











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroducción
In Brazil, an estimated 19 million people are older adults and these figures are expected to reach values higher than 32 million by 2025. 1 As population ages, frailty becomes more prevalent 2, since older people have a higher risk of falling, developing disabilities, institutionalization and mortality in comparison to younger people. 3
The frailty process is affected by a complex interaction of physiological mechanisms related to ageing that unbalance homeostasis in older people. 4 One factor that may worsen a frail elderly is stroke, as it can cause multiple impairments such as motor, sensorial, cognitive, speech and perception impairment 5, reducing the coping skills for organic and psychological stress and making the person more vulnerable to illness. 4 Screening older adults at high risk of frailty may lead to identify persons who would benefit from specific interventions for early detection and prevention. 3
Due to the lack of evidence of the main aspects of frailty in Brazilian elderly people regarding stroke through the use of a fast checklist, the aim of this study was to investigate the relation of stroke and its effects on the frailty process in older adults. Additionally, this work attempts to correlate the frailty condition assessed through the Kihon Checklist with body mass index, functional aspects and deficits caused by the stroke.
Material and methods
This longitudinal observational study was conducted in a Stroke Unit of a university hospital of the South of Brazil. This research was approved by the Ethics Committee of the Clinical Hospital of the Federal University of Paraná by means of certificate CAAE 38715714.2.0000.0096. It was classified as minimal risk according to the Declaration of Helsinki, considering that the personal information collected could be psychologically sensitive. Confidentiality of all data was preserved.
The subjects were patients aged 60 years or older -considered as older adults in Brazil 6-, who had suffered from ischemic stroke in the middle cerebral artery (MCA); were hospitalized after suffering a stroke in the period between February and November 2015; and returned to the outpatient service for a neurological appointment in the same hospital one month after discharge.
All volunteers signed the informed consent statement; in cases when the patient was unable to sign, it was signed by a responsible relative. The exclusion criteria were patients who suffered transient ischemic attack or stroke mimics; stroke caused by another artery or hemorrhagic ischemia; patients with a history of dementia; difficulty to understand and/or respond to the questionnaires or without family support to do so.
The baseline data related to the patient's life condition just before the stroke was collected during hospitalization, including (i) sociodemographics; (ii) lifestyle and health-related characteristics; and (iii) frailty condition by Kihon Checklist (KCL). To minimize the bias in this data collection phase, the evaluation was applied only by the main researcher and subsequently confirmed by relatives and/ or close friends of the patients.
Sociodemographic data regarding age, birth, sex, marital status, occupation and retirement were self-reported. The lifestyle questionnaire was elaborated by the author of the research, including "yes" or "no" questions about smoking and ethylic habits (current and past) and sedentarism. Furthermore, health-related characteristics about systemic hypertension, diabetes, obesity (Body Mass Index [BMI]>25) and dyslipidemia were collected from the medical report of each patient.
KCL is an index developed by the Japanese Ministry of Health, Labor and Welfare to screen fragility in older adults, in order to identify those who are at high risk of becoming functionally dependent. It includes 25 "yes" or "no" questions, divided into eight categories: total KCL, instrumental activities of daily living (IADLs), physical domain, nutrition, eating, socialization, memory and mood. 7-9
The following cutoff points for KCL were assigned: total KCL (sum of all questions) >7, indicating risk to become frail; IADL domain >3, for required supervision to perform activities; physical domain >3, representing low physical activity; nutrition domain =2 (adopted cutoff point for BMI<20.5 in Brazilians as suggestive of malnutrition); eating domain >2, suggesting oral dysfunction; socialization domain >1, signifying seclusion; memory domain >1 for cognitive impairment; and mood domain >2, indicating depression. A higher KCL score represents a frailer health condition, as adapted and validated for Brazilians in 2014. 8,9
The follow-up data were collected one to six months or more after discharge, when the patients returned to the neurological outpatient service for an appointment in the same hospital. During the appointment, elderly patients were reassessed using the KCL, the Rankin Scale (mRS) and the National Institutes of Health Stroke Scale (NIHSS). The mRS is frequently used to assess functional outcome after a stroke with a scale ranging from 0 to 6: 0 (zero) represents no symptoms, 1-5 indicate different scales of disability and functional dependency, and 6 indicate death. 10 The NIHSS is an assessment tool that indicates the severity of the neurological lesion and the prognostic outcome through 11 items that measure each deficit. 10
Statistical analyzes
A descriptive analysis was used to describe age and body mass index (BMI) (mean and standard deviation), and the nominal variables (sex, marital status, activity, lifestyle, hypertension, dyslipidemia and obesity).
The means of baseline KCL domains and follow-up data collections were compared using the paired t-test. Furthermore, the raw score of each KCL domain was dichotomized according to KCL cutoff points to compare the percentage of frail older adults between baseline and follow-up, using the Chi-square test.
