










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista de la Facultad de Medicina
Print version ISSN 0120-0011
rev.fac.med. vol.62 no.4 Bogotá Oct./Dec. 2014
https://doi.org/10.15446/revfacmed.v62n4.43489
DOI: http://dx.doi.org/10.15446/revfacmed.v62n4.43489
ORIGINAL RESEARCH
Barriers of access to oral health care among university students in southern Colombia, 2011. A multivariate analysis
Barreras de acceso a los servicios de salud bucal en estudiantes universitarios del sur de Colombia, 2011. Un análisis multivariado
Anderson Rocha-Buelvas1, Arsenio Hidalgo-Troya2, Ángela Hidalgo-Eraso3
1 Facultad de Odontologia, Universidad Antonio Narino. Bogotá, Colombia.
2 Facultad de Ciencias Exactas y Naturales, Universidad de Nariño. Nariño, Colombia.
3 Empresa Promotora de Salud EMSSANAR. Nariño, Colombia.
Correspondence: Anderson Rocha-Buelvas. Cra 14A No.70A-34. Posgrados en Salud. Fundación Universitaria del Área Andina. Telephone: +57 300 8934073. Bogotá, Colombia. E-mail: rochabuelvas@gmail.com.
Received: 15/05/2014 Accepted: 19/08/2014
Summary
Background. The right to health is considered to be a fundamental human right. Therefore, it is a starting point from which to combat unjust and immoral inequalities. It is essential to study the process through which a need for attention is completely satisfied.
Objective. To analyze determinants of access to oral health care among university students in municipality of Pasto.
Materials and methods. A sample of 338 university students answered a confidential survey that was based upon previous studies using a health care services utilization behavioral model.
Results. In terms of enabling factors, the students that responded as ‘having a bad health state’ were those that used oral health care services the most in last year, while those students that responded as "being dissatisfied with the appearance of their teeth’ used oral health care services less. In relation to need factors, the students whose quality of life was not affected by physical impairment and physical pain used oral health care services less. Predisposing factors were not statistically significant.
Conclusions. This study found that enabling and need factors were associated with recent dental consultations by university students in the municipality of Pasto.
Keywords: Health services accessibility; Equity in health; Student health services, Social determinants of health; Oral health; Colombia (MeSH).
Rocha-Buelvas A, Hidalgo-Troya A, Hidalgo-Eraso Á. Barriers of access to oral health care among university students in southern Colombia, 2011. A multivariate analysis. Rev. Fac. Med. 2014;62(4):521-8. http://dx.doi.org/10.15446/revfacmed.v62n4.43489.
Resumen
Antecedentes. El derecho a la salud es considerado un derecho humano fundamental, por tanto, es un principio para combatir las desigualdades –injustas e inmorales–. Así, es fundamental estudiar el proceso mediante el cual una necesidad de atención se satisface completamente.
Objetivo. Analizar los determinantes de acceso a los servicios de salud bucal en estudiantes universitarios del municipio de Pasto.
Materiales y métodos. En una muestra de 338 estudiantes universitarios se aplicó una encuesta confidencial utilizando un modelo comportamental de uso de servicios de salud.
Resultados. Sobre los factores de capacidad, los estudiantes que respondieron tener mal estado de salud utilizaron más los servicios de salud bucal en el último año, mientras que los que reportaron estar insatisfechos con la apariencia de sus dientes utilizaron menos los servicios. Respecto a los factores de necesidad, los estudiantes que no tienen afectada su calidad de vida por incapacidad física y dolor físico utilizan menos los servicios de salud bucal. Los factores predisponentes no arrojaron resultados significativos.
Conclusiones: Este estudio encontró que los factores de capacidad y de necesidades estaban asociados con la consulta odontológica reciente en estudiantes universitarios del municipio de Pasto.
Palabras clave: Accesibilidad a los servicios de salud; Equidad en salud; Servicios de salud para estudiantes; Determinantes sociales de la salud; Salud bucal; Colombia (DeCS).
