegal ES was greater among athletes focused on appearance rather than performance.
However, the complexity of the phenomenon has inevitably led to a comparison between more than two groups. Thus, although it has been found that MD symptoms are significantly more present among weightlifters (such as bodybuilders) than in university football players, the illegal ESU present in these was comparable to that estimated in non-natural bodybuilders.27 These results indicate that ESU does not respond unequivocally to the presence of MD symptoms, or at least not when this is assessed by combining attitudes and behaviours. In this sense, even though initially Kanayama et al.34 identified that three correlates of MD (body preoccupation, avoidance of showing the body and abandonment of leisure activities) were more present in the AAS users than in non-users, on subdividing the former based on the extent (experimental versus large users) and time of use (current vs ex-users), they found that two behavioural correlates were reactive, but not attitudinal. As such, given the heterogeneity brought about by the intersection between MD and ESU, other studies have opted to identify which groups are underlying, on the one hand, for weightlifters13 and, on the other, ES users.14 Regarding the former, based on the symptoms of MD, five groups were created:
Preoccupation with being muscular.
Preoccupation with fat.
Normal behaviour (but not attitude).
Normal.
For the latter, based on body image, four groups were created:
High body dissatisfaction not focused on muscularity.
High body dissatisfaction focused on muscularity.
Low body dissatisfaction with ESU, which stands out in groups 1 and 2. but particularly in the first.
Association-prediction between muscle dysmorphia and ergogenic substance use
As for the association between MD correlates and those of ESU, or of the predictive capacity of the former over the latter, 11 articles included some analysis that was conducive to such purposes (Table 2), the results of which can be grouped under three items:
Socio-cultural influences. In men, reading more male magazines was associated with a greater use of supplements to increase musculature, but not thermogenics30; in addition, social influence proved relevant in ESU prediction15 and, more specifically, the internalisation of the muscular ideal predicted greater protein use26 and more favourable expectations regarding and intention to use AAS.35
Body image. It has been identified that preoccupation,15 dissatisfaction, comparison26 and body checking16 predict ESU (legal and illegal); however, it should be noted that one study did not find the latter behaviour to be relevant in predicting favourable expectations or intention to use AAS.35
MD symptoms. In general, considering both their attitudinal and behavioural dimensions, it is agreed that MD symptoms have a predictive effect on ESU.15,25,29 Regarding the attitudinal dimension, although it has been documented that said symptoms are associated with greater ESU21,28 and predict more favourable expectations and a greater intention to use AAS,35 the only longitudinal study analysed did not find that the desire to increase musculature present at time 1 predicted ESU at time 217; however, in terms of the behavioural dimension, it was found that they are associated with more favourable beliefs,32 intention to use and ESU28,32 and, more particularly, that excessive exercise is associated with increased supplement use28 and that practising sports predicts ESU.15,29
Moreover, Cafri et al. (15 warn that the MD symptoms also act as mediators of the predictive effect of other variables regarding ESU, such as: body mass index, advertising influence and body dissatisfaction. Likewise, it is important to note that in the prediction of ESU, the iatrogenic effect of the use of these substances could also have an effect; for example, it has been documented that the use of supplements makes later illegal ESU more likely, (15,26 albeit with a certain degree of distinction between the sexes, since in men the use of supplements to increase musculature was more relevant and, in women, that of thermogenics.15
Discussion
This review shows the relationship between MD and ESU to be a topic that is largely unexplored in Hispanic America; moreover, it is important to note that, although a total of 22 articles were defined, which would indicate that, on average, two articles were published per year during the last decade, the interest in analysing this relationship was only explicit in just over half. With respect to their methodology, practically all of them are non-experimental, cross-sectional studies, based on intentional samples, predominantly university students. This situation is contrary to that documented by Suffolk et al.,36 who analysed the methodological characteristics of the articles published on MD between 1993 and 2013, and found that the majority had focused on samples of bodybuilders or weightlifters. In addition, it is notable that in the selection of their participants, the researchers pondered at least one of three items: gender (predominantly men), exercise (mainly weightlifting) and ESU (mostly AAS), which in turn resulted in the inclusion of multiple comparison groups and subgroups. Therefore, although the heterogeneity of the samples, groups and subgroups examined, which range from community to clinical samples, including those with different levels of presumed risk, is noteworthy, university students have been most widely examined. There are two reasons as to why this may be the case: on the one hand, it is considered that during late adolescence and early youth we begin to consolidate most of our lifestyle habits37 and, on the other, the undeniable fact that university students usually constitute easily accessible samples.
