











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Diabetes mellitus (DM) is a chronic, non-communicable disease. 1 In 2014, the World Health Organization (WHO) identified it as a pandemic and reported that 422 million people suffer from this disease worldwide. 2,3 According to the International Diabetes Federation (IDF), by 2035, this figure will reach 592 million. 4 As a result of this pathology, there are more than five million deaths per year.
One of the chronic complications of diabetes mellitus type 2 (DM2) is diabetic foot (DF) 3, which can result in amputation if it progresses to an ulcer. One of the consequences of such measure is the profound deterioration in patient's self-care, productivity and psychosocial functions, or even death. 2 Therefore, this is a complex disease that causes greater use of health services and requires up to 11% of the total health expenditure of each country. 3 This condition is responsible for 50% of all non-traumatic amputations. In addition, people who have one amputated leg lose the other in less than five years 5; about 20% of patients with DM2 manifest a picture of DF in the course of their life, and about 20% of them undergo amputation. 5 In Chile, in 2014, one in every 200 diabetics underwent and amputation and more than 16 000 received treatment for foot ulcers. During the last decade, the rate of amputations in patients with DM2 has increased by 28%. 6
The measures taken by the Ministry of Health of Chile and other international organizations to prevent foot ulcers are not effective. This can be seen daily in primary health care (PHC), where patients attend the first consultation due to the presence of a skin disorder on their feet. 7 The most relevant aspect should be the identification of patients at risk, in order to act in a timely manner and prevent the onset of the lesions. The prevention of DF is important for primary care systems, since the expenses generated by the treatment of complications can be reduced -the disease requires around 54.5 billion dollars a year in Latin America only for its management- and also because the quality of life of patients can be improved, given that the disease is a fundamental part of their daily lives and that of their relatives too. 8 From this perspective, a study based on the natural history of this ailment, with prevention at different levels of care, demonstrated a reduction in amputations of up to 85% 2, which proves that DF ulcers are preventable in most cases.
Education is a fundamental tool for prevention; however, for these actions to be successful, psychological, sociocultural, interpersonal and real needs of the individual who suffers from this pathology must be considered. It is essential that this process is based on the reality and experience of patients, since many times the delivery of information does not allow an adequate participation, not forgetting that what they know and what they would like to know should also be considered. 9
In consequence, it is important to note that inadequate perception of risk, by both the patient and the healthcare team, is a clear cause of the incorrect assessment of danger and, therefore, a human error. 10 It possible to infer that healthcare professionals should know about the perception of their users in relation to the occurrence of signs and symptoms that afflict them. All these factors justify the development of research to learn about the perception of users regarding their health condition and determine how educational and therapeutic intervention should be done at all levels of the disease and its complications. 5
With this in mind, the personnel of a family health center (CESFAM), in southern Chile has developed multiple strategies to reduce the onset of ulcers in DF patients. However, these measures seem to be insufficient considering that out of 667 diabetic patients, 12 developed wounds to their feet, five of them underwent amputation and the remaining seven are still receiving assistance from nurses. 7 This has an impact on the consumption of human and material resources, which has increased progressively, and has become impossible to maintain.
It is important to note that, despite carrying out the activities suggested in the documents delivered by the Ministry of Health regarding the execution of DF assessments -education about the correct use of footwear, socks, nail cutting, grooming of the feet, proper feeding, and podiatric controls- and the cardiovascular health program, no favorable changes have been observed in terms of the decrease in the incidence of ulcers. For this reason, multiple analyzes have been carried out to determine the causes of this situation, without obtaining results that allow guiding effective improvement plans with patients. 7 Given this situation, research on the perception of the incidence of foot ulcers in DM2 patients who presented with wounds in 2015 is necessary with the purpose of contributing to improve their quality of life.
This study seeks to understand the perception of DM2 patients in relation to the cause to which they attribute the occurrence of ulcers on their feet. The objectives are to discover the meaning of the concept of ulcer in DF and DM2, to understand what it means to live with a DF ulcer and to investigate the role of the health team. This investigation is expected to provide relevant information to design more comprehensive strategies and treatments.
This contribution implies knowing and considering the unmet needs of these patients in care plans, cultural aspects involved and beliefs related to health behaviors and self-care, since these are elements that will act systematically as facilitators of the changes in their behavior to favor improvement.
Materials and methods
Considering the nature of the research object, a qualitative, exploratory, descriptive and interpretative paradigm was applied to an intrinsic case study 11,12, whose purpose is to describe important aspects of a little known phenomenon, document it and explain its causes.
