










Services on Demand
Journal
Article
 Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista de la Facultad de Medicina
Print version ISSN 0120-0011
rev.fac.med. vol.62 no.1 Bogotá Jan./Mar. 2014
https://doi.org/10.15446/revfacmed.v62n1.43780
http://dx.doi.org/10.15446/revfacmed.v62n1.43780
CASOS CLÍNICOS
Dysphagia Lusoria and Zenker's Diverticulum
Dysphagia Lusoria y Diverticulum de Zenker. Reporte de caso
Julian D. Martinez1,2 • Luis F. Maya2 • Martin Gomez1 • Jorge Lizarazo3 • Mario H. Rey3 • Martin Garzon3 • Juan C. Marulanda3 • Juan C. Molano3 • Renzo Pinto3
1 Departamento de Medicina Interna. Universidad Nacional de Colombia. Bogotá, Colombia.
2 Fundación Universitaria Juan N. Corpas. Bogotá, Colombia.
3 Hospital Universitario de la Samaritana. Bogotá, Colombia.
Correspondence: Julian D. Martinez. Unidad de Gastroenterología, Hospital Universitario de la Samaritana, Carrera 8 No. 0-55 Sur, Bogota, Colombia. Telephone: 571-2804512. FAX: 571-2711772. E-mail: jdmartinezm@yahoo.com
Recibido: 11/12/2013 / Aceptado: 10/3/2014
Summary
An 81-year-old woman was referred for evaluation of dysphagia which she had suffered for four years. An upper gastrointestinal endoscopy revealed a Zenker's diverticulum and extrinsic compression of the esophagus. A thoracic CT scan confirmed the presence of extrinsic compression caused by an aberrant right subclavian artery, which compromised the posterior esophageal wall thus confirming a diagnosis of dysphagia lusoria. An association between Zenker's diverticulum and dysphagia lusoria is so uncommon that there have been no previously published cases.
Key words: Zencker Diverticulum, Deglutition Disorders, Case Studies (MeSH).
Resumen
Una mujer de 81 años fue remitida para evaluación de una disfagia que padecía desde hacía cuatro años. Una endoscopia gastrointestinal reveló un divertículo de Zenker y una compresión extrínseca del esófago. Un escaneo computadorizado del tórax confirmó la presencia de la comprensión extrínseca, causada por una arteria subclavia derecha aberrada, que comprometía la pared esofágica posterior, lo que confirmó un diagnóstico de disfagia lusoria. Una asociación entre el divertículo de Zenker y la disfagia lusoria es tan poco común que no han sido publicados sus casos con anterioridad.
Palabras clave: Divertículo de Zenker, Trastornos de Deglución, Estudios de Casos (DeCS).
Introduction
Dysphagia is the sensation that swallowing is difficult or impossible. The word derives from the Greek roots dys, which means difficulty, and phago, which means to eat. In the broadest sense, dysphagia includes any mechanical or functional alteration in the passage of solids and/or liquids between the mouth and the stomach. However, this can be differentiated into odynophagia, which is painful swallowing, and globus pharyngis which is the sensation of having a lump in one's throat (in the pharynx or cervical esophagus). Dysphagia is an important cause of morbidity and mortality that can cause dehydration, malnutrition, laryngeal spasms, bronchial spasms, pneumonia related to aspiration and death due to obstructed air passages. It occurs frequently: it presents in 10% of people over the age of 50 years, in 25% of elderly people hospitalized for any reason, and in 40% of the patients in geriatric institutions (1-3).
Case report
An 81-year-old woman came to the gastroenterology service after suffering from dysphagia for four years. Dysphagia was initially associated with solid foods, but six months prior to consultation the patient began to feel as if a foreign object was lodged behind her sternum. Patient had halitosis and occasional difficulty breathing, but did not report weight loss.
After an upper gastrointestinal endoscopy performed at a local hospital, a Zenker's diverticulum was founded. The patient had been referred for endoscopic septotomy. An important factor reported in the patient's medical history was her systemic arterial hypertension managed with losartan. Physical examination showed oropharyngeal erythema but no other alterations.
