











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Chronic lung diseases are common and their exacerbations are the main cause of consultation in the emergency department since they impair the quality of life of patients 1-3. In chronic obstructive pulmonary diseases, exacerbations account for 25% of the causes of dyspnea in the emergency room and represent 500 000 to 726 000 hospitalizations annually in the United States, generating 25-30% of the costs related to this pathology 1,2,4.
Different variables have been decisive for the prognosis of exacerbations; however, despite the pathophysiological correlation between chronic lung diseases with hypoxemia and erythrocytosis development, red blood cell parameters have not been evaluated as predictors of these events 2,5.
Erythrocytosis could affect the prognosis of an exacerbation by altering the microvascular rheology of patients and decreasing tissue perfusion and cardiac output 6,7. In long-term observations, anemia has been identified as a factor involved in the development of adverse events in patients with stable chronic lung disease, whereas erythrocytosis has shown its inference on a better prognosis 8-11.
Determining the virtual implications of red cell parameters in patients with pulmonary exacerbations could help defining the particular use of measures such as phlebotomy or red blood cell transfusion.
Currently, phlebotomy remains a measure of regular use in clinical practice, as it is economical and easy to perform; nonetheless, specifications around its technique are variable in studies and in usual clinical practice 7,12. There are limited data on its usefulness, as there are no works on proper methodology to evaluate its effectiveness 13-17. Therefore, there is a big gap in the state of the art, which indicates the need to expand clinical research to achieve a better characterization of the risk and the need for treatment of secondary erythrocytosis in stable and exacerbated chronic lung disease.
This study aimed to determine whether there is a relationship between the red cell prognostic parameters and adverse outcomes at 30 days in patients admitted under the diagnostic impression of an exacerbated chronic lung disease and secondary hypoxemia.
Materials and methods
Study design
An observational study of a single prospective cohort was performed considering the patients admitted to Fundación Hospital San Carlos between March 2011 and October 2011 with a diagnostic impression of exacerbated chronic lung disease and secondary hypoxemia, as unit of analysis.
The selection of the cohort was done in order to determine prognostic factors (at 30 days of admission) related to hospital stay, need for mechanical ventilation, need for transfer to intensive care unit (ICU), rehospitalization and death. Demographic, clinical and paraclinical variables supported in the literature were included.
Patients
Patients over 18 years of age, with a history of chronic lung disease, hypoxemia at admission and diagnostic impression of exacerbation of, infectious or non-infectious, chronic lung disease were selected. Patients were required to have lived in Bogotá at least in the last six months to avoid variations in erythrocyte indices.
The following operating variables were established as admission and results analysis criteria:
The term chronic lung disease referred to chronic obstructive pulmonary disease, diffuse interstitial lung disease, asthma or obstructive sleep apnea/hypopnea syndrome of more than three months of evolution, established by any of the following events: specific reference of the diagnosis by the patient or relative, diagnostic documentation prior to evaluation by a pulmonologist or internist, abnormal lung function tests compatible with the diagnosis of the disease, or daily use of inhalers or theophylline for more than three months.
Anemia was defined as hemoglobin values below 13 g/dL in men and 12 g/dL in women, according to normality data recorded for Bogotá and Quito 18,19.
Erythrocytosis was established based on hematocrit values higher than 50% in women and 55% in men 18,19.
Patients with congenital heart disease, for whom diagnosis of exacerbation of lung disease was discarded at discharge, and those who did not wish to participate in the study were excluded from the study.
To define the entry of each individual to the study, the patient or caregiver was asked to sign an informed consent during the initial interview for authorization to collect data, accessing medical records, follow-up at 30 days and processing the information obtained.
Study assessments
After checking the study entry criteria and obtaining the authorization of the patients or caregiver for inclusion, we proceeded to collect information through a survey to patients during their hospital stay. Demographic and clinical data were obtained directly from patients or their relatives, and were verified using the medical records, from where information about paraclinical was also extracted. In the event that the patient underwent phlebotomy, blood count values at admission and the last blood count obtained after the last blood collection were taken for comparison.
The survey was completed by telephone at 30 days after admission to hospital in order to assess the outcome. Data were collected and tabulated in Microsoft Access 2010 and SPSS v19 was used for conducting statistical analysis. These information handling procedures were verified, each and in full, ensuring that no inconsistencies or missing data were found. At each step, the fulfillment of the criteria for inclusion and exclusion was verified.