The non-probabilistic, intentional sample of cases, based on criterion and convenience 13, consisted of 12 DM2 patients who developed DF ulcers and were treated at CESFAM in 2015. The inclusion criteria were: age >18 years regardless of gender; normal cognitive, oral and auditory abilities to allow an effective communication and understanding of the objective of study, and willingness to participate voluntarily in the study, previously signing an informed consent.
Focus group was selected as the qualitative technique for data collection (two groups of six members each). Testimonies were collected until reaching the point of saturation, that is, repetition of ideas or gathering enough evidence to guarantee the credibility of the investigation. 14 A guideline was used to ensure that all subjects were explored, for example: Can you say what an ulcer is for you? Have you heard of DF ulcer? What do you think was the cause for the occurrence of your ulcers? An audio recorder and field notes were used, with the corresponding authorization, to support the collection of information in an exact way, as narrated by the participants themselves.
The analysis of data followed the constant comparison scheme 15 through a generative and constructive method in which inductive coding of categories was combined with constant comparison. Progressively, information that matched the object of study was reduced in three phases that formed different types of operations: segmentation and coding of units of analysis; identification of the main topics or emerging thematic nuclei, and integration and interpretation of the results in qualitative domains. 16,17 Information was manually structured in three levels by the researchers:
Level 1: Identification of units of analysis (textual narrations of the participating subjects) and segmentation for grouping into descriptive categories.
Level 2: A system of emerging thematic nuclei or metacategories was built from descriptive categories.
Level 3: As a consequence of the previous level, qualitative domains were identified through a sequential and transversal analysis of metacategories.
It should be noted that under this paradigm, data collection and subsequent analysis were concurrent 12, and that categorization and segmentation were two operations that were executed simultaneously because the used criterion belonged to a certain concept or topic, where the units that made reference to a certain idea were included in the corresponding categories.
Reliability was guaranteed using standards of rigor determined by: truth value or credibility (work over a prolonged period of time, continuous observation, triangulation, verification among participants), applicability or transferability (collection of abundant descriptive data, dense and meticulous descriptions), consistency or dependence (review tracks, including field notebooks, interview notes) and neutrality or confirmability (triangulation).18
Ethical considerations were safeguarded since this project was authorized by the Scientific Ethics Committee of the Universidad de La Frontera through Act No. 080/2016. The following ethical principles in research were considered 19,20:
Implicit social value since the results will provide probable social and scientific benefits.
Scientific validity was assured by a rigorous design, and the products were also triangulated by researchers.
The equitable selection of subjects was safeguarded by identifying key informants, that is, those people who contributed to the study because they were directly related to it.
A favorable risk-benefit ratio, focused on minimizing potential risks and increasing benefits proportionally, was accomplished following the non-maleficence and beneficence principles, without generating conflicts to the participants.
Independent assessment refers to non-distortion of research results, which was endorsed by the Scientific Ethics Committee of the University.
The informed consent, authorized by said Committee, included respect for the voluntary and conscious participation of the subjects, offering them the opportunity to raise questions and doubts, and withdraw from the study if they wished.
Respect for the subjects enrolled was met by giving them the possibility of changing their mind, ensuring confidentiality of the data and delivering the results of the study.
Results
Level 1
495 units of analysis, relevant to the study, were obtained and grouped into five emerging categories as shown in Table 1.
Table 1 Percentage distribution of coded emergent categories.
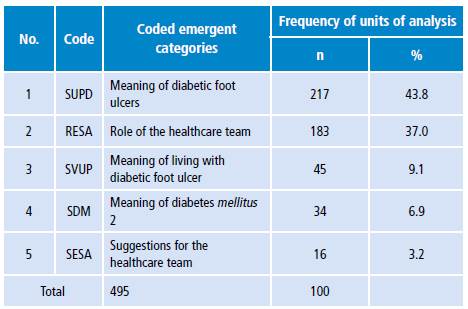
Source:Own elaboration based on the data obtained in the study.
As a result of this process, five emerging categories were obtained. They are presented in Tables 2, 3, 4, 5 and 6.
Table 2 Frequency distribution of units of analysis for the category "Meaning of diabetic foot ulcers" (SUPD).