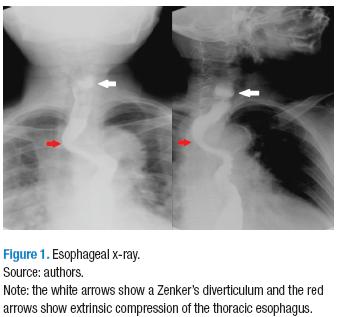
At the Hospital Universitario de La Samaritana (HUS-Samaritan Teaching Hospital), an esophageal x-ray showed a diverticular formation 20mm x 17mm in the cervical esophagus, indicated by a white arrow in Figure 1. The red arrow indicates extrinsic compression in the posterior wall of the thoracic esophagus at the top of the aortic arch together with multiple tertiary contractions in the distal third of the organ, which are compatible with an aging esophagus.
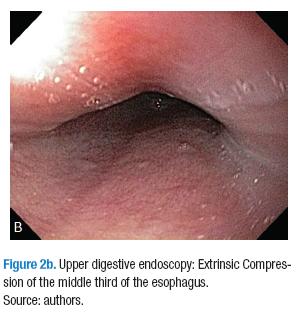
An esophageal endoscopy confirmed the presence of a diverticulum in cervical esophagus (Figure 2a) and extrinsic compression of the middle third of the posterior wall of the esophagus (Figure 2b).

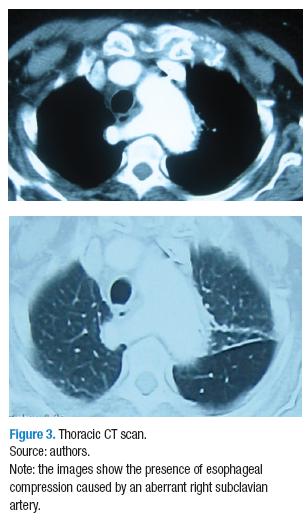
The images showed extrinsic thoracic compression, and a thoracic CT scan was ordered to rule out the possibility of mediastinal pathology. The scan showed changes in the morphology of the descending aorta. An aberrant right subclavian artery compromised the posterior esophageal wall, confirming the presence of dysphagia lusoria (Figure 3).
Dysphagia lusoria
Dysphagia lusoria refers to dysphagia caused by extrinsic compression of the esophagus by mediastinal vascular structures. An aberrant right subclavian artery is the alteration associated with this condition which has been described most often in the literature. It is also the congenital malformation most often associated with the aortic arch. It has a prevealence of 1.8% (4). Other vascular malformations which cause extrinsic compression with dysphagia or respiratory symptoms include double aortic arches, persistent right aortic arches with patent ductus arteriosus, and aberrant innominate arteries (5-7).
In 1761, David Bayford, an English surgeon, described the case of an elderly woman who had died of severe malnutrition because of "obstructed deglutition". He subsequently performed an autopsy on the woman and found that the cause of the obstruction had been an enlarged right subclavian artery that originated on the left side of the aortic arch and then crossed toward the right arm between the trachea and the esophagus causing esophageal compromise. He finally presented this case to a meeting of the medical society of London in 1787 (8).
The normal anatomy of the aortic arch characterize by three great branches: the left common carotid artery, the left subclavian artery, and the brachiocephalic artery. The brachiocephalic artery passes upwards, outwards and behind the left brachiocephalic vein and in front of the trachea. Finally, it divides into the common carotid artery and the right subclavian arteries at the sternoclavicular joint. The dysphagia lusoria (in the case presented) was the result of abnormal development of the aortic arch into four branches whose origins were separated by the right common carotid artery and the right subclavian artery resulting in a trajectory behind the esophagus, which caused the extrinsic compression.
This alteration can be asymptomatic. In such cases, its diagnosis is likely to be incidental to a thoracic imaging study. During infancy, dysphagia lusoria may manifest itself as a combination of dysphagia and dyspnea while among adults its symptoms are most often dysphagia associated with solid foods (7).
The initial evaluation of patients should include barium X-rays of the esophagus (esophograms), thoracic CT scans, and complementary esophageal endoscopy (9). CT scans are indicated for patients with suspected mediastinal alterations such as those whose angiographs have demonstrated aberrant blood vessels. Modern multi-slice 3D CT scanning is now the diagnostic technique of choice both because of its high resolution and because it is not invasive. (10,11)
Zenker´s diverticulum
Zenker´s diverticulum, also known as pharyngoesophageal diverticulum, occurs most frequently among the elderly. It is the formation of a pouch in the upper esophageal sphincter, which obstructs the passage of food. Although it was first described by Ludlow, it takes its name from German physician Friedrich A. von Zenker who published an article about it in 1877 that included a series of 27 cases with complete descriptions of its clinical and pathological characteristics. He defined it as a herniation of the mucosa of the posterior hypopharyngeal wall extending through the muscle layer (12).
