











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
Permalink
Introduction
Urinary tract infection (UTI) is the most frequent medical complication in pregnant women,1 with a prevalence between 14% and 48%.2-4 The high number of cases of this infection during pregnancy is associated with physiological and physical changes that increase the risk for its onset, such as glycosuria and alkaline urine pH; increased kidney size and glomerular filtration rate; dilation of the urinary tract due to decreased ureteral peristalsis secondary to the effect of progesterone; and progressive mechanical obstruction of the gravid uterus.5,6
UTI is defined as bacterial invasion, colonization, and proliferation of the urinary tract; these bacteria may migrate from the bladder to the renal parenchyma.7 Its clinical presentation includes asymptomatic bacteriuria and acute pyelonephritis.8 This infection is diagnosed based on clinical manifestations and the urine culture report with specific parameters for each type of UTI.
The microorganisms most frequently related to UTIs come from the perineal flora, finding that enterobacteria such as Klebsiella spp, Proteus mirabilis and Escherichia coli cause 95% of the cases,7 with the latter being the most common pathogen (70-80%).6,9 Bacterial resistance in these microorganisms varies according to the population studied and the type of antibiotic used for treatment, with ampicillin resistance occurring in 82% of E. coli infections and in up to 100% of Klebsiella spp and Pseudomona aeruginosa infections.9,10
Several studies have found that the most common risk factors for developing UTI during pregnancy are multiparity, low socioeconomic status, previous history of UTI before pregnancy, sexual activity during pregnancy, structural and functional alterations of the urinary tract, sickle cell anemia, diabetes, bacterial vaginosis, and being a teenage mother.1,6,8
UTIs during pregnancy can lead to serious maternal and fetal complications. Therefore, these infections in pregnant women, including asymptomatic bacteriuria, must be treated.5 It should be noted that untreated asymptomatic bacteriuria has a 20-30% chance of causing pyelonephritis,5 and, in turn, it is associated with negative outcomes such as increased incidence of preterm birth, low birth weight, anemia and respiratory distress in the newborn, increased risk of fetal and amniotic infection, and increased systemic fetal involvement due to maternal infections.5-7
There are several methods available to diagnose UTI, with urine culture being the gold standard. In Colombia, it is one of the routine compulsory tests that all women enrolled in the antenatal care (ANC) program for the first time must undergo. The recommendation is to perform it between weeks 12 and 16 of pregnancy and repeat it depending on the needs or conditions of the pregnant woman.11 The cost of urine culture is included in the health insurance plans available in the country, regardless of the type of enrollment of the mother (subsidized or contributory).
In Bucaramanga, access and quality of care of the ANC program have been prioritized based on the primary health care (APS in Spanish) model implemented by the Health and Environment Office of Bucaramanga and the Bucaramanga Health Institute, a Social Enterprise of the State (ESE-ISABU) since 2009. Consequently, urine cultures should be performed in 100% of users during their first ANC appointment within the framework of this model. ESE-ISABU is a municipal health service provider that provides primary care services to about 40% of the city's population. This group of beneficiaries is predominantly from the socioeconomic strata 1 and 2 according to the classification of the National Administrative Department of Statistics (DANE) (Table 1).
Table 1 Socio-economic strata in Colombia according to the National Administrative Department of Statistics.
| Stratum | Description |
|---|---|
| 1 | Low-Low: Beneficiaries of home utility subsidies. |
| 2 | Low: Beneficiaries of home utility subsidies. |
| 3 | Middle-low: Beneficiaries of home utility subsidies. |
| 4 | Middle: They are not beneficiaries of subsidies, nor do they pay surcharges; they pay exactly the amount that the company defines as the cost for providing home utilities. |
| 5 | Middle-high: They pay surcharges (contribution) on the value of home utilities. |
| 6 | High: They pay surcharges (contribution) on the value of home utilities. |
Source: Elaboration based on the data by National Administrative Department of Statistics.12
The literature review carried out for this research found that there are few studies in Colombia on the prevalence and pharmacological treatment of UTIs in pregnant women, and only one publication addressed covariate-adjusted risk factors.13 The scarce literature on this topic reported that the prevalence of UTI in pregnant women attending ANC was 10.5% in Bucaramanga, Santander;14 36.1% in Manizales, Caldas;15 and 48% in Soledad, Atlántico.4
Among the studies conducted in Colombia, it was found that López Martínez et al.16 studied pyelonephritis in pregnant women with an incidence of 1.8 cases per 1 000 births, establishing being adolescent, first pregnancy and having had UTI before pregnancy as associated factors. Also, Maldonado et al.17 reported a prevalence of asymptomatic bacteriuria of 7-9% in pregnant women between 12 and 16 weeks of gestation; in turn, Campo-Urbina et al.18 found the same condition in 10.6% of pregnant women evaluated in their study of pregnant women from 35 to 37 weeks. Finally, Torrejano et al.13 reported a higher prevalence of UTIs in mothers with low-education, multiparous, and late ANC enrollment, although these estimates were not statistically significant.12
Given this panorama and the scarce information available locally and regionally on UTIs, and considering that research shows that this type of infection is more frequent in populations of low socioeconomic levels, the objectives of this study were to determine the prevalence of UTI in socially vulnerable pregnant women in Bucaramanga, to characterize UTI cases, and to identify the factors associated with the development of this complication and the antibiotic resistance profile of the microorganisms that cause the infection.
