










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista de la Facultad de Medicina
versão impressa ISSN 0120-0011
rev.fac.med. vol.64 no.2 Bogotá abr./jun. 2016
https://doi.org/10.15446/revfacmed.v64n2.52409
DOI: http://dx.doi.org/10.15446/revfacmed.v64n2.52409
ORIGINAL RESEARCH
Coping and Quality of Life in Oncologic Patients of the Province of Nariño, Colombia
Afrontamiento y calidad de vida en pacientes oncológicos de Nariño, Colombia
Arsenio Hidalgo-Troya1, Amanda Pantoja-Córdoba2, Pamela Sañudo-Vélez2, Anderson Rocha-Buelvas3
1 Universidad de Nariño – Faculty of Exact and Natural Sciences – Department of de Mathematics and Statistics - Pasto - Colombia.
2 Universidad de Nariño – Faculty of Human Sciences - Department of Psychology - Pasto - Colombia.
3 Fundación Universitaria del Área Andina – Bogota Campus – Faculty of Health Sciences – Master's degree program in Public Health and Social Development - Bogota, D.C. - Colombia.
Corresponding author: Arsenio Hidalgo-Trojan. Department of Mathematics and Statistics, Faculty of Natural Sciences, Universidad de Nariño. Ciudadela Universitaria Torobajo, Calle 18 Carrera 50. Phone: +57 2 7310327. Pasto. Colombia. E-mail: arsenio.hidalgo@gmail.com.
Received: 09/08/2015 Accepted: 23/10/2015
Abstract
Introduction. Coping, regarded as the set of responses to stressful situations, executed to handle and neutralize them, is part of the psychological resources of human beings and it is a personal trait evidenced as intervening in terms of perceived quality of life.
Objective. To determine the relationship between coping strategies and quality of life in cancer patients at different stages of their cancer condition at an oncology unit in the province of Nariño, Colombia.
Materials and Methods. Cross-sectional study in a sample of 120 cancer patients attending in COEMSSANAR IPS, located in Pasto, Nariño.
Results. It was observed that the most adopted type of coping was "positive attitude", followed by "positive guidance", while the least adopted ones were "anxious care" and "hopeless". As for quality of life, it is evidenced that is favorable for this population. The relationship between coping and quality of life is different for each stage of cancer. Patients with better coping are those with higher quality of life.
Conclusion. A greater effort of the State and the institutions providing health services for the adoption of coping strategies in patients affected by cancer at all stages would significantly improve the quality of life of these people.
Keywords: Adaptation, Psychological; Quality of Life; Oncology Service, Hospital; Neoplasm Staging; Multivariate Analysis; Colombia (MeSH).
Hidalgo-Troya A, Pantoja Córdoba A, Sañudo-Vélez P, Rocha-Buelvas A. Coping and Quality of Life in Oncologic Patients of the Province of Nariño, Colombia. Rev. Fac. Med. 2016;64(2):181-8. English. doi: http://dx.doi.org/10.15446/revfacmed.v64n2.52409.
Resumen
Introducción. El afrontamiento, entendido como el conjunto de respuestas ejecutadas para mantener y neutralizar situaciones estresantes, es parte de los recursos psicológicos del individuo y es una de las variables personales evidenciadas como intervinientes en los niveles de calidad de vida percibida.
Objetivo. Determinar la relación existente entre las estrategias de afrontamiento y la calidad de vida de pacientes oncológicos en diferentes estadios del cáncer en una unidad de oncológica de Nariño, Colombia.
Materiales y métodos. Estudio descriptivo transversal realizado en una muestra de 120 pacientes oncológicos de Cooemssanar IPS en su sede de Pasto.
Resultados. Se observó que el tipo de afrontamiento más adoptado fue "actitud positiva", seguido de "orientación positiva", y los menos adoptados fueron "preocupación ansiosa" y "sin esperanza". En cuanto a la calidad de vida, se evidencia que es favorable para la población estudiada, aunque la relación entre el afrontamiento y esta es diferente para cada estadio del cáncer. Los pacientes con mejor afrontamiento son los que tienen mayor calidad de vida.
