











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Patellofemoral pain syndrome (PFPS) is one of the most common musculoskeletal disorders. It causes pain in the front of the knee and usually affects young adults.1-4 PFPS accounts for 11% to 17% of all knee pain cases, and its prevalence in physically active adolescents and adults ranges from 21% to 45% and from 15% to 33%, respectively,5-7 being higher in women, mainly because their Q- angle is higher than in men.2,8-10
There are several therapeutic alternatives to treat this condition, provided that, in patients with PFPS, healing knee pain is essential to improve their participation rates in physical and sports activities, which in turn will help them improve their body functionality and quality of life.11-13 In this sense, conservative (non-surgical) treatment for PFPS, based on physical therapy exercises, may lead to clinically significant pain level reductions, improvement of the knee functional capacity, and functionality recovery in the short and medium-term. However, the best way for a physical therapist to treat this disorder is still unclear; likewise, it is unknown if conservative management should be used with all patients with PFPS.2,4,14,15
Taking this into account, the objective of the present study was to determine the therapeutic effect of two muscle strengthening exercise programs in patients with PFPS (aged 15-45) from Bogotá, Colombia.
Materials and methods:
Study design
An experimental and randomized controlled clinical trial was conducted in 40 individuals (aged 15-40) who were diagnosed with PFPS from 2015 to 2018.
Sample size
In order to calculate sample size, a contrast non-parametric test of medians between two populations, adapted from Hollander et al.,16 and Delicado,17 was used to check the symmetric distribution of the groups. Finally, the table of critical values of the Mann-Whitney U test18 was used and a sample size of 20 individuals was established for each group. Consequently, out of the 60 patients who initially met the inclusion criteria, 40 were randomly distributed into groups A and B.
Study population: Participants were recruited from patients attending a doctor's visit and who were informed about the study by an orthopedic knee specialist. Upon their acceptance, they were referred to the main researcher to formalize their participation process.
Inclusion criteria
Being 15 to 40 years old and being diagnosed with PFPS from 2015 to 2018 (confirmed diagnosis through a CT scan of the knee).
Living in Bogotá, D.C.
Having clinical signs of patellar pain while resting, sitting for an extended period, or doing any following activities: going up or down stairs, jumping, running, squatting, kneeling.
Experiencing pain when moving the kneecap or being afraid of moving it at all.
Experiencing crepitus when doing squats.
Reporting unilateral or bilateral patellofemoral joint alignment complaints that were confirmed through a CT scan.
Having mild to moderate physical activity levels.
Exclusion criteria
Having a history of patellofemoral dislocation, subluxation or knee osteoarthrosis.
Having connective tissue disorders, knee bursitis, torn meniscus, patellar tendinitis, or synovial plica syndrome in the knee.
Having osteoarthrosis secondary to congenital diseases.
Having ligament or meniscal injuries.
Having undergone any type of lower limb orthopedic surgery.
Selection process
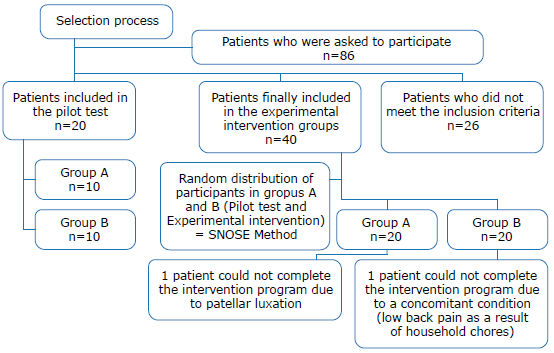
From January to June 2018, 86 people were asked to participate in the study, of which 26 were excluded since they did not meet the inclusion criteria: 12 were older than 40 years, 5 were younger than 15 years, 4 had been diagnosed with a condition other than PFPS (knee osteoarthritis), and 5 had undergone a knee surgery. Finally, based on the sample size previously established, out of the 60 participants who met the inclusion criteria, 40 were randomly selected to participate and complete the intervention programs according to the group into which they were classified. The study population selection process is shown in Figure 1.
