











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkIntroduction
The aortic artery is a high caliber vessel which originates in the vascular ring of the aortic valve and descends until dividing into common iliac arteries in the sacral promontory 1,2. Its histological structure, to which various pathological processes have been associated, has antiatherosclerotic, antithrombotic, as well as capacitor, conductor and pumping functions 2. The aorta presents subdivisions, determined by anatomical relationships, such as the aortic arch (AA), which originates in the posterior portion of the second right sternocostal joint and ends behind the second left sternocostal joint 1.
The vascular structures that supply the upper limbs and the brain originate in the AA: the brachiocephalic artery trunk, the left common carotid artery and the left subclavian artery 2. According to different investigations, the frequency of this pattern is 65-92.6% 3-8. The remaining structures correspond to anatomical variations, most likely caused by gestational processes, and are related to the arrangement of the primitive vascular branches within AA 9. Some of these variations usually have influence on different pathological processes, surgical approaches and complications 10.
Similarly, the existence of these variations has become a risk factor for the development of aortic disease 4. Therefore, knowing these vascular distributions is highly relevant for diagnosing and planning open and endovascular surgical approaches to the aortic disease 4,10,11, leading to the need for deeper knowledge on the frequency of anatomical variations of blood vessels originating in the AA, as well as on the calibers of each vascular structure in a sample of Colombian population.
Materials and methods
A descriptive cross-sectional study was carried out by dissecting 35 cervicothoracic plastrons, which were obtained from Anfiteatro de Medicina Humana (Human Medicine Amphitheater) of Universidad de Ciencias Aplicadas y Ambientales (UDCA), and donated in agreement by the Instituto de Medicina Legal y Ciencias Forenses (Institute of Forensic Medicine and Forensic Sciences). Plastrons with cervical congenital malformations, evidence of cervical trauma, cervical tumor processes or anatomical alterations caused by manipulation after removal of the corpse were not considered.
The dissection process was performed by removing fatty tissue and the pericardium covering the ascending aorta, the aortic arch and the blood vessels in the aorta. Then, the vascular diameters of the aortic arch were measured with a digital caliper (Figure 1). Throughout the process, photographic evidence was taken using a Nikon 1 J5 camera.

Source: Own elaboration based on the data obtained in the study.
Figure 1 Measurement of vascular diameters and intervascular distances.
After the observations and measurements, the information was tabulated in Microsoft Excel 2013 based on Natsis et al. as a classification parameter 3 (Table 1). The data regarding the vascular measurements were tabulated and cataloged according to the classification of Herrera et al.11.
Table 1 Representation of anatomical variations.

AA: aortic arch; BTC: brachiocephalic trunk; LCCA: left common carotid artery; LSA: left subclavian artery; RCCA: right common carotid artery; RSA: right subclavian artery; BA: bovine arch; LVA: left vertebral artery; ARSA: aberrant right subclavian artery; TIA: thyroid ima artery.
Source: Own elaboration based on 3.
The data obtained from the classification of anatomical variations were treated through absolute and relative frequencies for the corresponding comparison against other national and international studies, while the evidences obtained from the measurement of vascular diameters were handled through mean and standard deviations.
This research was developed in strict compliance with the criteria for performing medical-legal autopsies as specified in Decree 786 of 1990 12. The principles of the Declaration ofHelsinki 13 were also followed, guaranteeing a respectful treatment of the anatomical parts, and keeping the confidentiality, dignity and integrity of the deceased person. Likewise, according to the parameters of Resolution 8430 of 1993 of the Ministry of Health 14, the research was approved by the Institutional Ethics Committee.
Results
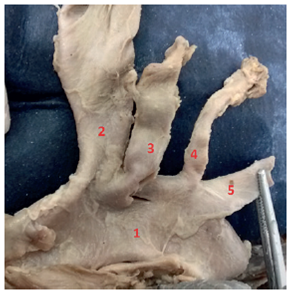
The most frequent type of AA in the sample was Type I or usual pattern (Figure 2) with 74.29% (n = 26). The Type II AA or bovine arch (Figure 3) was found in 11.43% (n = 4) of the study population, Type III AA (Figure 4) in 8.57% (n = 3), Type V AA (Figure 5) in 3% (n = 1), and Type VIII AA (Figure 6) in 3% (n = 1). Types IV, VI and VII were not found in this study (Table 2).

Source: Own elaboration based on the data obtained in the study.
Figure 2 Aortic arch Type I. 1: AA; 2: BTC; 3: RCCA; 4: LSA.