In relation to the measures aimed at evaluating the MD correlates, the increased use of two of them-DMS and MDDI-is noteworthy; although both instruments are widely used around the world, the former also has a large body of evidence supporting its reliability and validity.38-41 As a counterpart, the great heterogeneity of parameters or indicators that have been used in the evaluation of ESU is worrying, which has been mostly based on a very small number of items (between 1 and 3); or, for example, the very delimitation of the legality or illegality of an ES proves somewhat unclear, so it is recommended that future research specify which substances are considered illegal or that the laws applied be indicated. Therefore, an initial problem to be solved is the formulation of ESU parameters, indicators and measures, since, although important progress is identified in the development of measures aimed at evaluating the symptoms and correlates of MD, this does not make ESU extensive.
The only measure that showed a certain constancy of use among the studies is the MDI, an instrument, whose origin and purpose, however, are based on the measurement of MD symptoms, and not on ESU. It will therefore be necessary to evaluate whether or not this condition assumes a bias when evaluating the relationship between MD and ESU, when the same approach of the items maybe presupposing it. Moreover, in terms of the scope of the research, it is noteworthy that, in terms of the statistical analysis applied to the data, 40% was predictive, thus revealing that interest in identifying its feasible aetiological relationship has increased over the last decade.
Summarising the meticulous methodological analysis performed in this review, it is possible to discern a certain pattern that characterises the bulk of the studies: (a) cross-sectional studies; (b) non-probability samples; (c) intentional selection; (d) based on male university students, and (e) use of self-applied measures, mainly deliberately-designed items. In turn, there are also some methodological limitations, such as: (a) not mentioning the recruitment system; (b) continuing records from previous studies without complete data,34 and (c) using self-administered interviews to diagnose MD. These are some methodological aspects to be solved in future research, taking into account that aspects such as these define the methodological quality of the research conducted.
Now, in spite of the methodological variations and limitations, the results documented in relation to the frequency of ESU shed light on certain relevant aspects: (a) the feasible existence of a pattern of progression in ESU, which goes from legal substances at one end to illegal, with AAS at the other, thereby underpinning the relevance of extending the spectrum of ES to be examined, also taking into account that people usually use more than one16,29; (b) in men, although ESU is considered in order to increase muscle mass, it may coexist with the use of other substances aimed at burning fat, (4,42 confirming not only the general complexity of studying behaviours for effecting body change, but also specific ESU; (c) although practising sports does not seem to be related to a higher frequency of ESU, the evidence indicates that weightlifting does, which underlines the importance of analysing the reason behind participating in exercise (appearance vs performance), assuming that, although in both the function is to achieve a change in body structure or composition, the two purposes do not necessarily converge, and (d) it is evident that the presence of a MD diagnosis does not presuppose ESU, but it does make it likely, so that 7-9 out of 10 patients with MD have used an ES and 4 out of 10, an AAS.
However, other aspects are noteworthy among the results of the sample characterisation-comparison: (a) the attitudinal MD correlate does not show the capacity to differentiate between ES users and non-users, but the behavioural one, which indicates the need to evaluate these correlates differently, does36,43; (b) weightlifters and, more specifically, bodybuilders, represent two samples at a greater risk of MD and ESU, and (c) in the context of MD, ESU (mainly illegal) is a clinically relevant behaviour for effecting body change.
Finally, with regard to the predictive relationship between MD and ESU, this was only examined in nine articles, and it is clear that research concerning the topic is incipient. Nevertheless, according to the documented data, exclusively considering the results that coincide between at least two studies, four variables have proven relevant in the prediction of ESU: the internalisation of the muscular ideal, body preoccupation/dissatisfaction, MD symptoms and sports practice, and the finding that the use of supplements makes illegal ESU likely is also notable.
Conclusions
Although ESU is not a problem exclusive to men, weightlifters or bodybuilders, the presence thereof is confirmed to be predominant among them. Moreover, it is evident that substances used for the purpose of developing muscle mass are not limited to AAS, but comprise a wide range which includes those generally referred to as supplements and which are erroneously considered to be harmless. Therefore, there is an imminent need to work on the formulation of strategies that not only seek to influence the promotion of a healthy body image, and to thus prevent MD, but also awareness about the risks that in the medium and long term can lead to the use and, above all, abuse of ES.
Moreover, it is noteworthy that, despite the nosological relevance that ESU can have for MD, the number of research studies aimed at analysing its predictive relationship is scant. In addition, although it is clear that ESU is not present in all patients with MD and that not all users of these substances have MD, both conditions coexist in a high proportion of cases, which highlights the need for future research to define the clinical significance ESU in the context of MD.
In general, although this review is based on a growing interest in identifying the relationship between MD and ESU, the results obtained to date are still uncertain, mainly as a result of the lack of clarity and lack of consistency in the definition of indicators, parameters and measures used in and between the different studies. Therefore, one pressing need to overcome is to use ESU measures with adequate reliability and validity properties. Finally, it is important to point out two important limitations of this research: firstly, restricting the literature search to a single database and, secondly, limiting the selection of articles to those written in English or Spanish.