Outcome measures
The outcome variable was a composite between death, length of hospital stay in floors, need for invasive or non-invasive ventilatory support, need to transfer to ICU and rehospitalization, provided that they were associated with chronic lung disease. The evaluation began the day of admission of the patient to the institution until day 30 of follow-up.
Statistical analysis
Knowing, based on the studies published in the literature, that patients with chronic lung diseases have an 11% rate of mortality, 11.6% probability of readmission, 25% probability of admission to ICU, and 3% probability of requiring mechanical ventilation due to exacerbation, the risk of a combined outcome for the study was defined in at least 25%.
Guided by the value of prognostic factors evaluated during exacerbations, it is assumed that the presence of erythrocytosis may increase or decrease the risk twice for the combined outcome.
A sample of 122 subjects was estimated at two tails in Stata 9.1, finding an expected risk difference of 25% and a power of 80%, assuming an error α of 5%.
In order to determine the normality assumption, the Kolmogorov-Smirnov test was performed for univariate analysis of quantitative variables. Depending on the outcome, the abnormally distributed variables were reported by their median and interquartile range, while those presenting normal distribution were reported by their mean and standard deviation. The qualitative variables were reported as absolute and relative frequencies.
In addition, the distribution of variables was stratified by sex and hematocrit value, which was categorized into three groups according to the 25th and 75th percentiles of the distribution.
For bivariate analysis, the Mann-Whitney U test was performed. It differentiates the medians of independent samples in the analysis of quantitative variables that do not follow a normal distribution with the dependent variable. To establish the association between the independent qualitative variables and the dependent or outcome variable, the Chi square test of independence (X2) was used along with the Mantel-Haenszel method. If the expected frequencies were less than five cases, the Fisher's exact test was used. The odds ratio (OR) and confidence intervals were calculated through StatCal in EpiInfo 3.5.1.
To perform a multivariate analysis using the logistic regression method, those statistically significant variables associated with the outcome (p≤0.25) were selected, and the Hosmer and Lemeshow test was used as calibration criterion.
Results
Between March and October 2011, a cohort of 128 patients was selected, out of which 110 met the inclusion and follow-up criteria proposed for the study. The collection of the sample was interrupted between June and August 2011 due to issues in the attention of users in the institution, which affected the admission of patients.
The cohort was composed by subjects with a minimum age of 43 and a maximum age of 90, for a median of 73.5 years; the interquartile range was 62.5 to 84.5 years of age. 56.2% of the participants were female and the female: male: ratio was 5:4 (Table 1).
Table 1 Demographic, clinical and paraclinical characteristics of patients included in the study.
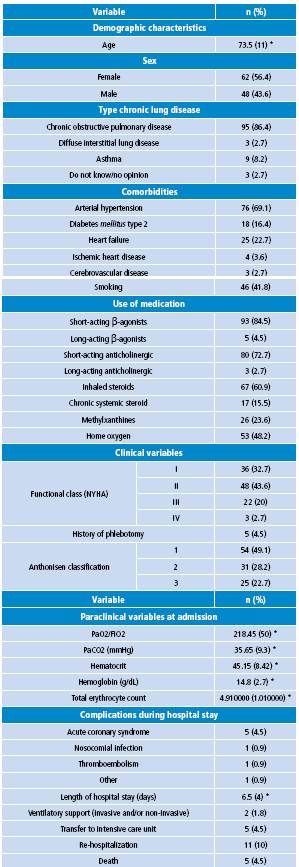
* Median (interquartile range). Source: Own elaboration based on the data obtained in the study.
The diagnosis of chronic lung disease was the most common chronic obstructive pulmonary disease (86.4% of the cohort) followed by asthma and interstitial lung disease. Asthma cases had an exclusive distribution in women. Overall, 3 out of 4 patients had NYHA functional class I or II, being the functional class IV the most uncommon.
The most frequently used medications were short-acting bronchodilators, and their combination was the most common association, followed by association with inhaled steroids. While the minority of patients had a severe functional class (IV), the use of long-acting bronchodilators was limited to only five cases, compared with the more extensive use of methylxanthines. There was no difference between sexes regarding the type of prescription medications. 48% of patients used home oxygen at the time of the study; indications for initiation and permanence with this treatment were not evaluated.