Informed consent and ethical considerations
Before participating in the muscle-strengthening exercise programs, all participants (n=60, pilot test and experimental intervention) signed an informed consent. In addition, this study was granted ethical approval by the Research Ethics Committee of the Faculty of Medicine of Universidad Nacional de Colombia, as stated in Minutes 007-078-17 of May 11, 2017. Likewise, all procedures performed were in agreement with the ethical principles for medical research involving human subjects outlined by the Declaration of Helsinki19 and the scientific, technical and administrative standards for health research established in Resolution 8430 of 1993,20 issued by the Colombian Ministry of Health.
Pilot test
A pilot test was conducted in 20 participants who met the inclusion criteria and expressed their willingness to participate in the study, but they were not included in the final sample due to the size previously established (20 participants per group). It should be noted that all patients who met the inclusion criteria (n = 60) were randomly selected to be part of the experimental study or the pilot test using the sequentially numbered, opaque, sealed envelopes (SNOSE) method,21 and that said method was also used for group distribution. Taking this into account, participants selected for the pilot test were randomly assigned to both intervention groups: A (n=10) and B (n=10). The pilot test lasted 4 weeks and it was used to standardize the strengthening exercise protocol by identifying the degree of difficulty of the exercises, the execution speed, the characteristics of the rest periods to be implemented between each exercise series and the commands to be used to ask participants to start performing each exercise series. It must be noted that none of data collected during this phase was considered for statistical analysis. The prescription of the exercises was adjusted after conducting the pilot test, taking into account the training phases and the principles of the prescription.
Additionally, the 20 participants of the pilot test completed the remaining four weeks of the treatment proposed at the start of the study in compliance with the ethical principles established for conducting this study, but only the results of the first month of intervention were analyzed to make the necessary adjustments to the experimental protocol. It should be noted that all the subjects who took part in this study, both in the pilot test and in the experimental protocol, were evaluated at the beginning and at the end of the 8 weeks of intervention by a physical therapist different from the one who carried out the training sessions or physical exercises.
Intervention
All participants (n=40) were randomly distributed into two experimental groups using the SNOSE method (n=20): the intervention group, in which a core muscle, hip and knee muscle strengthening exercise program was implemented (group A, n=20) and the control group, where a hip and knee muscle strengthening exercise program was used (group B, n=20).
Likewise, they were asked to complete each muscle- strengthening exercise program according to the group they were assigned to. Both exercise protocols lasted eight weeks and each session (45 to 60 minutes) consisted of four phases: warming-up, strengthening, neuromuscular training, and stretching (Figure 2).
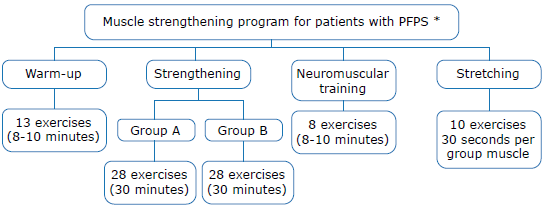
* Fora detailed description of each exercise, see Prieto-García.22 Source: Own elaboration.
Figure 2 Muscle strengthening exercise programs implemented in each group.
Exercise sessions took place at the Physical Rehabilitation Center of CAFAM IPS (Health Service Provision Institution) as follows: Three sessions per week during eight weeks, for a total of 24 sessions; each session was attended by the participants in groups of four people and was monitored by a physical therapy specialist, who was in charge of verifying that each exercise was properly performed, as well as teaching them the fundamentals of proper breathing techniques during the first two weeks of the intervention (anatomical conditioning phase), and providing them with feedback throughout the intervention. In addition, this specialist was also responsible for ensuring participants' posture was adequate for performing each exercise, thus avoiding low back pain as a consequence of using the wrong training method and increased intra-abdominal pressure due to inadequate breathing techniques when engaging in strength training.
Participants' adequate hydration during each training session was also ensured and, right before starting the intervention, they were informed about the importance of wearing appropriate footwear and sportswear for training. Also, during the first two weeks of the intervention, they were asked to wear training shorts so that the physical therapist specialist could see the position of their knees while performing the exercises. Then, they were asked to wear ankle length spandex pants to avoid any skin abrasion due to the rubbing effect of the TheraBand™; likewise, they were instructed to bring to the location where the sessions were held only a bottle of water for hydration and a towel to wipe their sweat, and to avoid wearing any item that could cause an injury during the sessions, such as bracelets or necklaces.