Materials and methods
Design and study population
The data obtained in the main study entitled "Technical efficiency of women's health prevention programs in Bucaramanga, Colombia: A four-stage analysis," authored by Ruíz-Rodríguez et al.,19 was subjected to a secondary analysis.
Said research followed a cross-sectional analytical observational design and was carried out between 2013 and 2014. The sampling frame was made up of the medical records of all pregnant women (n=2 932) who attended at least one ANC appointment between January 1 and December 31, 2012, at one of the 21 public primary care centers of the ESE-ISABU. Records of multiple pregnancies were excluded.
In the primary study, the sample was selected by simple random sampling using a random number table that was generated with Stata 12. Between 16 and 60 medical records were selected in each health center proportionally to the total number of pregnant women treated in each institution in 2012.
Furthermore, in the primary study, a checklist was designed to extract information concerning sociodemographic and obstetric data from the medical records, as well as anthropometric measurements, laboratory reports, diagnosis, and therapeutic plan for UTI. This checklist was drawn up taking into account the structure of the medical record form used in the health centers attached to the ESE-ISABU and with the support of medical and nursing staff with experience in ANC. A pilot test to standardize data collection was carried out when the instrument was ready. For more information on the methodology and the context of the study, see Ruiz-Rodríguez et al.19
The total sample included in the primary study (n=838) was analyzed in the present study; however, it should be noted that this sample size was not the same for all variables due to the lack of complete information from the medical records in some cases.
Variables
The dependent variable was the diagnosis of UTI by means of urine culture, in which a count >105 colony-forming units per milliliter was required. Independent variables included age (completed years), educational attainment (last year approved), paid occupation (yes/no), living with the partner (yes/no), and socioeconomic stratum reported in the medical record according to the DANE classification12 (Table 1). Due to the low proportion of pregnant women in strata 3, 4, 5 and 6, they were grouped and a variable of three categories was created (1, 2 and 3-6).
Independent variables also included pre-pregnancy body mass index (BMI), categorized as underweight, normal weight, and overweight according to the World Health Organization cut-off points;20 parity (yes/no); history of UTI (yes/no); gestational age at diagnosis of UTI (trimester); number of ANC visits attended (1-4 and >4); diagnosis of diabetes (yes/no) or vaginosis (yes/no) during pregnancy; and diagnosis of medium or high obstetric risk during the first ANC visit (yes/no), based on the information reported in the medical history by the physician and recorded in the administrative care area to which the health center belonged (north, west, east and south) and where each patient was treated.
Statistical analysis
A descriptive analysis of the characteristics of pregnant women was made using measures of central tendency and dispersion for continuous variables, and frequency tables for categorical variables. The prevalence of UTI was estimated based on the proportion of pregnant women with a UTI diagnosis report in their medical record and on the result of the urine culture test (n=648).
In addition, a bivariate analysis was performed to evaluate differences in the diagnosis of UTI according to the independent variables, using the Mann-Whitney U and chi-squared tests for continuous and categorical independent variables, respectively. A multivariate analysis was performed using a binomial logistic regression model, calculating prevalence ratios (PR) with a 95% CI to establish factors associated with gestational UTI.