Rocha-Buelvas A, Hidalgo-Troya A, Hidalgo-Eraso Á. Barreras de acceso a los servicios de salud bucal en estudiantes universitarios del sur de Colombia, 2011. Un analisis multivariado. Rev. Fac. Med. 2014;62(4):521-8. http://dx.doi.org/10.15446/revfacmed.v62n4.43489
Introduction
Despite the existence of very concrete cases in Colombia that have shown that inequity in oral health services in the population is persistent, studies that have examined inequalities in access and use of oral health services suggest positive advances in aspects like financing, affiliation to the system, and potential access. This, however, is not the case for real access to services (1-5). As a result, to analyze access to health services, research in public health has leaned on Andersen’s behavioral model of health service use. This model should be analyzed based on the current use of health care services and user satisfaction with them.
While research into social inequity in oral health is substantial in developed countries, it is scarce in developing countries. This inequity can be seen in Colombia where structural problems with oral health care are not very different between regions, and where educational level, occupation, the lack of money, and insurance, among other factors, can all constitute barriers of access to health services. As such, a representation of the university population in southern Colombia is the object of this study because, in addition to being rarely approached and studied, it is diverse, given that it is made up of individuals from varying socioeconomic strata, ethnic groups, and urban and rural areas of southwestern Colombia.
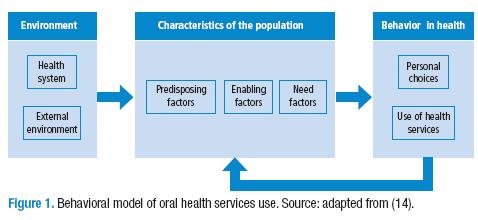
It is worth mentioning that, from the theoretical-operational field, the model identifies the influence both of individual variables (behavioral) and contextual variables (physical, political, or the economic environment). This happens through the identification of the individuals’ determinant factors of access to health care that can affect the reception of medical or dental care (9). These factors include predisposing factors (inherent to the patient and independent of their pathology), mediating or enabling factors (that facilitate or obstruct the use of health services and that are susceptible to changes in health policies), and need factors (the perception of and severity of the symptoms of the disease).
Thus, in practical terms, it is important to analyze these determinant factors with statistical models and to confirm the "inverse care law" (10) that states that populations with greater health needs receive less care, while healthier groups receive more care. These affirmations have been complemented with more recent theories such as what has been called the "inequality paradox" (11), which highlights the existence of subgroups within the subpopulations that, due to the social characteristics that they share, are subject high health risk factors. The identification of groups that are potentially vulnerable to risks is a fundamental aspect in the scientific and political approach to health inequities. Herein lies the importance of this kind of study.
Materials and methods
This study is descriptive and includes analytical prevalence. A confidential survey was used that was created based on previous studies and on Andersen’s behavioral model of health service use (12) (Figure 1) adapted for dentistry by Kiyak (13). A pilot study of 18 surveys was carried out with a provisional version to ensure that it was easily understood. These pilot participants were also asked if the questionnaire lacked any aspects that they considered important.
The survey was administered in the Pasto campus of the Universidad Cooperativa de Colombia, in rooms and at times previously arranged together with the university’s academic direction. The students were systematically chosen from every academic program. The inclusion criteria were: university students studying in the first semester of 2011 in the programs of medicine, dentistry, auxiliary nursing, industrial engineering, law, or accounting. University students attending other higher education institutions in Pasto were excluded.
A probability sampling was performed. The first sampling was stratified according to the percentile distribution of the students by gender, program of studies, and semester. Finally, a quota sampling for each semester was moved forward. Of a population of 1816 students (841 male, 975 female), the prevalence of use of health services for the sample was estimated at 39.6%, according to a study from Pizarro and cols. (15). A sample group of 277 participants was originally obtained. This was later increased by 15% as a safety margin against possible losses of information. This left the sample size at 304 people.
Three groups of exposure variables were established based on the determinant factors of access to oral health services, including: 1) need factors, the result of the review of the OHIP-14 "Oral Health Impact Profile" along with its translation to Spanish (16), 2) predisposing factors, and 3) enabling factors.
In the first group, the variables were: physical discomfort, functional limitations, physical pain, physical impairment, psychological impairment, social impairment, and disability. The second group included gender, age, pertinence to an ethnic group, program of study and semester, marital status, and employment status. Finally, in the third: state of health, state of oral-dental health, dental problems, mental health, satisfaction with teeth appearance, socioeconomic stratus, social support (Duke-11), knowledge of rights in relation to general health. For the outcome variable, we determined if the student "had consulted a dentist in the last 12 months".