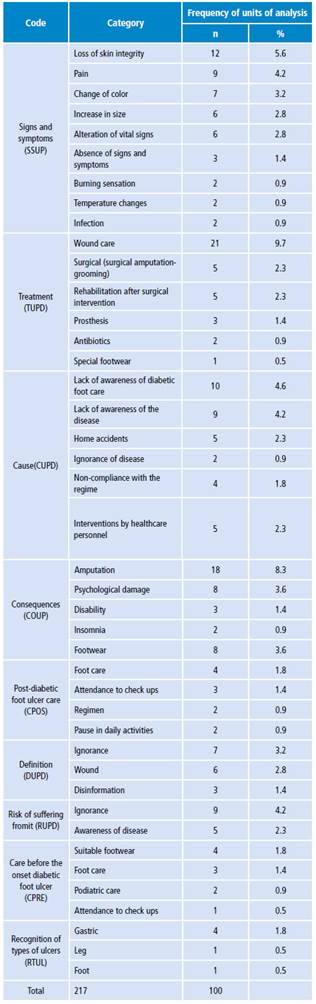
Source: Own elaboration based on the data obtained in the study.
Table 3 Frequency distribution of the units of analysis of the category "Role of the healthcare team" (RESA).
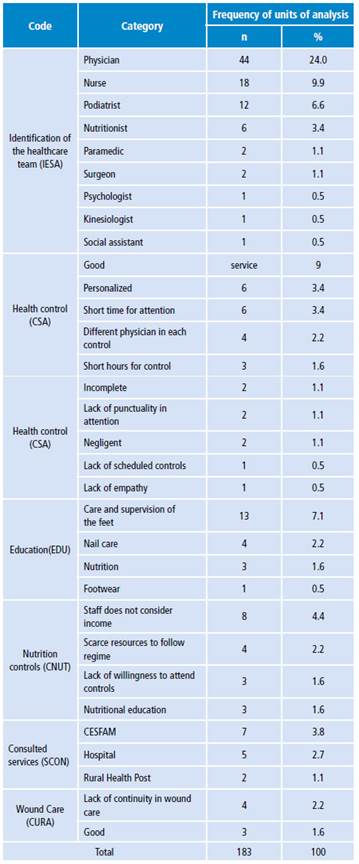
Source: Own elaboration based on the data obtained in the study.
Table 4 Frequency distribution of the units of analysis of the category "Meaning of living with diabetic foot ulcer" (SVUP).
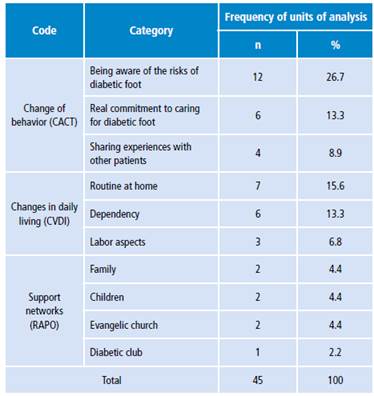
Source: Own elaboration based on the data obtained in the study.
Table 5 Frequency distribution of the units of analysis of the category "Meaning of diabetes mellitus 2" (SDM).
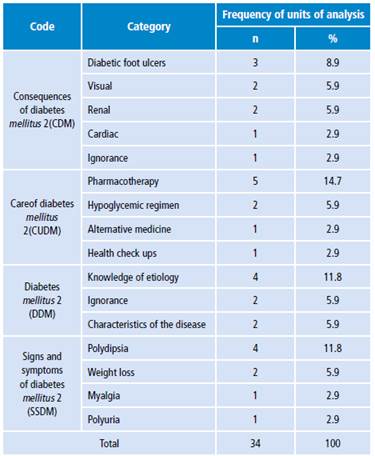
Source: Own elaboration based on the data obtained in the study.
Table 6 Frequency distribution of the units of analysis of the category "Suggestions for the healthcare team" (SESA).
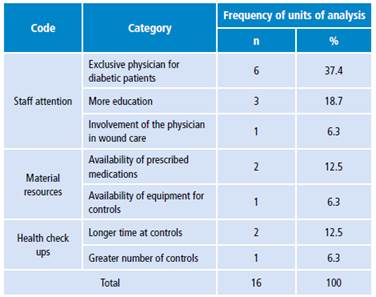
Source: Own elaboration based on the data obtained in the study.
Level 2
Three thematic nuclei or metacategories emerged at this level:
Metacategory 1: Statement regarding concepts associated with the pathology and the role of the healthcare team.
Metacategory 2: Experience of living with a DF ulcer.
Metacategory 3: Suggestions for future consultations.