Finally, following Greenland's recommendations,21 variables that showed p-values <0.20 for the bivariate analysis were included in the regression model; in addition, other variables that the authors considered relevant based on what was found in the literature review were included. Taking the above into account, the final model was adjusted for age, educational attainment, paid occupation, BMI, history of UTI, gestational age, diagnosis of gestational diabetes, vaginosis, obstetric risk during pregnancy and administrative area in which patients were treated.
Ethical considerations
The present research complied with the ethical principles for medical research on human beings established by the Declaration of Helsinki.22 According to the provisions on health research in Resolution 8430 of 1993 of the Ministry of Health of Colombia,23 the present study is considered a risk-free research as retrospective techniques and methods for reviewing medical records were utilized and no intervention or intentional modification of the biological, physiological, psychological or social variables of the participants was performed. Moreover, the study was endorsed by the Ethics Committee of the Bucaramanga Health Institute as stated in Minutes No. 02851 of June 8,2011.
In order to respect the right to the integrity and confidentiality of the information obtained, each medical record was assigned an individual code for identification.
Results
Characteristics of the study population
The medical records of 838 pregnant women enrolled in ANC programs at 21 primary care centers of Bucaramanga affiliated with ESE-ISABU were reviewed. The median age of participants was 22 years (IQR=19-27), and the median years of schooling was 9 years (IQR=6-11). 32.29% of pregnant women had a paid occupation. Only 803 pregnant women (95.82%) had at least one urine culture requested during their ANC appointment and the result was recorded in the medical record of 648 (77.32%) of them. Similarly, of the total number of pregnant women analyzed (n = 838), 20 (2.38%) had a history of UTI and 145 (17.30%) were diagnosed with vaginosis during pregnancy (Table 2).
Table 2 History and sociodemographic, anthropometric, and clinical characteristics of pregnant women attending antenatal care programs in Bucaramanga, Colombia.
| Characteristics | n | % | ||
|---|---|---|---|---|
| Sociodemographic | Age (years) (x, IQR) (n=838) | 22 | (19-27) | |
| Education (years) (x, IQR) (n=767) | 9 | (6-11) | ||
| Paid Occupation (n=836) | 270 | 32.29 | ||
| Living with the partner (n=821) | 637 | 77.58 | ||
| Socioeconomic stratum (n=828) | 329 | 39.73 | 39.73 | |
| 309 | 37.31 | 37.31 | ||
| 190 | 22.94 | 22.94 | ||
| Anthropometric | BMI (n=816) | 65 | 7.96 | 7.96 |
| 476 | 58.33 | 58.33 | ||
| 275 | 33.70 | 33.70 | ||
| History | Parity (n=835) | 330 | 39.52 | |
| ITU (n=838) | 20 | 2.38 | ||
| Clinical | Gestational age at UTI diagnosis (trimester) (n=673) | 336 | 49.92 | 49.92 |
| 298 | 44.27 | 44.27 | ||
| 39 | 5.79 | 5.79 | ||
| More than 4 ANC visits (n=838) | 457 | 54.53 | ||
| Diagnosis of diabetes during pregnancy (n=838) | 23 | 2.74 | ||
| Diagnosis of vaginosis during pregnancy (n=838) | 145 | 17.30 | ||
| Diagnosis of UTI during pregnancy (n=648) | 94 | 14.50 | ||
| Diagnosis of medium or high obstetric risk in the first ANC (n=755) | 427 | 56.55 | ||
| Administrative area of the care center (n=838) | North | 250 | 29.83 | |
| West | 229 | 27.32 | ||
| East | 166 | 19.80 | ||
| South | 193 | 23.03 | ||
BMI: body mass index; UTI: urinary tract infection; ANC: antenatal care visit.
Source: Own elaboration.
Figure 1 shows the distribution of urine culture results. Of the total number of pregnant women (n=838), 1.19% (n=10) had a diagnosis of UTI recorded by the physician in their medical records, but no urine culture results were found to support this diagnosis. Also, the results of urine culture were not recorded in the medical history of 19.30% (n=155) of those who underwent this test (n=803).