Esophageal diverticula classifies into three types according to their locations. Zenker´s diverticula are those pharyngeal herniations that occur within Killian's dehiscence, a weak area in between the thyropharyngeus part of the inferior constrictor of the pharynx and the cricopharyngeus muscle. Middle third esophageal diverticula are located down to 5 cm below the tracheal carina while epiphrenic diverticula occur in the lower 10 cm of the organ (13).
Failure of coordination related to either the superior or the inferior sphincter can produce increased intraluminal pressure, protrusion of the mucosa, and diverticula. Increased hypopharyngeal pressure can cause Zenker's diverticula, just as abnormal traction or pushing of the esophagus can produce diverticula in the middle and lower thirds of the esophagus.
The prevalence of esophageal diverticula in the whole population is estimated to be between 0.02% and 0.77% although the majority of diverticula do not present symptoms. At least 3% of all dysphagia patients are diagnosed with diverticula. The majority of these cases occur among elderly patients who visit the doctor because of severe halitosis, laryngeal symptoms and respiratory symptoms (13,14).
Although Zenker's diverticula are pulsion diverticula, the cause of high hypopharyngeal pressure and lack of coordination of the superior esophageal sphincter during swallowing cannot be identified in the majority of patients. Nevertheless, various theories postulate the cause as a constrictive myopathy of the sphincter combined with spasms of the sphincter. This type of diverticulum has been reported to be associated with various illnesses that, in one way or another, produce alterations of the normal movement of the esophagus and increase intraluminal pressure in the esophagus. These pathologies include gastric, esophageal and laryngeal neoplasias, esophageal rings in the upper third of the esophagus, Chagas disease, systemic diseases such as poliomyelitis, and anatomical defects such as hiatal hernias, reported in more than 30% of these patients (15-22).
Diagnosis base upon clinical evidence and confirmed with a barium esophogram that will show an accumulation of the contrast medium in the proximal third of the esophagus. In some cases, endoscopy of the upper digestive tract may be useful for detection of this abnormality (13). Treatment should usually be conservative and based on life style changes for patients with multiple comorbidities, small diverticula, or few symptoms. On the other hand, cricopharyngeus myotomies, either endoscopic or surgical, may be indicated to divide the septum and allow the passage of food around the diverticulum and through the esophagus (23-25).
Discussion
No cases of dysphagia lusoria associated with Zenker's diverticulum have been previously reported in the literature of the world. In 1965 Schermuly reported on a cased of Zenker's diverticulum associated with achalasia in Germany. Two decades later Schwartz and cols., postulated that achalasia and esophageal rings could cause pharyngeal protrusions such as Zenker's diverticula. They proposed that these pathologies should be ruled out before deciding upon any treatment of these cases. One of the author's of this article has reported on a case in which Zenker's diverticulum was associated with achalasia (26). Persistence of the motor disorder generated by achalasia is conducive toward increased intraluminal pressure in the esophagus followed by development Zenker's diverticulum, worsening dysphagia and increased risk of bronchial aspiration.
As the population of elderly people in Colombia grows, the number of patients with dysphagia due to various causes will increase. This will require well informed physicians who are prepared to perform the appropriate studies to establish correct and precise diagnoses and offer the best solutions available in our environment in an opportune manner.
Conflict of interest
None declared by the authors.
Funding
Supported by the Hospital Universitario de La Samaritana, Bogotá, Colombia.
Acknowledgements
None declared by the authors.