The presence of comorbidity was high, especially in women; among them, hypertension was the most prevalent comorbidity, followed by heart failure and diabetes mellitus type 2. Almost half of patients had a history of smoking and it was two times higher in men compared to women.
Regarding the severity of the exacerbation, all patients presented hypoxemia at admission, and the central tendency was no hypercapnia in accordance with the values of pCO2 accepted as normal for Bogotá. After assessment of the severity using Anthonisen criteria, 54% were classified in type 1.
During hospital stay, eight cases presented complications, four of them showed one of the outcomes assessed at 30 days, and only one included death. The most common outcome was rehospitalization, which occurred in 10% of the cohort; this coincides with data reported in the literature.
Erythrocyte parameters showed an overall predilection of being within normal values, with a median of 45.15% and an interquartile range of 8.42% for hematocrit. The frequency of anemia was 7.3%, while the presence of erythrocytosis was identified in 14.5% of the population, with a similar distribution between the sexes.
When assessing the data by dividing the sex distribution and the hematocrit levels in the 25th and 75th percentiles (Table 2) in order to debug the virtual relationships of the different levels of red cell parameters with the characteristics of the cohort, no relationship between hematocrit values and NYHA functional class of patients, nor between severity of exacerbation according to the criteria of Anthonisen was evident. Nevertheless, there was a tendency to lower PaO2/FiO2 and higher pCO2 in the presence of higher levels of hematocrit at admission.
Table 2 Clinical and paraclinical characteristics of patients included in the study by sex and hematocrit levels in percentiles.
* Median (interquartile range)
† Mean (standard deviations)
Source: Own elaboration based on the data obtained in the study.
No relationship between a history of use of home oxygen and hematocrit values was found.
At admission, five patients had a history of phlebotomy and hematocrits were located preferentially in the last interquartile or near this range. In only one case phlebotomy was repeated.
Regarding the outcomes, there was a predilection to higher length hospital stay in the presence of lower levels of hematocrit. Other outcomes did not appear to have any relation to hematocrit levels, although no deaths were recorded in the group of patients with the highest levels of hematocrit.
The variables in the bivariate analysis that were statistically significant to be included in the multivariate analysis were age, history of hypertension, history of heart failure, use of short-acting anticholinergics, home oxygen, type of Anthonisen and hematocrits at admission, being blood pressure the factor with the greatest weight (Table 3).
Table 3 Bivariate analysis of prognostic factors for the composite outcome.
NA: Not applicable.
* X2 Mantel-Haenszel method
† Mann Whitney U test
‡ Fisher.
Source: Own elaboration based on the data obtained in the study.
Regarding red blood cell parameters, a tendency to have a protective effect when located in the core values of hematocrit against extreme values, this difference did not show a statistical significance.
The multivariate analysis found an association with the development of the composite outcome in the Anthonisen classification, paradoxically, being the association with type 2 (OR=10.45, 95%CI: 1.11-98.48; p=0.04) higher when compared with other types. Hypertension continued to be the factor with the strongest association (OR=11.02, 95%CI: 1.32-91.75; p=0.026) and a history of heart failure acted as a protective factor (OR=0.09, 95%CI: 0.01-0.82; p=0.032) in an unexpected and difficult to understand association from the clinical and pathophysiological point of view (Table 4).
Table 4 Multivariate analysis of prognostic factors for the composite outcome.
Hosmer and Lemeshow test: 0.948.
Source: Own elaboration based on the data obtained in the study.
Only three of the patients underwent phlebotomy, and its indication included the hematocrit value in all cases, regardless of the clinical presentation. Blood volumes extracted and the number of sessions were variable in each of the procedures and did not correlate with the magnitude of change in the red blood cell values in the subsequent blood count control (Table 5). None of these patients presented any of the outcomes assessed at 30 days.
Discussion
This study attempted to establish the relationship between red blood cell parameters and the development of adverse outcomes at 30 days in patients with exacerbated chronic lung disease. The results showed that exacerbations of chronic lung diseases afflicted, with very little difference in frequency, both men and women and appeared at similar ages, without any difference in the severity of the disease, although comorbidities are more often associated with women. In Colombia, short-acting bronchodilator and inhaled steroids remain the mainstay of treatment; although, despite guideline recommendations for management of chronic obstructive pulmonary diseases, only a few cases of patients receive long-acting bronchodilator 20.