Level 3
Based on the aforementioned level, two qualitative domains arose as shown in Table 7:
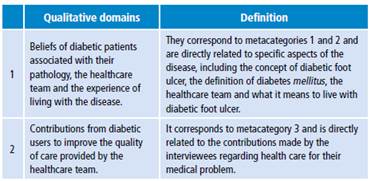
Examples of domain 1 stories:
"[...] It is a small thing that appears on the foot and gets bigger and bigger. It has to be taken care of because if you don't, it may lead to something severe like an amputation, as was my case [...]" "[...] Diabetes is the malfunction of the pancreas [...]" "[...] A doctor told me that the feet are like dead because blood does not circulate, so you could be set on fire and would not feel the toes because blood does not circulate, it does not reach, so you should not get close to the fire [...]"
"[...] One time, a doctor strongly hunted me down, looked at my exams and told me that I could have a stroke at any time and told me to leave. She did not even tell me the result, she only treated me once. So, the point is knowing what is happening, not that they scold you and scare you [...]"
"[...] The podiatrist cut me so deep that I drew blood and everything began at that point [...]"
"[...] The problem is that you are always treated by any physician, and only for like 15 minutes per patient. You don't have time to ask anything [...]"
"[... ] The change of physician means the loss of continuity of the indications, because a physician tells you one thing and you already trust him, and then it starts all over again [...]" "[...] Humanitarianly, I have been treated better by nurses than by physicians [...]"
Examples of domain 2 stories:
"[...] There should be a diabetes doctor, someone who will follow you up and has more specific knowledge of diabetes, someone who feels confident and committed to the issue [...]"
"[...] I would like to receive better information regarding diabetes, what the consequences of this disease are [...]"
"[...] If you are cited for exams, that they are taken early; they call you at eight o'clock and take the sample at eleven o'clock and you have to come on an empty stomach. Just imagine, I use insulin and my sugar levels drop quickly and I cannot inject myself until I eat. There should be priorities [...]"
"[...] That a doctor and a nurse checked the wounds, but there must be a doctor. Another aspect is that sometimes medications are not available and the doctor gives you the prescription so you have to buy them, so I must have money and sometimes
I don't have any. It is also assumed that medicines should not fail us [...]"
"[...] That they take a reasonable length of time for controls and that they are not done so fast. They should be done calmly because some of them just do it in a rush. Also, they should have the drugs available because the government is supposed to provide them for us and I have spent up to 22 000 Chilean pesos in the drug store when the drugs are not available in the pharmacy [...]"
Discussion
Given the specific objective of discovering the meaning of DF ulcer and DM2, some informants reported that it is a wound while others were uninformed. If they are asked about the types of ulcers, it is inferred that they do not recognize the word "ulcer" as an injury to their feet. However, the literature defines it as a "neuropathic-based clinical alteration induced by sustained hyperglycemia, in which injury and/or ulceration of the foot occurs with or without coexisting ischemia and previous traumatic trigger". (21, p1) All of this could be supported by what was expressed as "Suggestions to the healthcare team" in relation to the service provided by the staff, more education on the subject and the frequency of health checkups, since patients ask for longer interventions by the corresponding professionals.
With respect to the risk of developing a DF ulcer, the literature states that "between 40 to 50% of diabetic patients will develop an ulcer on their feet during the course of their illness and, of these, 20% will require amputation". (21, p1) However, the key informants of this study refer ignorance of the occurrence of the ulcer, which may mean that not all of them have been educated on this issue and, therefore, do not know appropriate care measures to prevent a possible injury to their feet. In this regard, it is important to note that for DF prevention, the professional team, in addition to examining the lower limbs, must be able to motivate and educate the patients to check and care for their feet daily, encouraging self-care. 22
Subjects identified the signs and symptoms experienced when the ulcer appeared on their feet, which correlates to a large extent to the signs exposed by the literature. 23 They recognize, particularly, the lack of awareness of care as a cause associated with the occurrence of ulcers, which coincides with the lack of guidance on how to take care of the feet. 24 In turn, amputation is mentioned as a consequence that can lead to a second amputation, which is compatible with another study carried out in North America stating that 9-20% people with diabetes underwent a second amputation 12 months after the first amputation, and that, within the 5 five years after the initial amputation, 28% to 51% surviving patients would need to undergo a second intervention on the same limb. 25
Regarding the meaning of DM2, patients stated that they know information related to its etiology and are able identify some signs and symptoms of the disease, which coincides with other studies. 26-28 These findings may arise due to inadequate perception by the healthcare team of the educational needs of the users and reveals the need to rethink a way of working that adapts to local reality and the characteristics of the community. Therefore, education is a fundamental strategy to achieve self-care and promote commitment to health. 29,30
Regarding the second specific objective "To reveal what it means to live with a DF ulcer", patients expressed undergoing changes in the basic activities of daily life (BADL), which are "universal, related to living conditions and to basic requirements specific to each person, and imply a minimum cognitive effort, so they are acquired early in order to achieve personal independence". (31, p268) They usually included eating, grooming, bathing, dressing, personal mobility, sleep and rest.