Conclusión. Un mayor esfuerzo del Estado y de las instituciones prestadoras de servicios de salud para la adopción de estrategias de afrontamiento en los pacientes afectados por el cáncer, en todos sus estadios, mejoraría notablemente la calidad de vida de estas personas.
Palabras clave: Adaptación psicológica; Calidad de vida; Servicio de oncología en hospital; Estadificación de Neoplasias; Análisis Multivariante; Colombia (DeCS).
Hidalgo-Tovar A, Pantoja Córdoba A, Sañudo-Vélez P, Rocha-Buelvas A. [Afrontamiento y calidad de vida en pacientes oncológicos de Nariño, Colombia.] Rev. Fac. Med. 2016;64(2):181-8. English. doi: http://dx.doi.org/10.15446/revfacmed.v64n2.52409.
Introduction
In 2012, 14.1 million new cancer cases occurred worldwide, out of which 8.2 million ended in deaths, out of which 30% could have been avoided. It is estimated that this public health issue will increase to 12 million cases by 2030 (1). Cancer is the third leading cause of death in Colombia; the five most common types of cancer are prostatic, breast, cervical, colorectal and stomach (2). In Nariño, Colombia, the burden of noncommunicable diseases is increasing (3) and the burden related to cancer highlights a large sum of years lost due to premature death (DALY) particularly in women. In the central region, where the city of Pasto is located —the greatest receiver of cases in the department— tumors with more than 50% of years lost due to premature death (DALY) in men correspond to stomach, leukemia, prostate, colon and rectum, while women's tumors are related to the sexual and reproductive organs, stomach and breast (4).
Beyond these figures, it is worth mentioning that the difficulties and psychological distress in cancer patients is manifested by emotional reactions that prevent them from seeking treatment, cooperating or interfering with it, which in turn causes more pain and discomfort, emotional responses manifested as psychiatric symptoms, and emotional reactions that disrupt daily, individual and social activities (5).
In Colombia, the prevalence of psychiatric disorders in chronic diseases, such as cancer, is one of the highest: 6% to 38% corresponds to depression and 20.5% corresponds to anxiety (6), so that coping becomes a very important aspect as a part of the psychological resources of the individual, and is one of the personal variables that intervenes in the levels of the perceived quality of life. Quality of life is understood as the activities that are valued per se and in the ability to accomplish them, since life is perceived as a set of doings and beings —achievements— valued by the individual (7,8).
Thus, Barez-Villoria (9), based on Moorey and Greer, states that the existence of a scheme of survival or cognitive triad in patients with cancer —comprising the diagnosis, the perceived control and the prognosis— determines various types of coping. These coping strategies aim at anxious concerns related to depression and anxiety, fatalism and helplessness/hopelessness related to depression, and the fighting spirit (the one with better adaptation), which can determine the psychological morbidity of cancer patients.
In the population of developing countries, it has been found that avoidance and deterioration strategies are correlated with the dimensions of life quality; therefore, it is important to measure the relationship between coping variables and quality of life for the issue of cancer in different contexts (10).
Materials and methods
A cross-sectional descriptive study was conducted with a population of 477 people, using a simple random probability sample, a margin of error of 7.7% and a confidence level of 95%. The sample size was 120 cancer patients (97 women and 23 men) ranging between the ages of 22 and 80. The selection criteria were: being diagnosed, being patients of the oncology unit of the service provider institution Cooemsanar IPS located in Pasto between the months of June and July 2010, and having accepted the disease.
To develop the study, two measurement tools validated in Colombia were used:
Mental Adjustment to Cancer (MAC) scale (11), whose purpose is assessing specific coping responses in any adult cancer patient and consists of 27 items and 4 dimensions: positive attitude, positive orientation, anxious and hopeless concern; the responses were quantified using a four point Likert scale.