Of the outcomes assessed in this cohort at 30 days, mortality, the need for ventilatory support and transfer to ICU presented in a very low proportion to the expected compared to previously reported data; the only outcome that showed a similar frequency to that reported in the literature was rehospitalization in 10% of cases 5,21,22. Erythrocytosis frequency was 14.5%, being higher than that reported in other cohorts 8-10.
There are several observations that have found a worse prognosis of mortality and need for hospitalization in patients with lower red cell mass compared to those with higher values 9,10,12. The prognostic value of this variable in the exacerbation has not been evaluated to date.
Since the NYHA functional class and the use of medications did not differ due to hematocrit levels, erythrocyte parameters in this cohort did not appear to have any relation to the severity of chronic lung disease in patients. On the other hand, the presence of the exacerbation did not differ according to the Anthonisen criteria, but did show a trend to greater affectation of oxygenation and hypercapnia in the presence of higher hematocrit levels. Adverse outcomes were more likely to occur at the extremes of the distribution of hematocrit values, also with longer hospital stay when hematocrit values were lower.
The multivariate analysis did not include erythrocyte parameters given the lack of statistical significance of the data provided by these variables with the outcome.
The variables that were statistically significant showed some unusual associations, particularly with the Anthonisen classification and the presence of a history of heart failure, the latter being a protective factor, without defining a coherent explanation for this finding and without any publication report with a similar result that could be used to infer that protective effect. By contrast, other prognostic factors found to be related with exacerbations in other studies, such as age, use of home oxygen, the presence of signs of respiratory distress at admission, the number of Anthonisen criteria present and blood gases, could not be validated in this cohort 2,5,22,23,24.
Phlebotomy was performed in only three patients; indications focused on the hematocrit value and the technique used was variable in each case without having a direct relationship between the volume of blood extracted and the change of red cell values, in fact, in one patient no changes were seen. These data, although scarce, revalidated the limitation on the approach to a patient with erythrocytosis in the emergency room, as well as the absence of protocols that clarify the possible indications and phlebotomy techniques.
The negative result of this study, regarding the influence of erythrocyte parameters in the prediction of exacerbations in chronic lung disease, may be caused by the statistical limitations of the study because the projected calculation of the sample was not obtained due to the difficulties for collecting data during the months in which the Fundación Hospital San Carlos was not fully functioning.
Also, fewer events than expected for the composite outcome presented, which could be explained by the fact that some of the included subjects were patients referred from other institutions in Bogotá, thus constituting a screened population for the hospitalization pavilions with minimum probabilities of requiring intensive care management or death, which implies a selection bias in the sample.
Since Fundación Hospital San Carlos did not have UCI service for most of the time when the sample collection was being performed, there is a possibility that patients admitted to the emergency room that required mechanical ventilation were sent to another institution before they could be included in the study. It is also probable that there were cases of patients with exacerbation who died during hours not available for sample collection and, therefore, could not be included.
Another limitation of the study was establishing definitions accepted for inclusion criteria and data analysis. The definition of chronic lung disease that was coined sought to be sensible, considering that few patients have pulmonary physiology studies and that some of those who actually had them were not available at the time of the survey or follow-up. This is why the diagnosis reported by the patient and relatives was chosen, making it difficult to determine which patients actually had a chronic lung disease and which type.
The difficulty in establishing the definition of hypoxemia, anemia and erythrocytosis is also relevant because normal values for Bogotá differ from those accepted at sea level, where most definitions are validated. For this, oxygen saturation was chosen considering the dissociation curve of hemoglobin and the values of red blood cell parameters of studies that have determined normal values in high altitudes 18,19.
Determining which patients had chronic hypoxemia at admission was difficult because, in most cases, there were no data, and for those who received home oxygen its indication was unknown.
The results suggest the need for further studies to clarify the relevance of erythrocyte parameters in exacerbations of chronic lung disease, both at sea level and in populations located at higher altitudes, as in this case.
The usefulness of phlebotomy in patients with erythrocytosis in this context remains uncertain, as well as the extrapolation of hematocrit values relevant to Bogotá. Studies that include phlebotomy in the prognosis of exacerbation should also evaluate the proper adherence to treatment, including supplemental oxygen as a primary factor to prevent recurrence of erythrocytosis.
In conclusion, this study could not determine a statistically significant association between red blood cell parameters and prognosis of patients with exacerbation of chronic lung disease; however, there is a tendency for extreme values to have adverse outcomes.

