











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Loss of muscle strength (dynapenia)1 has a negative impact on morbidity and mortality.2 Therefore, the timely assessment of muscle strength is fundamental in preventive medicine.3
The handgrip strength test is a validated and simple test used to assess muscle strength in several health-related contexts.4-10 Despite its importance in clinical practice, there is a wide range of equipment and protocols to measure maximal handgrip strength (MHS).11 Particularly, the effects of warming-up before performing MHS tests have not been described yet.
A warm-up is generally intended to generate an increase in muscle temperature, facilitating increased blood flow, optimizing metabolic responses,12,13 reducing muscle viscosity (i.e. smoother contraction), and increasing nerve conduction velocity.14 By extension, the search for an optimal muscle temperature range that limits fatigue as much as possible whilst maximizing performance12-15 seems prudent. Commonly, warm-up protocols tend to reflect the experience of individual researchers and practitioners, and most studies are performed in athletes.16
Controlled studies about the effects of warm-up on maximal performance are particularly scarce, maybe due to the unwillingness of voluntary subjects to complete a maximal effort without warm-up (i.e. control condition). However, among the studies investigating the effect of warm-up protocols on muscle performance (e.g., maximal strength), conflicting results have arisen and some of them show an increase in performance after general, specific,17 or combined warm-up,18 while others have not.16
Considering the lack of studies addressing the effects of warm-up on sedentary overweight women and MHS, as well as the clinical relevance of MHS in community-health programs,19 a standardized protocol of application is required. The aim of this study was to compare the acute effects of different warm-up strategies on MHS in sedentary women since it has been suggested that different warm-up protocols may have an impact on MHS.
Materials and methods
Ethical considerations
This study (study protocol No. 103- 2018) was approved by the Institutional Review Board of the Department of Physical Activity Sciences, Universidad de Los Lagos, as stated in Minutes DECAF2016/3, issued on April 25, 2016. The participants who agreed to take part in the study signed an informed consent form, after being explained about the risks and benefits derived from their participation. The study was conducted according to the ethical principles for medical research involving human subjects established in the Declaration of Helsinki 2013.20
Subjects and procedures
A public call was made in a local University to recruit sedentary overweight women willing to participate in a randomized single-blind crossover study. A total of 12 women were recruited (age: 21.1±2.0 years; fat mass: 38.1%±8.4%; see Table 1 for more characteristics), and completed four different measurement protocols to assess MHS, with 48h of rest between each.
Table 1 Baseline characteristics of the sample.
| Variables | Mean | σ |
|---|---|---|
| Body mass (kg) | 64.5 | 9.1 |
| Height (m) | 158.3 | 8.4 |
| Body mass index (kg/m2) | 26.3 | 3.9 |
| Body fat (kg) | 24.8 | 7.3 |
| Lean mass (kg) | 22.1 | 3.3 |
| Water (L) | 29.8 | 4.0 |
| Lean mass left hand (kg) | 2.1 | 0.4 |
| Lean mass right hand (kg) | 2.1 | 0.4 |
| Fat mass left hand (kg) | 1.8 | 0.7 |
| Fat mass left hand (kg) | 1.8 | 0.7 |
σ: standard deviation.
Source: Own elaboration.
To be included in the study, participants were required to: i) be over 18 years old, ii) be sedentary (weekly physical activity level = 600 MET-min/week),21 iii) be free of cardiovascular, pulmonary or skeletal muscle diseases,22 and iv) have fat mass >30% of total body mass. All experimental procedures were performed under controlled and standardized conditions in the Laboratory of Human Performance at the university where the study was conducted, always at the same time of day, with the same temperature, humidity, rest time (i.e., sleep hours before testing), menstrual cycle phase, and hours after the last meal. According to previous recommendations, height (Bodymeter 206, SECA, Germany to 0.1cm), body mass and body composition (InBody120, tetrapolar 8-point tactile electrodes system, model BPM040S12F07, Bio-space, Inc., USA, to 0.1kg) were measured.23
Measurement of handgrip strength
The test was applied according to previous recommendations.24 To assess MHS, an adjustable digital dynamometer was used (Jamar®, PLUS+, Sammons Preston, Patterson Medical, Illinois, United States). After randomly assigning the order of dominant and non-dominant hand assessment, three trials were performed to achieve maximal voluntary isometric handgrip strength (MVIHS) for both dominant and non-dominant hands, with 2 minutes of rest between trials.
For each trial, subjects were asked to exert 5 seconds of maximal effort, while receiving standardized verbal motivation. Subjects completed each trial while sitting up straight on a chair. The hip, knee, and elbow were flexed to a 90° angle and the shoulder was abducted and neutrally rotated. The forearm was in a neutral position and the wrist was slightly extended (0° to 30°). Subjects performed the test with a horizontal cylinder using the digital grip dynamometer in position 2, while the evaluator lightly held its base. The best result (in kg) of the three trials for each hand was chosen for statistical analysis.