Questionnaire of quality of life related to health (SF-36) (12), which is a generic scale that provides a profile of the health status and allows assessing the quality of life related to health in specific subgroups, comparing the burden of various diseases, detecting positive and negative health states, recognizing the benefits produced by different treatments and exploring the physical and mental health focusing on functional status and emotional well-being. This questionnaire consists of 36 items and 8 dimensions: physical function, physical role, bodily pain, general health, vitality, social function, emotional role and mental health; the responses were quantified using a Likert scale of five ordinal responses. The Cronbach's Alpha Reliability Coefficient was 0.7, while the pooled estimates obtained by meta-analysis were >0.7.
An univariate analysis was performed to characterize the behavior of the different dimensions of the quality of life and coping variables and to establish their correlation with the canonical form which identifies the dimensionality of each set of variables, maximizing the relationship between the two sets through canonical functions that allow the theoretical construct of variable pairs —linear combinations— based on the original variables. This canonical analysis was generally performed by stratifying the different stages of the cancer disease in groups: group one, patients in stage I and II; group two, patients in stage III and IV, and group three, patients already treated and attending follow-up sessions.
The validity of the relationship between pairs of theoretical values is reflected through canonical correlation; this value, when squared, represents the amount of variance of a theoretical value explained by the other theoretical value, that is, the amount of shared variance between these values —canonical R2 or canonical root. The canonical functions with statistically significant correlation coefficients (p≤0.05) and with appropriate magnitudes of canonical correlations and redundancy measures for the variance percentage explained by the pair of data sets are analyzed. The interpretation of the pair of theoretical values generated by the valid canonical function is performed through weighting the canonical functions selected for analysis.
Results
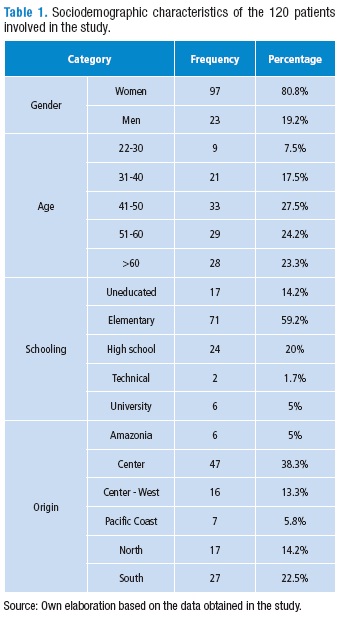
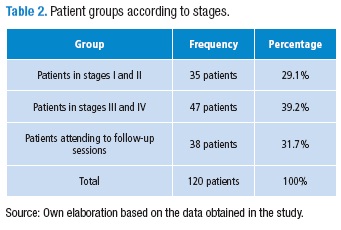
It was found that 80.2% of patients were female and the average age was 50.6, with a value of standard deviation of 13.6 years and a variation range of 22 to 80 years. In relation to schooling, 59.2% of patients had elementary education, 20% high school education, 5% higher education and 14.2% were illiterate. Most patients (38.3%) came from the central area of the department, 22.5% from the south and 14.2% from the north (Table 1) and 28.3% were diagnosed with breast cancer, followed by cervical cancer with 25% and ovarian cancer with 8.3%. The stages were distributed similarly in all patients (Table 2).
Within these patients, 91.7% responded to the oncological disease with the "positive attitude" type of coping, which indicates that most patients took up an active coping response, accepting the diagnosis and adopting an optimistic attitude. Regarding positive orientation, 51.7% of patients tended to be located in this type of coping (Table 3).
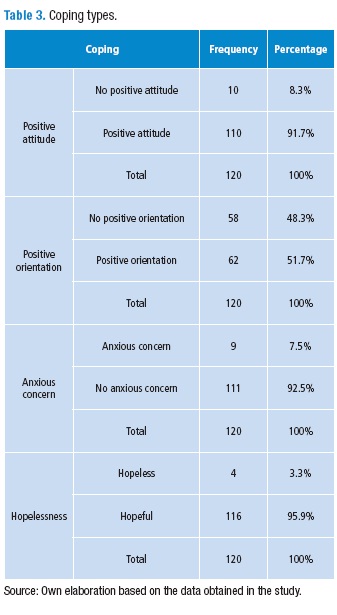
92.5% of patients presented the "no anxious concern" type of coping, while 95.9% was located in "hopeful", confirming that most of them adopted an adequate coping type regarding the disease. Those who adopted the wrong type of coping (8.3% "not positive attitude", 7.5% "anxious concern" and 3.3% "hopeless") were included in "without positive orientation".