Referencias
1. Castell D, Donner MW. Evaluation of Dysphagia : a careful history is crucial. Dysphagia. 1987;2:65-71. [ Links ]
2. Sivarao DV, Goyal RK. Functional anatomy and physiology of the upper esophageal sphincter. Am J Med. 2000;108(Suppl 4a):27S-37S. [ Links ]
3. Palmer J, Drennan J, Baba M. Evaluation and treatment of swallowing impairments. Am Fam Physician. 2000;61:2453-62. [ Links ]
4. Mc Loughlin MJ, Weisbrod G, Wise DJ, Yeung HP. Computed tomography in congenital anomalies of the aortic arch and great vessels. Radiology. 1981;131:399-403. [ Links ]
5. Edwards JE. Congenital malformations of the heart and great vessels. Malformations of the thoracic aorta. In Gould SE, ed. Pathology of the Heart, 2nd ed. Springfield: Charles C Thomas; 1960. p. 391-462. [ Links ]
6. Álvarez JR, Quiroga SJ, Nazar AB, Comendador MJ, Carro, GJ. Aberrant right subclavian artery and calcified aneurysm, of Kommerell's diverticulum: an alternative approach. J Cardiothorac Surg. 2008;3:43-9. [ Links ]
7. Levitt B, Ritcher JE. Dysphagia lusoria: a comprehensive review. Dis Esophagus. 2007;20:455-60. [ Links ]
8. Asherson N. David Bayford. His syndrome and sign of dysphagia lusoria. Ann R Coll Surg Eng. 1979;61-67. [ Links ]
9. Muñoz A, Obregón J, Salej JE, Jiménez JM. Dysphagia lusoria: A case report and review of the literature. Revista Colombiana de Gastroenterología. 2009;24:396-402. [ Links ]
10. Gareth J, Owens PE, Roobottom CA. Aberrant right subclavia artery and dysphagia lusoria. N Eng J Med. 2002;347:1532 [ Links ]
11. Kantarceken B, Bulbuloglu E, Yuksel M, Centikaya A. Dysphagia lusoria in elderly: A case report. World J Gastroenterol. 2004;10:2459-60. [ Links ]
12. Herbella FAM, Matone J, Del Grande JC. Eponyms in esophageal surgery, part 2. Dis Esophagus. 2005;18:4-16. [ Links ]
13. Thomas ML, Anthony AA, Fosh BG, Finch JG., Maddern GJ. Oesophageal diverticula. Br J Surg. 2001;88:629-42. [ Links ]
14. Greenwald E, Rawlinson JD, Marshall JK. A distinctive case of dysphagia. JAMC. 2004;170:42. [ Links ]
15. Johnson JT, Curtin HD. Carcinoma associated with Zenker`s diverticulum. Ann Otol Rhinol Laryngol. 1985;94:324-25. [ Links ]
16. Birt BD. Dysphagia due to simultaneous laryngocele and Zenker`s diverticulum. Laryngoscope. 1985;95:1-2. [ Links ]
17. Mercer CD, Hill LD. Esophageal web associated with Zenker`s diverticulum. Can J Surg. 1985;28:375-76. [ Links ]
18. Low DE, Hill LD. Cervical esophageal web associated with Zenker`s diverticulum. Am J Surg. 1988;56:34-7. [ Links ]
19. Georgalas C, Baer ST. Pharyngeal pouch and polymiositis: association and implications for aetiology of Zenker`s diverticulum. J Laryngol Otol. 2000;114:805-7. [ Links ]
20. Gage-White L. Incidence of Zenker`s diverticulum with hiatus hernia. Laryngoscope. 1988;98:527-30. [ Links ]
21. Dantas RO. Diverticulo de Zenker em paciente com esofagopatia chagasica. Arq. Bras. Med. 1983;57:78-80. [ Links ]
22. Sasaki CT, Ross DA, Hundal J. Association between Zenker diverticulum and gastroesophageal reflux disease: development of a working hypothesis. Am J Med. 2003;115(Suppl 3A):169S-71S. [ Links ]
23. Minecci PC, Mathisen DJ. Modified diverticulectomy and myotomy for recurrent Zenker diverticulum. J Thorac Cardiovascular Surg. 2003,125:969-71. [ Links ]
24. Takes RP, van den Hoogen FJ , Marres HA. Endoscopy myotomy of the cricopharyngeal muscle with CO2 laser surgery. Head Neck. 2005;27:703-9. [ Links ]
25. Gómez MA, Ardila SF, Arbeláez V. Experience in the treatment of Zenker`s diverticulum: a series of 18 cases. Revista Colombiana de Gastroenterología. 2011;26:98-103. [ Links ]
26. Martinez JD. Zenker´s diverticulum and acalasia. rev.fac.med. 2008;56:65-70. [ Links ]