Warm-up protocols
Four randomly selected warm-up protocols (Table 2) were applied for the forearm muscles of both the dominant and non-dominant hands as follow: i) no warm-up (control condition), during which subjects remained seated comfortably for three minutes before testing; ii) static stretching warm-up, in which subjects carried out static stretching of the forearms flexors and extensors muscles for a total of 5 sets of 5 seconds each;25 iii) strength (i.e. elastic band-based) warm-up, during which subjects completed two sets of 10 repetitions for the forearm flexor muscles for a duration of 2.5 sec-ondsforeach contraction26 using an elastic band (THERA Band™; medium intensity, blue color) and 30 seconds to 1 minute of rest between sets; and iv) isometric therapeutic squeezing-ball warm-up, during which subjects completed 1 grip per 2.5 seconds (for a total of 20 repetitions) on a therapeutic squeeze ball.27 The Borg Rating of Perceived Exertion was used to measure intensity during warm-ups to standardize it across all conditions, always with a score between 3 and 6 points. After the warm-ups, 3 minutes elapsed before testing MHS.
Table 2 Characteristics of the warm-up protocols.
| Warm up | Exercises | Sets | Repetitions | Rest between sets | Rest after warm-up |
|---|---|---|---|---|---|
| No warm-up | - | - | - | - | - |
| Static stretching | Static flexion of wrist | 5 | 5 seconds | 30 seconds | 3 minutes |
| Static extension of wrist | 5 | 5 seconds | 30 seconds | ||
| Elastic band | Dynamic flexion of wrist | 2 | 10 | 30 seconds | 3 minutes |
| Isometric therapeutic squeezing-ball | Squeeze and release | 1 | 20 | 30 seconds | 3 minutes |
Source: Own elaboration.
Statistical analysis
All values are reported using means and their corresponding standard deviations. The Shapiro-Wilk and Levene's tests yielded non-significant values for all data. To determine the effects of the conditions on MHS, absolute mean differences between conditions were compared using a repeated measures analysis of variance, with Fisher post hoc procedures. The a level was set at p<0.05 for statistical significance, with Cohen's d representing effect size (ES) interpreted as <0.2=trivial; 0.2-0.6=small; >0.6-1.2=moderate; >1.2-2.0= large; >2.0-4.0 = very large; >4.0=extremely large).
The reliability of the assessments was determined using the intra-class correlation coefficient. All measurements yield values >0.9.
Results
The MHS mean values for the non-dominant and dominant hand were 23.8kg and 24.9kg after no warm-up, 20.3kg and 21.4kg after the stretching warm-up, 20.9kg and 22.9kg after the strength warm-up, and 22.0kg and 23.0kg afterthe squeezing-ball warm-up, respectively (Figure 1). No significant differences (p>0.05; ES<0.2) were observed among warm-up protocols.
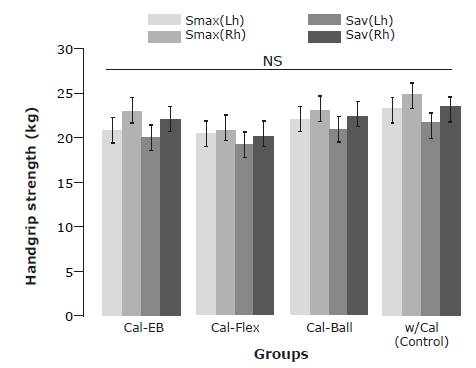
* Sav: mean maximal strength values from three measurement trials. † Smax: Denotes maximal strength value from three measurement trials. ‡ NS: non-significant differences within-groups and between groups. Source: Own elaboration.
Figure 1 Maximal handgrip strength of dominant and non-dominant hands in obese sedentary women after no warm-up, stretching warm-up, strength warm-up, and squeezing-ball warm-up. Lh: left hand; Rh: right hand; Cal-EB: strength warm-up; Cal-Flex: stretching warm-up; Cal-Ball: squeezing-ball warm-up; w/Cal: no warm-up.
Regarding the maximal strength value obtained from the 3 MHS trials (Smax in Figure 1) and the mean strength value obtained from the 3 MHS trials (Sav in Figure 1), no significant differences were observed between values (p>0.05; ES<0.2).
Discussion
The aim of this study was to compare the effects of different warm-up protocols on MHS. The main findings suggest that the 3 randomly selected warm-up protocols had no effect on MHS in a sample of 12 sedentary overweight women. Moreover, a reduced MHS trend was observed in the participants after performing a static stretching-based warm-up.