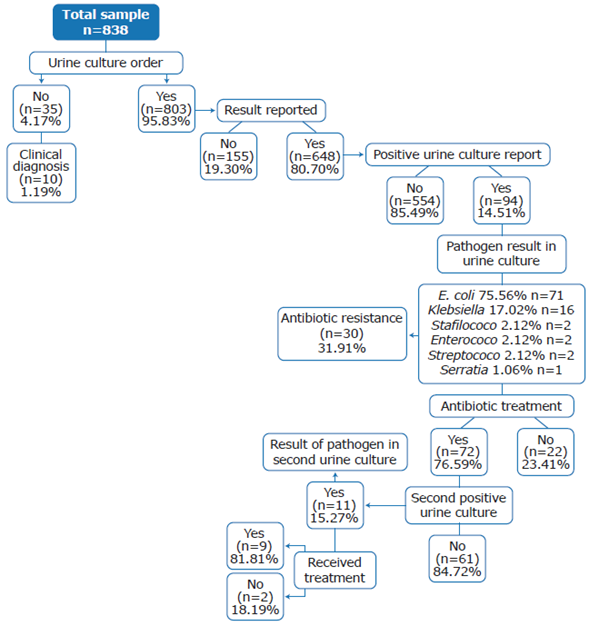
In the medical records that reported a urine culture (n=648), it was identified that the prevalence of UTI was 14.50% (n=94), and that this infection was caused by E. coli (75.53%), Klebsiella spp (17.02%), staphylococcus (2.13%), enterococcus (2.13%), streptococcus (2.13%), and Serratia (1.06%).
Antibiogram was requested to 31.91% (n=30) of pregnant women with UTI and, based on the results, it was found that the most common antibiotic resistance was against trimethoprim/sulfamethoxazole (26.92%), followed by nitrofurantoin (19.23%), cephalosporins (11.54%), ampicillin/sulbactam (7.69%), and ampicillin (3.85%). Moreover, resistance to trimethoprim/ sulfamethoxazole (31.25%) and nitrofurantoin (40%) was the most frequent in E. coli and Klebsiella cases, respectively (Table 3). There was also only one report of antibiotic resistance to trimethropim/sulfamethoxazole in staphylococci and to nitrofurantoin in enterococci. 76.59% of women diagnosed with UTI received antibiotic treatment with nitrofurantoin (30.93%), ampicillin (20.62%), cephalexin (20.62%), and amoxicillin (9.28%), which were the most used drugs.
Table 3 Antibiotic resistance profiles according to isolated germs.
| Organism | Trimethoprim/ sulfamethoxazole (%) | Nitrofurantoin (%) | Cephalosporins (%) | Ampicillin/ sulbactam (%) | Others |
|---|---|---|---|---|---|
| E. coli | 31.25 | 6.25 | 12.50 | 6.25 | 43.75 |
| Klebsiella | 0.00 | 40.00 | 20.00 | 20.00 | 20.00 |
Source: Own elaboration.
The bivariate analysis found that pregnant women with UTIs were of a median age, lower than in those who did not have such a diagnosis (21 vs. 22.50); in contrast, no statistically significant differences were observed regarding the other sociodemographic, anthropometric, or clinical variables, nor regarding the health history and the administrative area of the care center (Table 4).
Table 4 Sociodemographic, anthropometric, and clinical characteristics and history of pregnant women with a diagnosis of urinary tract infection based on urine culture.
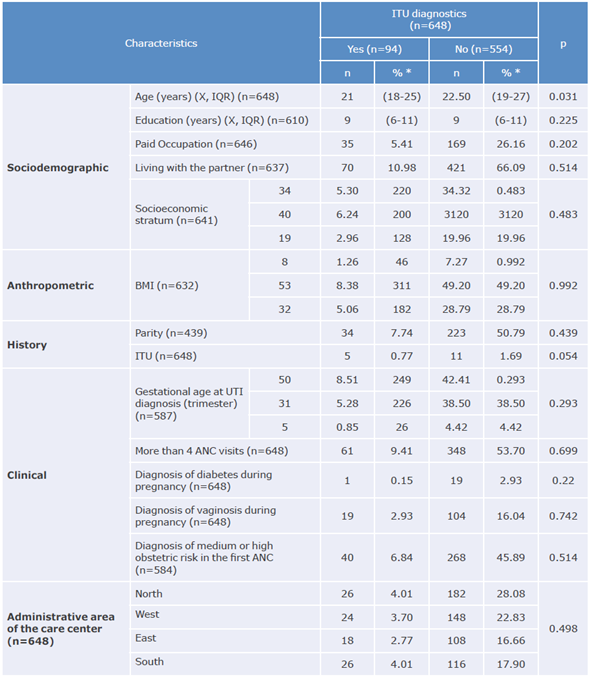
BMI: body mass index; UTI: urinary tract infection; ANC: antenatal care visit.