Source: Own elaboration based on the data obtained in the study.
Figure 3 Aortic arch Type II. 1: AA; 2: BA; 3: BCT; 4: LCCA; 5: LSA.
Source: Own elaboration based on the data obtained in the study.
Figure 4 Aortic arch Type III. 1: AA; 2: BCT; 3: LCCA; 4: LVA; 5: LSA.

Source: Own elaboration based on the data obtained in the study.
Figure 5 Aortic arch Type V. 1: AA; 2: Common trunk originated from 3: RCCA and 4: LCCA; 5: ARSA; 6: LSA.
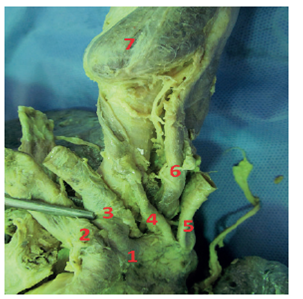
Source: Own elaboration based on the data obtained in the study.
Figure 6 Aortic arch Type VIII. 1: AA; 2: BCT; 3: LCCA; 4: TIA; 5: LSA; 6: esophagus; 7: thyroid gland.
The mean diameter of AA before the origin of the first blood vessel was 23.4mm±3.36. The diameter of the brachiocephalic trunk (BCT) was 9.95mm±1.90, of the bovine arch (BA) 10.1mm±1.37, of the left common carotid artery (LCCA) 5.78mm±1.64, of the left subclavian artery (LSA) 8.0mm ± 2.3, of the left ventricular artery (LVA) 3.97mm±0.47, and of the thyroid ima artery (TIA) 6.1mm (Table 3).
Table 2 Distribution of anatomical variations of the aortic arch.

Source: Own elaboration based on the data obtained in the study.

Discussion
The study of the anatomical variations of the AA is of great importance for morphological research due to its application in the clinical and surgical approach to the aortic disease. Different morphological patterns of this structure have been described; the first one is Type I or usual pattern, which consists of the emergence of three vascular branches known as arterial brachiocephalic trunk (BCT), left common carotid artery (LCCA) and left subclavian artery (LSA). According to the literature, the prevalence of this anatomical distribution is 71.383%; in this study, a frequency of 74.29% was found, which was similar to the 74.4% reported by Celikyay et al.7 (Table 4).
Type II AA or bovine arch (AB) has a common vascular trunk between the BCT and LCCA, and one LSA alone. Its frequency has been described in 15%-21.1% (Table 4). In this study, this was the second most frequent distribution with 11.43%, less than that reported by Natsis et al. in Greece 3, by Celikyay et al. in Turkey 7 and by Herrera et al. in Colombia 11,15. AA Type II has proven to be a risk factor for premature aortic disease and, therefore, knowing how frequent it is among the general population could help determining the probability of acute aortic syndromes in patients with this abnormality 4.
Type III AA is defined as the origin of BTC, LCCA, a left vertebral artery (LVA) originating directly from the AA and LSA. This pattern has been reported with frequencies between 0.16% and 8.2% (Table 4), whereas this study found a frequency of 8.57%. Although this figure is beyond the aforementioned range, it is very close to that reported by Herrera et al. for the Colombian population 11, and both are higher than those obtained by Natsis etal.3 and Celikyay etal.7 (Table 4). This variation of AA may be a population preference, which would be relevant for the clinical and surgical approach to aortic disease.
Regarding Type IV AA, there is a great discrepancy between population studies around the world because some authors use this category to include all anatomical variations that do not fit into any of the first three groups, while others such as Natsis et al.3 classify up to 8 types of AA in a much more accurate morphological description. According to the first approach, Type IV anatomical variations have a frequency of 0.8-23% -a very wide range- in the population of other countries. In this study, this group of data had a frequency of 6%, a number higher than that reported by Herrera et al.11 for the local population (3.3%), but within the range described for the world population (Table 4).
Table 4 Distribution of anatomical variations of the aortic arch in the world population and in this study.
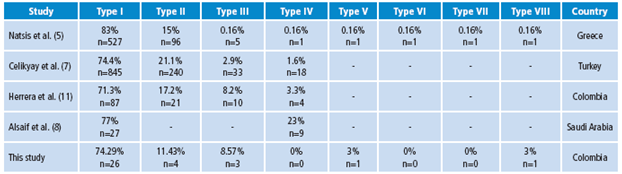
Source: Own elaboration based on 11.
To provide a more detailed anatomical description of Type IV variations, a sub-classification was done based on Natsis et al.3 including the following morphological patterns:
Type IV: absence of BTC; the right subclavian artery (RSA) has its own origin; a common trunk between the right (RCCA) and left (LCCA) common carotid arteries is seen, and LSA is observed.
Type V: there is a common trunk between RCCA and LCCA; LSA and aberrant right subclavian artery (ARSA) are observed. Type VI: there is a common trunk between LCCA and RCCA, and between RSA and LSA.
Type VII: absence of BTC. RSA, LSA, RCCA and LCCA have an independent origin.
Type VIII: TBC, median thyroid artery (MTA), LCCA and LSA are observed.
Natsis et al.3 reported only one case (frequency 0.16%) of each subtype (Table 4). This study found only one Type V case and one Type VII case, with a frequency of 3% each. Although both studies found only one case of each type, the frequencies differ from each other because of the population sample considered for each study, which does not rule out the low occurrence of these anatomical variations in the general population.
The analysis of blood vessel diameters is also of great importance not only at the morphological but also at the surgical level, during the preoperative assessment of aortic disease for endovascular or open intervention 8. While the diameter of AA in the Colombian population described by Herrera et al.11 has an average of 20.1mm, this study found an average of 23.4mm (σ=3.36), which does not represent a significant difference. No other consulted study measured AA (Table 5).
Table 5 Diameter measurements in millimeters of the main blood vessels in the world population and this study.