Predisposing, enabling and need factors associated with the use of oral health services were identified through bivariate and multivariate analyses with the goal of obtaining an explanatory model from the individual determinants of Andersen’s model. For the multivariate analysis, the binomial logistic regression model was used with the variables that presented a p-value with a significance lower than 0.25, as proposed by Hosmer and Lemeshow. To measure the OR values or the force of association, a multivariate analysis was performed with the logistic regression model and Wald’s test. Confusion and modification of effect were searched for. The analysis was carried out in the program SPSS®, version 17. The data was analyzed independently in males and females.
Results
The significant results in the bivariate analysis (Table 1) were oriented toward two of the determinants of access to oral health services according to Andersen’s model: enabling and need factors. In the realm of enabling factors, of the university students with dental problems, 53% of them responded that they went to a dental consultation in the last year. Meanwhile, 62% of those who did not have dental problems had gone to a dental consultation. It is also worth pointing out that of the university students that indicated having knowledge of their rights to general health care, 60% attended a dental consultation. On the contrary, of those who did not indicate having knowledge of their rights only 52% attended a consultation.
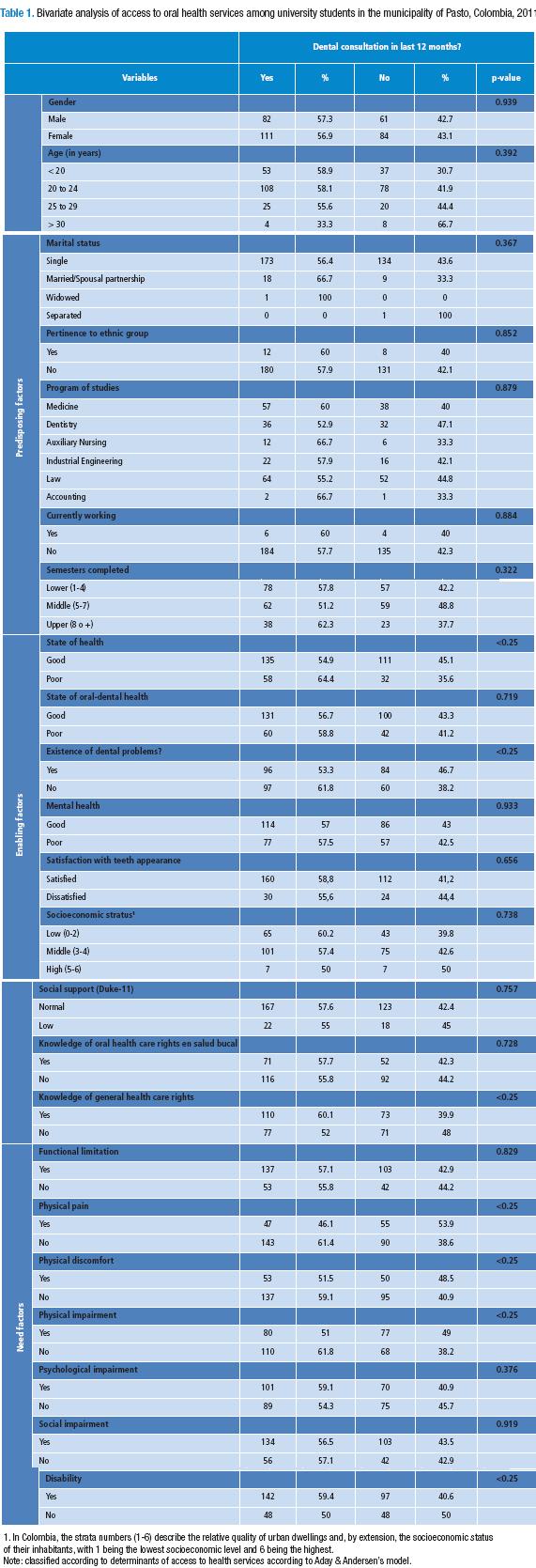
Furthermore, with respect to need factors it was observed that 46% of students had attended a dental consultation when their quality of life is affected by physical pain from poor oral health. Meanwhile 61% of students without physical pain had attended a dental consultation. In Table 1, it can be seen that of those university students whose quality of life was affected by physical discomfort, 52% attended a dental consultation in the last year, while 59% of those whose quality of life was not affected attended a dental consultation. 51% of students whose quality of life had been affected by physical impairment related to oral health attended a dental consultation. However, when this is not the case, 61% of students attend a dental consultation. Of those students whose quality of life is affected due to a disability related to oral health, 59% attend a dental consultation. When no disability exists, 50% attend a dental consultation.