Regarding quality of life (Table 4), it was found that the "physical function" and the "social function" have similar behavior with higher average scores of 81.3 and 81.0 respectively, with low standard deviations that indicate homogeneity in the scores. This proves that physical activities such as self-care, walking, climbing stairs, bending and making moderate and intense efforts have not been affected, just as the social function has not been significantly reduced.
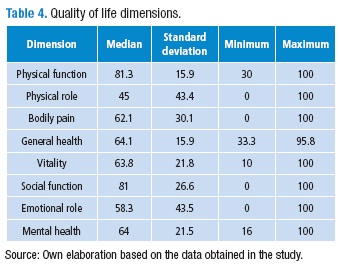
"General health", "mental health" and "vitality" dimensions show similarities, presenting high mean scores of 64.1, 64 and 64.8, respectively, with low standard deviations that indicate homogeneity in the scores. This shows that the dimensions "general health", which evaluates personal health assessment, and "mental health", which is related to depression, anxiety, behavioral control or general welfare, can be placed in the variable "vitality" that involves feelings of energy and dynamism against the feeling of tiredness and exhaustion related to the disease.
The mean scores of the dimensions "physical role", "emotional role" and "bodily pain" are low considering that their standard deviations are large; therefore, the scores are scattered and occur heterogeneously. This shows that physical health interfered and hindered the performance of everyday activities. It was also found that the intensity of pain and its effect on the regular work, as well as the degree of interference of emotional problems in their daily activities is considerable.
The results of segments A to D shown in Table 5 indicate the existence of a linear correlation between the sets of the variables quality of life and coping observed in the general population, the population of patients in stages I-II and the treated population in follow-up sessions, but not in the population in stages III and IV, taking into account the statistical significances of canonical correlations and the magnitudes of canonical correlations and redundancy measures in this type of functions.
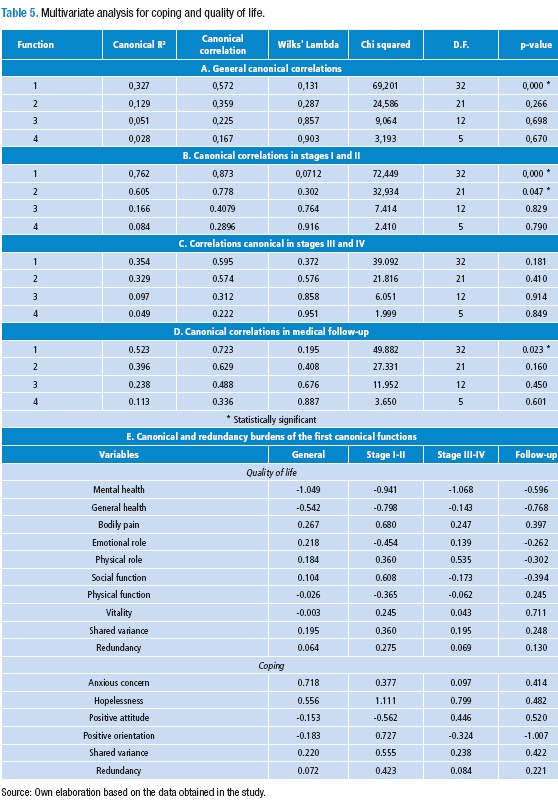
Statistical significance was found in the general population in the first canonical function (canonical correlation 0.572 and redundancy measure 0.064) showing, due to their canonical weights, that the components in quality of life with greater impact on the correlation were "mental health" and "general health" and on coping "anxious concern" and "hopeless" (Table 5, segment E).