* Percentages were estimated based on the total n reported in the left column for each variable.
Source: Own elaboration.
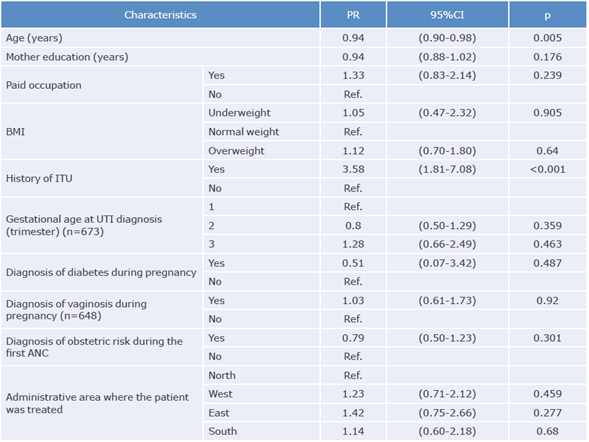
On the other hand, multivariate analysis showed that a history of UTI before pregnancy was positively associated with the diagnosis of UTI during pregnancy (PR: 3.58, 95%CI: 1.81-7.08; p<0.001) and that, in contrast, for each year of maternal age increase there was a 6% reduction in the prevalence of UTI (PR: 0.94, 95%CI: 0.90-0.98; p=0.005) (Table 5).
Discussion
UTIs are the most frequent complications during pregnancy and affect mainly socially vulnerable pregnant women. To the authors' knowledge, this is the first study in Colombia that characterizes UTI (both in terms of prevalence and the most frequent uropathogens and their treatment with antibiotics) in low-income pregnant women treated in a primary care center focused on the APS strategy.
Although urine culture is a mandatory and free test according to the Colombian regulations, the present study found that it was not requested in 4.17% of the participants and that no report of the results was found in the medical records of 19.30% of the pregnant women to whom it was ordered (n=803). In this regard, studies in other contexts show that lack of knowledge of clinical practice guidelines among health professionals can affect compliance with such guidelines,24 which, in turn, may explain why the necessary procedures are not always performed.
The results of this study showed a prevalence of UTI of 14.50%, which was lower than that reported in other studies developed in Colombian cities, in which percentages of 10.5%,14 36.1%15 and 48% were found,4 taking into account that those studies were also carried out in institutions of the first level of care. The low prevalence reported here could be related to the APS approach used in the primary care units of the ESE-ISABU or to a potential bias in the selection of the study population since most pregnant women included were of low socioeconomic status and belonged to subsidized health care scheme.
E. coli (75.53%) and Klebsiella spp (17.02%) were the most frequently isolated uropathogens, which agrees with Gessese et al.,25 who conducted a study in an Ethiopian population with characteristics similar to those of the present research, finding that of 56 positive urine cultures, E. coli was the most common pathogen causing UTI during pregnancy (46.4%), followed by Staphylococcus aureus (14.3%).
Likewise, Hamdan et al.2, in Sudan, found that E. coli and Staphylococcus aureus are the main etiological agents of UTIs during pregnancy with 42.4% and 39.3% of cases, respectively. In contrast, Sheik et al.3 found that staphylococcus species were more common than E. coli in Pakistan. In addition, other studies indicated that Klebsiella spp is associated with very few cases of UTIs.2,3,25
In Colombia, other studies had already reported E. coli as the most frequent positive uropathogen responsible for UTI in the urine cultures of pregnant women, with percentages ranging from 44% to 89%,9,10,16 and that it is followed by Klebsiella spp species, with frequencies between 11% and 22%,9,10 which coincides with the findings of this study.
It should be noted that UTI due to enteropathogenic bacteria is related to several factors, including inadequate urinary habits.26 Therefore, it is of great importance that, in both general medicine and ANC consultations -as recommended in the Comprehensive Care Route for the Promotion and Maintenance of Health and the Comprehensive Health Care Route for the Maternal and Perinatal Population, regulated by Resolution 3280 of 2018 of the Ministry of Health and Social Protection27-, pregnant women should receive information about adequate urinary habits and perineal hygiene practices, which are mechanisms for preventing colonization of the urinary tract by this type of bacteria. It is also important to train medical staff to adequately provide these instructions during the consultation.