Study variables
Dependent variable: Anterior knee pain.
Independent variables: Muscle strengthening programs: Groups A (core, hip and knee muscles strengthening exercises) and B (hip and knee muscle strengthening exercises only).
Intervening variables: Age, sex, BMI, physical activity level, Q-angle, muscle strength, flexibility and unipedal balance.
Anthropometric measurements and assessment of physical activity levels and quality of life
The following anthropometric variables were measured for all participants: height, weight, body mass index (BMI), body fat percentage, muscle mass percentage, visceral fat percentage, basal metabolic rate, and metabolic age. Their level of physical activity was also measured using the International Physical Activity Questionnaire (IPAQ). Furthermore, anterior knee pain was measured using the visual analogue scale (VAS) and the Kujala anterior knee pain scale. The latter scale was used to assess participants' quality of life since this tool is specifically designed to measure the quality of life in people with PFPS by means of 13 questions grouped into 3 domains: pain and physical alteration, limb mobility limitations, and participation in sports activities.
Finally, a Microsoft Excel® sheet was created to record participants' data, including pain assessment, Q angle (right and left knee), core muscle strength, hip and knee muscle strength, muscle length, static balance, and postural assessment.10,23-27
Statistical analysis
Before conducting the statistical analysis, the database (the Microsoft Excel Sheet) was filtered by organizing the data collected according to each study variable. Then, a univariate analysis was performed to determine absolute and relative frequencies, followed by a bivariate analysis to compare the scores obtained in each of the domains of the Kujala scale. Furthermore, the Spearman's correlation coefficient was used to assess the correlation between Q-angle and anterior knee pain.
On the other hand, in order to assess whether there were differences or not regarding the study variables between both groups after completing the intervention, a comparison of the scores obtained after the administration of the Kujala scale and the Visual Analogue Scale (VAS) in both groups and the measurements obtained from the number of squats performed by each participant, their Q-angle, balance data, physical activity levels and core muscles strength measurements, was performed. In addition, normal distribution of data was evaluated using graphical and numerical methods. Finally, two-tailed statistical hypothesis tests were performed using a Cronbach's alpha coefficient of 0.05. STATA 14.0 was used to perform all statistical analysis.
Results
As mentioned above, 40 people with PFPS were randomly distributed into group A (n=20) and group B (n=20); however, only 19 participants of each group were able to complete the intervention program since one person in Group A presented with patellar luxation and a person in Group B withdrew from the study as a result of a concomitant condition that made impossible the proper execution of the exercises. Out of the 40 participants, only 4 (10%) were men; 26 (65%) had normal weight (BMI<25), and 14 (35%) were overweight (BMI≥25). Participants' average age was 32in Group A, and 29 in group B. The basic demographic characteristics of the study population, as well as their baseline (pre-intervention) measurements and scores for each study variable, are shown in Table 1. There were no significant differences between both groups at this stage.
Table 1 Basic demographic data and baseline measurements and scores of the study population by intervention group.
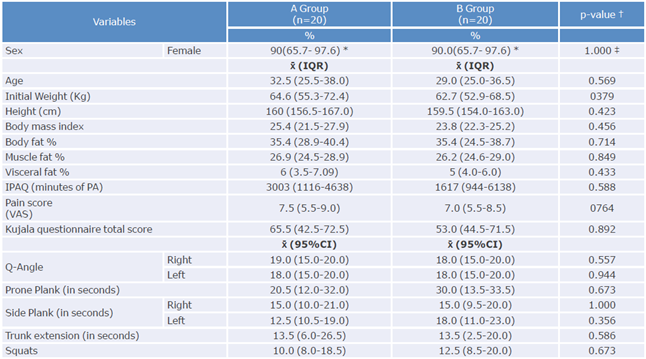
IPAQ: International Physical Activity Questionnaire; PA: Physical Activity; VAS: Visual Analog Scale.
* CI:95%.
† Mann-Whitney U.
‡ Chi square test.
Source: Own elaboration.
Post-intervention results
Table 2 shows the differences of the medians (post-intervention changes or differences in pain, knee alignment, core muscles, hip and knee strength, and balance) per intervention group for each study variable measured before and after the intervention.