In the population of patients in stages I-II, statistical significance in the first and second canonical function was found, with better results in the first function (canonical correlation of 0.873 and redundancy measure of 0.423), noting that the components in quality of life with higher incidence in the correlation were "mental health" and "general health" and in coping "hopeless" and "positive orientation". No linear correlation between quality of life and coping in patients in stages III-IV was found, while linear correlation between patients who were treated and attended follow-up sessions, with statistical significance in the first canonical function (canonical correlation of 0.723 and redundancy measure of 0.221) was observed, showing that the components in quality of life with greater contribution to the correlation were "general health" and "vitality" and to coping were "positive orientation" and "positive attitude".
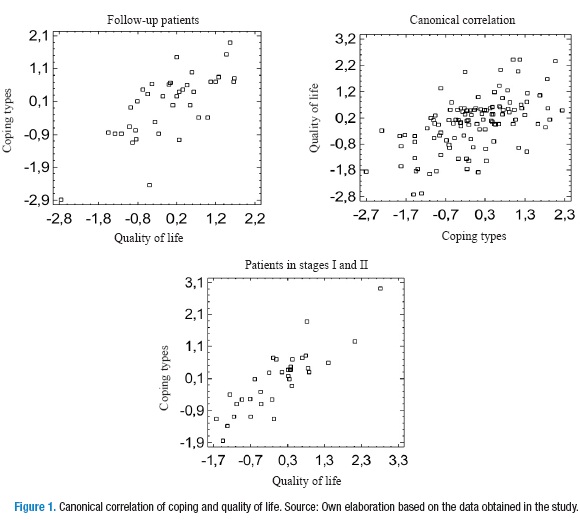
Finally, it was shown that the relationship between types of coping and quality of life is direct, that is, the higher the coping, the better the quality of life because, in each of the series, coefficients have significant positive burdens and, therefore, the index resulting for each instrument includes a considerable number of canonical variables (Figure 1).
Discussion
According to Arraras et al. (10), since the decade of 1990, the interest for properly assessing the impact of the disease and treatments on the quality of life has increased (13). Currently, interest in the correlation of these variables in the hospital environment aims at obtaining a comprehensive view, where treatment not only emphasizes on the physiological symptoms but also on the psychological aspects of the disease, since the best way to mitigate its impact is adopting the appropriate coping strategies that positively affect the quality of life, restoring mental health and well-being of these patients.
Contradictorily, there is evidence that, in cancer patients, the functional dimensions and symptoms of the disease show favorable conditions with clinically significant levels of anxiety-depression (14). Also, many studies that have measured the quality of life in patients with a definitive diagnosis of cancer show deterioration, during and after treatment, of the functional and financial aspects (15), while other studies attribute to spirituality or religiosity the improvement of the quality of life of patients undergoing palliative care in the treatment of tumors in advanced stages (16).
A study in the Netherlands showed, regarding the results of this study, that coping strategies are related to quality of life, depression and despair, therefore, interventions of the cognitive behavioral type are considered useful in healing and palliative patients (17), which makes important the use of a conceptual model such as quality of life related to health, that empirically assesses the scientific design of interventions in order to promote psychosocial well-being and coping strategies (18). The results of this study and the findings presented here, like many others, indicate that cognitive assessment —through which the cancer patient attributes a meaning to the diagnosis of the disease in terms of a challenge, a threat, damage or loss, or absence of threat— will define the type of coping that the patient will adopt to deal with the disease.
During the univariate analysis, it was found that a large percentage of patients are located in the "positive attitude" type of adaptive coping and a significant percentage is also located in "positive orientation", which indicates that the decision-making and implementation of actions aimed to preserve health and fight the oncological disease are present. For these reasons, coping with cancer cannot be characterized by one coping strategy, but it may be changed over the disease process. Similarly, a person may be using different coping strategies simultaneously.