Source: Own elaboration based on 11.
In other studies, BTC had a minimum diameter of 9.7mm and a maximum diameter of 21.82mm. In this research, a diameter of 9.95mm (σ=1.90) was determined, which is within the described range and is slightly lower than the lower cut-off point (Table 5). The measures taken in this study and in Herrera et al.11 showed lower averages than those obtained by other authors in different countries, perhaps, due to the height of the Colombian population, which tends to be smaller.
The diameter of the bovine arch or bicarotinal trunk (common origin of BTC and LDDA) showed an average of 10.1mm (σ = 1.37), a figure much lower than those reported by Yeri et al. in Argentina (cited by 11) and Herrera et al. in Colombia 11 (Table 5).
The LCCA is responsible for supplying oxygenated blood to the structures of the neck and a large part of the brain 9. The diameter of this artery was 5.78 mm (σ=1.64), quite similar in the upper cut (7.42 mm) to the findings of other studies in the world, but with a minimum value of 4.14mm that shows that vascular diameters in the Colombian population may be smaller than those reported in other countries (Table 5).
The LSA, in charge of supplying the left upper limb and some thoracic structures, had an average of 8.0mm, close to that reported by Herrera et al.11, 7.6mm, and smaller than those reported in other studies. The standard deviation obtained in this study (σ=2.3) allowed determining a maximum value of 10.3mm, which is within the range reported in the world (7.6-17.42mm), as well as a minimum value of 5.7mm, which is lower than this range (Table 5).
Although the measurement of LVA is part of the study of anatomical variations, it was not reported in any of the works consulted, which makes comparing results impossible. In this study, the diameter of such artery had a mean of 3.97mm (σ=0.47) (Table 5).
The TIA, one of the least described arteries in morphological studies on AA, was not reported in the works consulted, which hinders comparison. In this research, the only case found had a diameter of 6.1mm (Table 5).
Conclusions
The distribution of the aortic arches in the sample studied had frequencies similar to those shown in previous studies on local and world population, being AA Type I the most frequent pattern.
AA Type II or bovine arch had a lower frequency than all the studies reviewed. Given the proven association between its presence and a higher incidence of aortic disease, this finding could mean that the Colombian population has a lower risk of contracting pathologies related to this anatomical variant 16-22.
Type III AA reported a much higher frequency in this study, as well as in the study by Herrera et al.11 done on Colombian population 11, compared to research from other parts of the world. This could be a major particularity of the Colombian population in relation to endovascular and open surgery, especially when planning highly complex surgical procedures.
Type IV AA and its subdivisions were found to be less frequent compared to the other groups. It should be noted that two rare blood vessels were described in this group: the right aberrant subclavian artery (RASA) and the thyroid ima artery (TIA); therefore, doctors and surgeons are advised to be attentive to the presence of these structures in Colombian patients.
In general, the diameters of blood vessels from the AA had lower mean values than those reported in studies from other countries. This is most likely due to anthropometric differences in height and weight, which in the Colombian population tend to be lower than in the rest of the world 11,15. The presence of smaller diameters in the vessels derived from AA increases the risk of vascular disease by 6.15%, in consequence, the Colombian population may be at higher risk of acquiring this disease.
Conflict of interests
None stated by the authors
Funding
The research was funded by Universidad de Ciencias Aplicadas y Ambientales (UDCA).