The variables from Table 1 that were chosen for the Hosmer-Lemeshow test were as follows: state of health, dental problems, and knowledge of rights. Nevertheless, all of the variables in Table 1 regardless of their p-value were submitted to Wald’s test with the goal of adjusting them to the model of logistic regression with a p-value of 0.10. The multivariate analysis in table 2 showed that, among the enabling factors, the state of health and satisfaction with the appearance of the teeth have a statistically significant relationship with the use of health care services. For example, university students that report having poor health use oral health services 2.3 times more than those who report having good health, while those who report being dissatisfied with the appearance of their teeth use oral health services 0.4 times less than those who are satisfied with the appearance of their teeth.
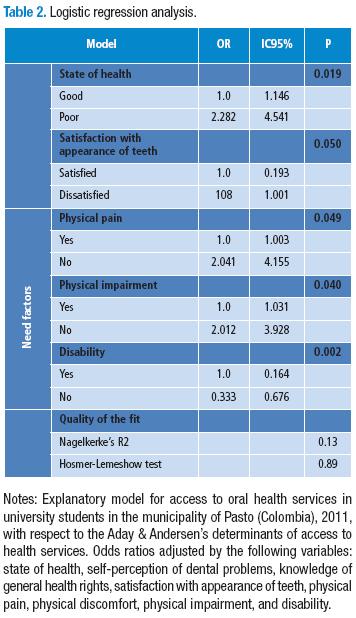
In the multivariate analysis in table 2, the need factors —physical pain, physical impairment and disability— showed a statistically significant relationship to the use of oral health services. Thus, university students who reported that their quality of life was not affected by physical pain and physical impairment are those that use oral health services twice as often as their counterparts who did report negative effects to their quality of life. The opposite occurs in university students who reported that their quality of life was not affected by disability, since they accessed oral health services 0.3 times less than those with disabilities.
Discussion
With regard to enabling factors, the students who reported having a poor state of health are those who used oral health services the most over the last year. Furthermore, a large proportion of the women in the study affirmed that they had poor mental health and emotional affectations. The students who reported being dissatisfied with the appearance of their teeth are those who used oral health services the least in the last year, probably because they do not perceive their own dental problems. When it comes to need factors, the students whose quality of life was not affected by all factors except disability were those who attended dental consultations the most in the last year.
With respect to the enabling factors, the state of health can undoubtedly become a barrier for the access to oral health services, as this study has demonstrated (17). State of health is intimately related to life experience and especially to psychosocial factors. Among these we may include state of health, among many other individual characteristics. This could be motivating students with poor health to attend the recent dental consultation (18). In this way, psychological potential also benefits teeth appearance and even dental cosmetics in current times (19).
Various studies have demonstrated that the negative effects of daily life in adults have a notable influence on oral health. In a related way, satisfaction with the appearance of the teeth can worsen when the individual in question suffers from caries or periodontal disease, conditions that could not be taken into account in this study. We deduce, then, that dissatisfaction with the appearance of the teeth reduces the possibilities of attending a dental consultation in the last year (20), given that expectations play an important role in patient satisfaction.
An example of this can be found in studies where dissatisfied patients, who nonetheless have high or medium expectations, increase their consumption of health services. Patients with low expectations, however, reduced the consumption of services and, as a result, their personal satisfaction also dropped. This evidence suggests that dissatisfaction with teeth appearance can be related to the patient’s values and expectations, since they are subjective aspects. At the same time, they are enabling factors or facilitators of the use of oral health services among students (21).