The "fighting spirit" was present in 63% of the patients, which is equivalent to two types of coping: "positive attitude" and "positive orientation", which coincides with other findings in chronic patients (12) who report a tendency to assume adaptive coping types such as "targeting the problem" and "positive reassessment". Also, the "hopelessness" and "anxious concern" types of coping, or the least adopted by the subjects of this study, indicate that they lack strategies for coping with and controlling the disease and that they have a perception of threat, which coincides with the Barez- Villoria et al. study (9), where "hopeless" coping is adopted by a minority.
The dimensions of quality of life "physical function" and "social function", as prevalent, are the result that resembles the research of Contreras (12), where patients do not realize that their physical or emotional health conditions significantly interfere with their social life. Dimensions "mental health," "general health" and "vitality", presented at a medium level and that allow stating that these are not significantly affected, agree with the findings of Montes et al. (19), who claim that treatments for cancer disease have implications in the short and long term on the well-being of a patient; however, the positive assessment of health of the study subjects shows that the prospects of current and future health are manifested through feelings of energy and vitality.
The dimensions "physical role" and "emotional role" are the least prevalent, demonstrating that there is interference of physical health during work or other daily activities; this is added to the interference of emotional problems related to the impact and adjustment to the disease in the daily activities of patients. The dimension "bodily pain" is also affected, indicating that the pain caused by the cancer disease has an impact on daily tasks.
The multivariate analysis arises from the need to examine the relationships that exist between coping strategies and other variables such as quality of life or anxiety and depression; according to the study of Portillo-Guerra & Restrepo (20), this proposal is consistent with the findings in the analysis of this study, where a direct linear relationship between quality of life and coping, established by the statistically significant correlation coefficient with a confidence level of 99.9%, was observed, which allows stating that the better the coping, the higher the quality of life or vice versa.
As in this study, the research of Rodríguez-Quintana et al. (21) reports that the analysis of association between quality of life and coping depends on the stage of cancer; for example, it was observed that for groups of patients in stages I-II and follow-up —already treated— there was a significant correlation coefficient, while in the group of patients in stages III-IV, there was none. The study variables behaved independently.
This study is consistent with current research interest on psychology, since new methodologies were used to expand knowledge about the psychological impact of oncologic disease by providing information on the psychological resources these patients have to cope with the disease; this, undoubtedly, is of great importance to strengthen the theoretical proposals in the fields of health psychology and psycho-oncology. A greater emphasis on patients in stages III and IV in new studies is also considered as necessary because one of the limitations of this research was not having a more homogeneous population in terms of gender and amount of patients for each stage.
Conflicts of interest
None stated by the authors.
Funding
No external or institutional funding was stated by the authors.
Acknowledgement
Psychology Program of Universidad de Nariño.
References
1. Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C, et al. Cancer Incidence and Mortality Worldwide: IARC Cancer Base. GLOBOCAN 2012. 2013;10(11). [ Links ]