The relation between stroke and frailty (total KCL) was established by analyzing variances in the baseline and follow-up data using the Friedman nonparametric test. Finally, the correlations among frailty, BMI, mRS and NIHSS were analyzed using the Kendall's test.
The critical value for significance was established by p<0.05. Death in the follow-up data was considered as missing data, with the exception of the mRS that provides scores for death cases.
For statistical analysis, the SPSS Statistics software (Version 22, IBM Inc. Chicago, IL, USA) was used.
Results
The total amount of patients from whom data were collected was 25, but 9 were excluded for not participating on the second phase of the research. The baseline data consisted of 16 patients (mean age 72.19±7.20 years) who met the inclusion criteria for the study. Most of the subjects were male (68.8%; n=14); married (53.3%; n=9), retired (68.8%; n=11) and sedentary (68.8%; n=11). The BMI indicated that approximately one third of the patients (31.3%; n=5) were obese (BMI>30kg/m2) (Table 1 ). In addition, half of the sample in the baseline had a family history of stroke and 6.3% (n=8) of the subjects had already had at least a previous ischemia.
Table 1 Sociodemographic, lifestyle and health-related characteristics of the participants in the baseline data collection. Curitiba, 2015.
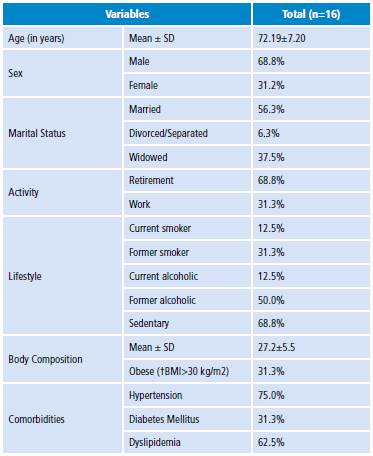
†BMI = body mass index.
Source: Own elaboration based on the data obtained in the study.
Most of the participants suffered the stroke in the left MCA (56.2%; n=9); and the remaining (43.8%; n=7) suffered it in the right MCA. Intravenous thrombolysis was performed in 75% of subjects in the follow-up collection phase.
During the second phase of the study, 13 patients were monitored, of which three died before data were collected. After the stroke, the BMI of the patients decreased, achieving a mean of25.77±5.92 kg/m2.
In terms of frailty, the mean scores increased in all KCL domains from the baseline to the follow-up. However, such differences could be statistically identified in total KCL (p=0.001), IADL (p=0.001), physical domain (p=0.002), socialization domain (p=0.006), and mood domain (p=0.004) (Table 2).
Table 2 Comparison of mean scores in KCL domains between baseline and follow up data collections. Curitiba, 2015.
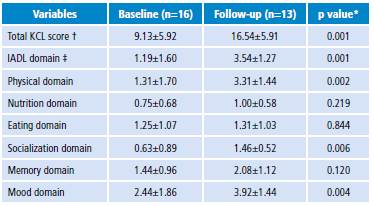
*p<0.05 significant difference. t KCL: Kihon Checklist. t IADL: instrumental activity of daily living.
Source: Own elaboration based on the data obtained in the study.
In agreement with the results presented in Table 2, there were statistical differences in the percentages of frail subjects between baseline and follow-up data collections. The percentage of frail elderly in IADL (p=0.015), physical (p=0.021) and mood (p=0.021) domains were higher after the stroke. Regarding the total KCL score, there was a tendency towards higher values in the follow-up period (p=0.057), while the socialization domain could not be statistically analyzed as all subjects were considered frail (100%) (Table 3).
Table 3 Percentage of frail subjects in baseline and follow-up data collections. Curitiba, 2015.
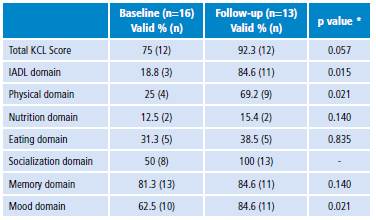
* p<0.05 significant difference.
Source: Own elaboration based on the data obtained in the study.
After conducting a different statistical analysis, the Friedman nonparametric test showed a difference in the frailty condition before and after stroke, suggesting an influence of the stroke on frailty (p<0.001). However, there was evidence of frailty regardless of MCA sides (p=0.050).
The relation between BMI and frailty in the baseline collection could not be observed; however, such association was observed in the follow-up (p<0.049) using the Kendall's test.
The median mRS was 4 (n=16), considering that the scale has a score to be used in death cases. The mRS analysis showed a strong relation with total KCL (p=0.002), indicating an important influence of functional loss on the frailty process.
Finally, the median NIHSS was 5 (n=13) and its relation with total KCL was also significant (p=0.027), correlating the deficits caused by stroke with frailty. As expected, the relationship between the mRS and the NIHSS scales in the follow-up collection phase demonstrates that functional loss is a consequence of the stroke (p=0.026).
Discussion
This study compared frailty conditions in the older adults before and after a stroke. When pairing the total KCL score results of baseline and follow-up data, a significant worsening of frailty in the elderly was found (p=0.001), indicating, as expected, that stroke influences the frailty process.