With respect to need factors, upon revising other studies that use quality instruments related to oral health such as the GOHAI or the OHIP-14 (22), it is reported that dimensions like physical pain and physical impairment tend to affect quality of life and have an impact on the use of oral health services. This explains the results of this study. A study carried out by Dumitrescu and cols., on Romanian university students, shows that recent dental consultations are associated with feelings of satisfaction with life and happiness (23). Therefore, surely the majority of students who are in the middle of pursuing their life projects by studying a university program may be more motivated to make use of oral health services when their quality of life is not affected, especially if we take into account that physical pain and impairment are adverse situations from the psychosocial point of view.
The rate of use of oral health services by university students in the municipality of Pasto is mid-range. However, it is higher than the rate of use of oral health services among adults in developed and developing countries. It is worth pointing out that this behavior might be associated, according to Andersen’s model, with socioeconomic stratus, age, educational level, and with the fact that the students live in an urban area. However, we would also like to highlight that the index of patients with caries, fillings and lost teeth is unfortunately far from Colombia’s national goals (2,3,24), since in 2011 it was at 5.9 (25).
This study verified that enabling and need factors were associated with recent dental consultations in university students in the municipality of Pasto. As such, these results favor the development of strategies by health authorities to improve access to oral health services for the university population, showing the need of fomenting knowledge of oral health rights in the young adult population, and of providing empirical resources for new research alternatives. For example, this study could be carried out in other social contexts that display greater vulnerability from the viewpoint of the social determinants of oral health.
Due to this, we can conclude that the use of oral health services by university students in the municipality of Pasto, Colombia, although high compared to other studies and populations, does not necessarily lead to these individuals having better oral health. As such, a limitation of this study is that the approach to examining the access to services was not sufficient to give explanations based on reasons of health, politics, social factors (distribution of health goods, services, and opportunities), and economic factors.
Conflict of interest
This article represents multivariate analysis of the unpublished thesis for the fulfillment of the requirements of the main author’s Master of Public Health degree. The univariate and bivariate analysis can be found published as: Rocha-Buelvas A, Hidalgo A, Hidalgo-Eraso A. Determinantes de utilización de los servicios de la salud bucal en estudiantes universitarios del municipio de Pasto, 2011. Rev Fac Nac Salud Pública. 2013;31(3):359-71.
Financing
This research project was self-financed by the main author, was supported ad honorem by the co-authors in the statistical components, and was authorized by the Academic Direction of the Pasto campus of the Universidad Cooperativa to carry out information collection with its students in its classrooms.
Acknowledgments
The authors would like to thank the School of Public Health in the Faculty of Health at the Universidad del Valle for having supported and reviewed this research, a requirement for attaining the main author’s Master of Public Health degree. In addition, we thank tutor Andrés Alonso Agudelo, jury members Eliana Martínez and Edwin Meneses, and academic peers Carlos Augusto Hernández and Lyda Osorio.
References
1. Agudelo AA, Gómez J. Condiciones de salud bucal de los recuperadores informales del sector de Guayaquil y de sus familias. Medellín-Colombia, 2003. Revista Facultad de Odontología. 2004;15:12-20. [ Links ]
2. Rengifo HA, Corchuelo, J. Inequidades en la Atención Odontológica en una Red de Salud en Cali, Colombia. Rev Salud Pública. 2009;4:526-37. [ Links ]