2. Piñeros-Petersen M, Pardo-Ramos C, Gamboa-Garay Ó, Hernández-Suárez G. Atlas de mortalidad por cáncer en Colombia. Bogotá, D.C.: Instituto Nacional de Cancerología, Ministerio Protección Social, Instituto Geográfico Agustín Codazzi; 2010. [ Links ]
3. Rocha-Buelvas A, Trujillo-Montalvo E, Hidalgo-Patiño C, Hidalgo-Eraso A. Burden of disease in Nariño, Colombia, 2010. Colomb. Med. 2014;45(28):96-103. [ Links ]
4. Rocha-Buelvas A, Trujillo-Montalvo E, Hidalgo-Patiño C, Hidalgo-Eraso A. Carga de cáncer del departamento de Nariño y subregiones, Colombia, 2010. Rev. Fac. Nac. Salud Pública. 2014;32(3):340-54. [ Links ]
5. Sanz J, Modolell E. Oncología y psicología: un modelo de interacción. Psicooncología. 2004;1(1):3-12. [ Links ]
6. Ministerio de Salud y Protección Social, Colciencias. Encuesta Nacional de Salud Mental 2015. Tomo I. 2015. Bogotá, D.C.: Minsalud; 2015. [ Links ]
7. Sen A. El desarrollo como libertad. Buenos Aires: Editorial Planeta; 2000. [ Links ]
8. Sánchez-Pedraza R, Ballesteros MP, Anzola JD. Concepto de calidad de vida en mujeres con cáncer. Rev. Salud Pública. 2010;12(6):889-902. [ Links ]
9. Bárez-Villoria M. Relación entre percepción de control y adaptación a la enfermedad en pacientes con cáncer de mama. [Tesis Doctoral]. Barcelona: Universitat Autònoma de Barcelona; 2002. [ Links ]
10. Llull DM, Zanier J, García F. Afrontamiento y calidad de vida. Un estudio de pacientes con cáncer. Psico-USF. 2003;8(2):175-82. [ Links ]
11. Forero-Carreño F, Bernal-Rojas G, Restrepo-Forero M. Propiedades psicométricas de la escala de ajuste mental al cáncer (MAC) en una muestra de pacientes colombianos. Avances en Medición. 2005;3:135-52. [ Links ]
12. Contreras F, Esguerra G, Espinosa JC, Gómez V. Estilos de afrontamiento y calidad de vida en pacientes con insuficiencia renal crónica (IRC) en tratamiento de hemodiálisis. Act. Colomb. Psicol. 2007;10(2):169-79. [ Links ]
13. Arraras JI, Martínez M, Manterota A, Laínez N. La evaluación de la calidad de vida del paciente oncológico. El grupo de calidad de vida de la EORTC. Psicooncología. 2004;1(1):87-98. [ Links ]
14. Gaviria AM, Vinaccia S, Riveros MF, Quiceno JM. Calidad de vida relacionada con la salud, afrontamiento del estrés y emociones negativas en pacientes con cáncer en tratamiento quimioterapéutico. Psicol. desde el Caribe. 2007;20:50-75. [ Links ]
15. Rohani C, Abedi HA, Omranipour R, Langius-Eklöf A. Health-related quality of life and the predictive role of sense of coherence, spirituality and religious coping in a sample of Iranian women with breast cancer: a prospective study with comparative design. Health Qual. Life Outcomes. 2015;13(1):1-14. http://doi.org/bdhd. [ Links ]
16. Vallurupalli M, Lauderdale K, Balboni MJ, Phelps AC, Block SD, Ng AK, et al. The role of spirituality and religious coping in the quality of life of patients with advanced cancer receiving palliative radiation therapy. J. Support. Oncol. 2012;10(2):81-7. http://doi.org/c2sm8j. [ Links ]
17. van Laarhoven HW, Schilderman J, Bleijenberg G, Donders R, Vissers KC, Verhagen CA, et al. Coping, quality of life, depression, and hopelessness in cancer patients in a curative and palliative, end-of-life care setting. Cancer Nurs. 2011;34(4):302-14. http://doi.org/d8f4gv. [ Links ]
18. Schwartzmann L. Calidad de vida relacionada con la salud: aspectos conceptuales. Cienc. Enferm. 2003;9(2):9-21. http://doi.org/fqbhf7. [ Links ]
19. Montes L LM, Mullins P MJ, Urrutia S MT. Calidad de vida en mujeres con cáncer cérvico uterino. Rev. Chil. Obstet. Ginecol. 2006;71(2):129-34. http://doi.org/c6sq8q. [ Links ]
20. Portillo-Guerra C, Restrepo M. Evaluación del cuestionario de calidad de vida EORTC QLQ C-30 dentro de un estudio con pacientes adultos de centros de oncología de Bogotá. Avances en Medición. 2004;2:51-61. [ Links ]
21. Rodríguez-Quintana R, Hernando-Trancho F, Cruzado JA, Olivares ME, Jamal I, Laserna P. Evaluación de la calidad de vida, estado emocional y estrategias de afrontamiento en pacientes con enfermedad neoplásica pulmonar. Psicooncología. 2012;9(1):95-112. [ Links ]