As for treatment, despite the consensus that all UTIs in pregnancy trigger adverse events for maternal-fetal health7 and should, therefore, be treated,5, it was found that 23.40% of pregnant women included in the present study who had a positive urine culture report for UTI did not have any type of treatment reported in their medical records. This may be due to the prioritization of other health conditions of pregnant women by medical professionals or to failures in the medical records.
The most prescribed antibiotics to treat UTI in the participants were nitrofurantoin and ampicillin (30.93% and 20.62%, respectively), which are among those recommended by guidelines for UTI management of the Colombian Association of Infectious Diseases.7 These findings show that ANC physicians at ESE-ISABU know and follow the antibiotic management schemes indicated by the national guidelines. However, it is necessary to continuously update the processes related to the treatment of common diseases of pregnant women because recent studies recommend avoiding treatment with nitrofurantoin and trimethoprim/sulfamethoxazole in the first trimester of pregnancy.28
Although antibiogram studies were performed in only 31.91% of the population with positive urine cultures for UTI included in the study, these results are important for determining the resistance profile in low-income populations in Bucaramanga. Thus, it was found that most UTI cases showed resistance to nitrofurantoin, which was not effective in 40% of Klebsiella infections, contrasting with previous studies that showed that ampicillin-resistant E. coli.3,25 was more frequent (57-73%).3,9,25 Also, a study conducted in Colombia in nine hospitals reported high resistance to ampicillin in 42.2% of E. coli infections and in 57.1% of Klebsiella spp infections.
In the present study, only clinical and demographic factors were associated with the frequency of UTI in the study population. On the one hand, the history of pregestational UTI was positively associated with a diagnosis of UTI during pregnancy with the greatest strength of association (PR: 3.58, 95%CI: 1.81-7.08, p<0.001). This result is consistent with what was reported in a review on the topic 6 as well as in original studies conducted in Ethiopia,25 Pakistan29 and four major cities of Colombia.15However, other studies, such as those carried out in Sudan2 and Pitalito, Colombia,12 did not find that association, which may be explained by the fact that their study populations were hospitalized, and the socioeconomic level variable was not included in the analysis.
Furthermore, it was observed that the prevalence of UTI during pregnancy dropped by 6% for each year that maternal age increased, (PR: 0.94, 95%CI: 0.90-0.98; p=0.005), which is consistent with López-Martínez et al.15, who found a significant association between UTI and age (p=0.008) after observing that being a teenager increased the likelihood of developing an infection of this type since the average age of patients with this infection was 21.97 years and the average age of those who did not have it was 22.78 years. However, this finding differs from other international studies in which age was not associated with UTI.25,30,31 This difference can be explained because the environmental characteristics of the populations studied are different and because international research included variables such as meat consumption and hygiene, which were not considered in the present study. The fact that age was negatively associated with UTI is a relevant finding because it suggests the need to implement strategies that delay pregnancy intention in very young women.
Some of the strengths of this study that must be stressed are the representativeness of the primary care public service network in Bucaramanga, the random sampling of medical records proportional to the number of pregnant women enrolled in ANC programs in each health center, and the collection of data made by professionals with experience in health promotion and disease prevention programs, who were trained in a checklist adjusted for that purpose.
Conversely, one of the main limitations of the study, and in general of secondary analyzes derived from medical records, is that there is a potential bias of classification due to the underreporting of data, which could affect the estimates obtained here. Although it was not possible to control this bias given the nature of the study (review of information already registered in the medical records), an attempt was made to minimize it by training the data collection team to perform a thorough review of the records and extract data carefully. Finally, since this is an observational study, there was also a potential confounding bias; in this regard, an attempt to control it was made by performing a multivariate analysis, which was adjusted for potential confounding variables.
Conclusions
Even though, according to Colombian regulations currently in force, treatment of UTI should be a priority in pregnant women, its prevalence in the study population was almost 15%. This situation shows the need to implement education strategies on urinary habits and perineal hygiene directed to pregnant women, mainly to the younger ones and those with a history of UTI, to prevent its onset during pregnancy and the possible consequences for maternal and fetal health. Additionally, once UTI occurs during pregnancy, it is essential to quickly identify the pathogens involved and establish the antibiotic resistance profile to provide timely care and prevent complications.
This study also provides information on compliance with maternal care guidelines and antibiotic regimen schemes used to treat UTIs during pregnancy by general practitioners. Therefore, the data reported here may help develop public policies to improve the prevention and care of this disease in similar populations.