Regarding static stretching in warm-up routines, Behm etal.,28 in a study about the effects of static stretching warm-up on the strength of quadriceps muscles, reported a significant 12% maximal isometric strength decrease. Similar results have also been described for the pectoralis major and the triceps brachii muscles.29 In this sense, the results reported in the present study are in agreement with the aforementioned findings28,29 since static stretching of forearm flexor and extensor muscles, regardless of hand dominance, negatively affected MHS in sedentary overweight women. Several factors may help to explain the impairment in MHS after static stretching, such as alterations in the mechanical components of muscle contraction,30 decreased muscle activation,28 or both.30
In the current study, compared to the control condition, there were no improvements in MHS after the warm-up with elastic band. This finding is contrary to the results of a study conducted by Tilley & Macfarlane,31 where an increase in swing performance was demonstrated in elite male golfers after a warm-up with a rubber band. In male judokas, a warm-up with an elastic band allowed them to improve performance in the jerk test when compared to a control condition.32 Moreover, Mina et al. ,33 observed an increase in maximal squat strength in men after a warm up with an elastic band. In addition, in a study conducted by Aandahl et al.34 an increase in the maximal kick speed in martial arts fighters was observed leading the authors to conclude that this increase was due to greater recruitment of higher order motor units, greater synchronization of the motor units and low presynaptic inhibition.
However, the performance-enhancing factors observed in previous studies31-34 were found in athletes, not in a sedentary population as in the present study. Notably, the aforementioned studies31-34 usually analyzed the effect of elastic band warm-ups on large muscle groups in multi-joint exercises, which differ from the muscle groups analyzed in our study. Therefore, these methodological elements (i.e., sedentary vs. athletes; small muscle group vs. large muscle group; single-joint vs. multi-joint) could help explain the difference between the results found in this work and those previously published.31-34
Current results show that the specific warm-up with a therapeutic ball (squeezing-ball warm-up) had no effect on MHS when compared to the control condition. A specific warm-up involves skill exercises that demonstrate equivalency with the targeted motor task.35 It seeks to increase performance36 via increases in muscle temperature, reductions in muscle viscosity and greater nerve conduction velocity.14 In a study conducted by Andrade et al.,37 the effects of a general warm-up, a specific warm-up and a combined warm-up on explosive muscle performance were compared, finding improvements in squat jump and drop jump after a specific jump-based warm-up. Similarly, in a study conducted in volleyball players, an improvement in countermovement vertical jump was observed after a specific warm-up protocol based on jump exercises.38
It is worth noting that the improvements in jumping performance after specific jump-based warm-ups were observed in large muscle groups. Smaller muscles, such as the forearm, are composed of a significant number of slow-twitch muscle fibers that require a low motor unit firing frequency (i.e., 5 to 30Hz), unlike other larger muscle groups.39 Such slow-twitch fibers are easily excitable40 and so require lower levels of stimulation to achieve maximal activation and, therefore, maximal strength. Consequently, as forearm muscle activation in hand-grip tasks is relatively easier41 compared to larger muscle groups, a specific warm-up may not add to the performance of such muscle group during hand-grip tasks.
It should be stressed that no differences were observed in MHS after dynamic (elastic band) and isometric (static stretching; isometric therapeutic squeezing-ball) warm-up protocols. Such observation seems to be contrary to the findings of a previous study,42 where a dynamic warm up, when compared to static-stretching warm up, improved power and agility (T-shuttle run, medicine-ball underhand throw for distance, and 5-step jump) in male and female military cadets. However, the methodological differences between the studies, such as the participant's characteristics (females vs. mix sample of male and females), physical fitness level (low vs. high), type of performance test (maximal isometric strength vs. dynamic power test), among others, should be considered.
In this regard, the American College of Sport Medicine indicated that more controlled studies are needed to substantiate the effectiveness of warm-up protocols.43 The lack of consensus may be partially related to the different methodological issues previously reported, as the effect of warm-up may vary according to such aspects.13 Moreover, most studies on warm-up strategies have been conducted in athletes.13 In this sense, the present results expand the limited knowledge available about the effect of different warm-up protocols on the MHS of sedentary overweight women.
Limitations, strengths, and practical applications
A limitation of the study was its sample size, as it may not have allowed obtaining statistically significant findings. Future studies should aim to replicate the current findings with a greater sample size. Additionally, to better understand the underlying mechanisms of different warm-up protocols, future research should include bio-mechanical as well as physiological measures related to the responses of forearm muscles to different warm-up protocols in sedentary overweight women.
Conclusion
Warm-up of the forearm muscles does not acutely increase isometric MHS in sedentary overweight women in the dominant, or the non-dominant hands. Three isometric trials, without warm-up, allows achieving MHS with high reliability, serving as a time-efficient measurement protocol with high applicability in clinical practice.