The revelations of these discourses are related to other studies on the topic which stress that the loss of mobility, caused by the ulcer or by the treatment received by diabetic people with injuries in their feet, generates considerable restrictions in the performance of daily life activities associated with domestic work, leisure activities and work, and cause different levels of disability that, in turn, have a negative impact on the quality of life, thus generating highly stressful situations. 32,33 This could be attributed to the feeling of threat that puts the well-being of the patient at risk; therefore, the healthcare team should implement strategies that allow patients to cope with the condition, leading to important changes that require previous information and the perception of support. 34
In relation to the third objective, "to investigate the role of the healthcare team", professionals identified by users were physicians, probably due to their intervention and decision-making at times of decompensation of the pathology, and nurses, because of ministerial protocols 35 and wound care.
Most of the informants reported that protocolized activities carried out by the healthcare team 35, including health checkups, have a good but short personalized attention and that the rotation of physicians implies the lack of follow-up and constant changes in indications. Furthermore, they expressed difficulties for obtaining appointments, lack of punctuality in attention, failure to comply with the appointments and, finally, stressed the lack of empathy of some people who perform the interventions. This may be related to work overload in employees, since the time allocated for consultation (30 minutes) is insufficient to address this type of user. It could be assumed that the aforementioned factors reflect the flaws of knowledge acquired, since not all necessary activities described to prevent the complications of DM2 are fulfilled 29, reflecting again the importance of health education in relation to the needs of users.
With regard to wound care, they are considered adequate; however, lack of continuity was reported, especially in patients who require the procedure at home, probably because of lack of personnel, lack of coordination in case the responsible professional is absent or external factors such as lack of mobility. It has been demonstrated that multidisciplinary work regarding care of DF patients may help to accelerate the healing rate of the ulcer or influence its recurrence and the occurrence of a second amputation in diabetics. 36 This could explain the need for more comprehensive care in the management of patients with DF ulcers.
Likewise, the vast majority of key informants reported that they have received nutritional education, but aspects such as income are not considered, hindering adherence to the regimen due to low family income and the implicit expenses derived from the treatment of DF ulcers. This coincides with a study stating that compliance with dietary recommendations was mostly partial. 36 The findings of this work may be related to the fact that the healthcare team does not know the characteristics and problems of the population and, therefore, care, indications and education have not been adapted to the real context of users to respond accurately to their needs. It should be borne in mind that medical and dietary treatment influence dietary behavior, so health professionals must consider sociocultural determinants when designing and implementing treatment strategies. 36
Finally, suggestions provided by the users endorse the need for a "multidisciplinary team focused on delivering the necessary knowledge and tools to allow patients to engage in the care of their health". (22, p26) In the last 15 years, care of diabetic patients has been proven to be optimal only when financing and human resources have sufficient quality 2, so it is essential to know and understand the perception and behaviors of DM2 patients, in order to redirect the model of care towards them, incorporating comprehensive care that includes biological, psychological, social and spiritual well-being dimensions according to the characteristics of the community. 29
Conclusions
DF ulcer has been described as a wound associated to gastric ulcers in most cases. Without assuming the risk of developing it, users recognize the lack of self-care, home accidents and non-compliance with the diet as the cause of their occurrence. Actually, they understand that the consequence of DF is the amputation of the limb.
With respect to the meaning of DM2, a few users understand its etiology. Others identify signs and symptoms such as polydipsia, weight loss, myalgia and polyuria. In turn, pharmacological treatment has greater adherence compared to hypoglycemic regimen.
Regarding "what it means to live with a diabetic foot ulcer", they stated that they have experienced changes in daily life and in home routines, absence from work and degree of dependency.
Physicians are frequently identified as participants of the healthcare team, followed in order by nurses, podiatrists, nutritionists, paramedics, surgeons, physiotherapists, psychologists and social assistants. Additionally, activities related to the healthcare team are education, taking good care of the feet and nails, diet and appropriate footwear. About health controls, good personalized attention was reported, as well as short periods spent in care, which are insufficient and done by different doctors in each control; an exclusive physician for each patient was suggested.
In conclusion, it was confirmed that health education, based on the perceived needs of users, is one of the most important strategies for self-care and prevention of this disease. It is worth noting that the results of this study are not generalizable and only represent the opinion of the diabetic patients enrolled in the CESFAM Belarmina Paredes of the Futrono borough, who presented foot ulcers in 2015.