3. Agudelo AA, Martínez E. La salud bucal colectiva y el contexto colombiano: un análisis crítico. Revista Gerencia y Políticas de Salud. 2009;8:91-105. [ Links ]
4. Agudelo AA, Isaza LT, Bustamante DA, Martínez CM, Martínez CM. Morbilidad bucal percibida y características sociales en la población desplazada y destechada de un asentamiento del municipio de Bello (Antioquia), 2005. Revista Facultad de Odontología. 2006;18:36-46. [ Links ]
5. Galvis LA, Meisel A. Convergencia y trampas espaciales de pobreza en Colombia: Evidencia reciente "Documentos de trabajo sobre Economía Regional". Cartagena: Centro de Estudios Económicos Regionales -CEER- Banco de la República; 2012. [ Links ]
6. Lang T, Kelly-Irving M, Delpierre C. Inequalities in health: from the epidemiologic model towards intervention. Pathways and accumulations along the life course. Rev Epidemiol Sante Publique. 2009;57:429-35. http://doi.org/cwfjc8. [ Links ]
7. Andersen R, Newman JF. Societal and individual determinants of medical care utilization in the United States. Milbank Mem Fund Q Health Soc. 1973;51:95-124. http://doi.org/fbgc4t. [ Links ]
8. Andersen RM, McCutcheon A, Aday LA, Chiu GY, Bell R. Exploring dimensions of access to medical care. Health Serv Res. 1983;18:49-74. [ Links ]
9. Kogevinas M, Pearce N, Susser M, Boffeta P. Social inequalities and cancer "Social inequalities and cancer". Lyon: IARC; 1997. [ Links ]
10. Watt G. The inverse care law today. Lancet. 2002;360:252-4. http://doi.org/b66ctp. [ Links ]
11. Frohlich KL, Potvin L. Transcending the known in public health practice: the inequality paradox: the population approach and vulnerable populations. Am J Public Health. 2008;98:216-21. http://doi.org/bxzf6b. [ Links ]
12. World Health Survey 2003 results. Geneva, World Health Organization [Internet]. 2007 [citado 2011 enero 6]. Disponible en: http://goo.gl/HIzBVw. [ Links ]
13. Chen M, Andersen RM, Barmes DE, Leclerq MH, Lyttle CS. Comparing oral health care systems: a second international collaborative study. Geneva: World Health Organization; 1997. [ Links ]
14. Andersen RM. Revisiting the behavioral model and access to medical care: Does it matter? J Health Soc Behav. 1995;36:1-10. http://doi.org/dhrntg. [ Links ]
15. Pizarro V, Ferrer M, Domingo-Salvany A, Benach J, Borrell C, Pont A, et al. The utilization of dental care services according to health insurance coverage in Catalonia (Spain). Community Dent Oral Epidemiol. 2009;37:78-84. http://doi.org/ftc8p6. [ Links ]
16. Feigelman S, Li X, Stanton B. Perceived risks and benefits of alcohol, cigarette and drug use among urban low-income African-American early adolescents. Bull N Y Acad Med. 1995;72:57-75. [ Links ]
17. Ajayi DM, Arigbede AO. Barriers to oral health care utilization in Ibadan, South West Nigeria. Afr Health Sci. 2012;12:507-13. [ Links ]
18. Marques-Santiago B, Gondim Valenca AM, Vianna Vettore M. Social capital and dental pain in Brazilian northeast: a multilevel cross-sectional study. BMC Oral Health. 2013;13:2. http://doi.org/zcn. [ Links ]
19. White DA, Tsakos G, Pitts NB, Fuller E, Douglas GVA, Murray JJ, Steele JG. Adult Dental Health Survey 2009: common oral health conditions and their impact on the population. Br Dent J. 2012;213: 567-72. http://doi.org/zcp. [ Links ]
20. Newsome PRH, Wright GH. A review of patient satisfaction: Concepts of satisfaction. Br Dent J. 1999;186:161-5. [ Links ]
21. Sun N, Burnside G, Harris R. Patient satisfaction with care by dental therapists. Br Dent J. 2010;208:E9. http://doi.org/dfcd2x. [ Links ]
22. Misrachi C, Espinoza I. Utilidad de las Mediciones de la Calidad de Vida Relacionada con la Salud. Revista Dental de Chile. 2005;96:28-35. [ Links ]
23. Dumitrescu AL, Kawamura M, Dogaru BC, Dogaru CD. Relation of achievement motives, satisfaction with life, happiness and oral health in Romanian university students. Oral Health Prev Dent. 2010;8:15-22. [ Links ]
24. República de Colombia, Ministerio de Salud. III Estudio Nacional de Salud Bucal y II Estudio de factores de riesgo de las enfermedades crónicas. Dirección General de Promoción y Prevención. Bogotá: Ministerio de Salud; 1999. [ Links ]
25. República de Colombia, Instituto Departamental de Salud de Nariño. Indicadores Básicos de Salud del Departamento de Nariño 2009. Subdirección de Salud Pública. Pasto: Instituto Departamental de Salud de Nariño; 2009. [ Links ]