The initial data of total KCL mean scores (Table 2) demonstrated that the studied population already presented signs of frailty, even before the stroke. It is worth noting that the aging process per se is surrounded by accumulated deficits, mainly in the neuroendocrine, immune and muscular-skeletal systems, that can favor a frailer state 2,3,11,12 and are not necessarily caused by a specific disease or adverse health event such as a fall, a stroke or others. However, when any of these conditions occurs, the recovery process depends on how weakened the organism is. 4,11,13,14
The depletion of physiological mechanisms, caused by frailty, is determinant for coping with acute conditions. This explains the worsening of the total KCL score after the stroke and the increase of frailty percentage in older adults, noting the difficulty of overcoming the deficits caused by the disease. Moreover, a possible negative spiral of losses is observed, as the frail organism is more vulnerable to acute events that, when they occur, worsen even more the frailty process. 3
Regarding the worsening of frailty aspects after the stroke (Table 2), the physical domain showed greater worsening rates, highlighting issues involving strength, balance and physical resistance, which corroborate the fact that the pathology can cause sensorial and motor losses. 5,15 This was reinforced by the significant correlation between the increase of the NIHSS score and the functional loss measured by mRS.
With respect to functional performance, the ability of performing activities was compromised by the neurological event, in agreement with the failure scores obtained in the IADL domain. This suggests that the pathology can influence dependency on external help to perform activities. Previous studies using KCL have shown the correlation between functional loss and cognitive impairment. 16 In consonance with these findings, it is worth mentioning that stroke may compromise cerebral regions which can lead to apraxia. 5 With this in mind, it is possible to conclude that functional decline in stroke patients is strongly dependent on specific clinical characteristics. 17
Regarding the memory and mood domains, alterations before stroke in the baseline phase were observed, which can be explained by neuronal aging combined with low reparative capacity of that cell type. 18 Moreover, these aspects may be connected to a mild cognitive impairment that triggers short-term memory and mood disorders, represented by time disorientation, occasional forgetfulness, lack of interest and emotional lability. 18-20 Additionally, depression rates in the aging population may increase as a consequence of pathophysiological issues related to neurotransmitters, social conditions, psychiatric diseases, psychologic traumas, among other factors. 21
During the follow-up phase, a significant worsening in the mood domain was observed, which may refer to psychological implications associated to the disease. It is estimated that depression can be detected in 20% to 50% of stroke patients 22, as there are related symptoms of sadness, anxiety, tension, lack of interests, among others, due to functional loss, pain, discomfort and cognitive deficits arising from the stroke. 16,23 Some evidence show that people who suffered from a stroke are more prone to memory loss and even to develop vascular dementia. 24,25 In the study, the cognitive alterations were made evident by the higher scores in the memory domain, representing the influence of stroke on the cognitive component of older adults.
It was that 100% of the older adults started to develop socialization issues after the stroke, considering that disabling diseases may limit social participation and, consequently, impose new limitations to their lifestyle. 26 This is evident in the seclusion experienced by these patients after being hospitalized, since they stop leaving their homes. This has consequences in many aspects of their lives -emotionally, professionally and spiritually-, and reduces their social acquaintanceship, which is confined to family and closer friends that pay visits. 27
Regarding nutrition, the mean score increased from the baseline to follow-up phases, but is not statistically relevant. Nevertheless, differences in body composition measured by BMI were observed. The index decreased between data collections, although the sample was still considered overweight after the stroke. In relation to the eating domain, an increase in the mean score between both moments was also observed, although they were not statistically different; the percentage of subjects with oral dysfunction was similar before and after stroke.
Based on this study, it is possible to state that the deficits caused by a stroke let the sample even frailer and, in consequence, the studied elderly became more susceptible to adverse events such as functional dependence, falls, hospitalizations, institutionalizations and even death. 3,28 For the purpose of assessing frailty before and after stroke, the KCL seems to be an effective tool, as it allows a brief analysis of the main aspects of frailty and can be easily applied. 9,16Thus, this study emphasizes that frailty screening, as part of the procedures offered by Stroke Units, can be beneficial for both the elderly patients and for the health team as it may guide multidisciplinary intervention, taking care of the main impaired domains of KCL, especially those with more problems before the stroke. Such improvement in opinion and treatment would reinforce comprehensive care to support frailty in older people. 29,30
This study has some limitations, including the small sample size; some patients did not return for the neurological appointment and did not participate of the follow-up study; additionally, it was performed in only one institution. Future studies conducted to find associations between frailty and stroke should have a greater sample size from different institutions.
Conclusion
This research confirmed the influence of stroke on frailty in elderly patients. Moreover, it demonstrates the importance of assessing frailty to improve treatment in stroke patients. Each KCL domain is valid to detect the increase of frailty associated with stroke, as well as to predict the aspects of the disease that may pose major challenges to the patients' recovery and assist the actions of multidisciplinary teams.