Table 2 Effects of muscle strengthening exercise programs on participants' pain, knee alignment, core, hip and knee strength and balance by intervention groups.
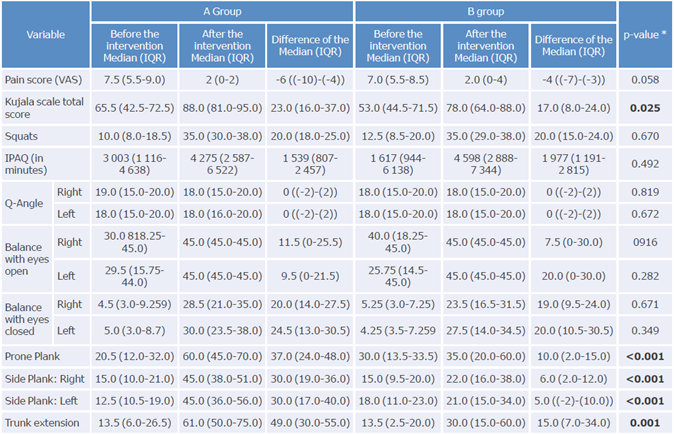
IPAQ: International Physical Activity Questionnaire; VAS: Visual Analog Scale.
* The Mann-Whitney U test was used to obtain the measurements of the difference of the median between groups.
Source: Own elaboration.
When core muscle strengthening exercises are added to the conservative (non-surgical) management of patients with PFPS or anterior knee pain, their quality of life, measured with the Kujala scale, improves since a significant pain reduction was reported in the present study in the group where these exercises were implemented. In addition, a statistically significant difference (p=0.025) was found between both groups in the total score of the Kujala scale, as participants in group A, in average, scored 5 points more than participants in group B (23.0 vs. 17.0), which shows that patients who were asked to perform core strength exercises had a better outcome regarding the improvement of their quality of life after completing the exercise program.
An increase in core muscle strength was also observed in group A after the intervention, especially in the case of side planks since the holding time in group A increased 30 seconds in average for both sides, while in group B it only increased 7 and 5 seconds in average for the right and left side, respectively, with a statistically significant p-value (p<0.001) in both groups.
On the other hand, differences regarding total pain scores according to the VAS were also observed between both groups: -6 (IQR: (-10)-(-4)) and -4 (IQR: (-7)-(-3)), respectively. Although these differences were not statistically significant, they were clinically relevant. In the case of hip and knee strength, measured through the squat test, no statistically significant differences were found in the median deltas between both groups, yet all participants, regardless of the intervention group they were in, increased their hip and knee strength after completing the program as a result of performing strengthening exercises for these muscle groups.
Discussion
According to the results obtained here, adding core muscle strengthening exercises to conventional management of PFPS (based on hip and knee strengthening exercises) is more effective to reduce pain in these patients than using only hip and knee muscles strength exercises.
Regarding hip and knee muscles strengthening, Neal et al.,28 state that typical exercise interventions performed in rehabilitation centers, and based on the strengthening of the muscles of the knee and the hip, have a positive impact on pain reduction and improve knee functionality, which is similar to the findings of the present study, where, according to the total score of the Kujala scale, all participants in both groups experienced pain reduction after completing the intervention program. Pain reduction in the total score of this scale has also been described in other studies, such as those conducted by Moradi et al.29 and Kettunen et al.30
On the other hand, Behm et al.,24 Anderson et al.,31 and Anh et al.9 have described that balance training using unstable surfaces increases central muscle activation, for activities that emphasize neuromuscular coordination involving the movement of the whole body are effective to increase balance. Therefore, performing unipedal standing balance exercises (when the base of support is reduced) and unilateral exercises increases the superficial muscular activation of core muscles. In this sense, a similar finding was observed in the present study since it was found that posture can be controlled with less effort, better coordination, and greater muscular efficiency after training by activating core and postural muscle. Thus, progressive balance training may improve both bipedal and unipedal balance in middle-aged people, especially in balance exercises done with eyes closed.
Furthermore, Oliver et al.32 reported that trunk extension exercises, performed in prone position, as well as the quadruped superman exercise, produced the highest activation levels in core muscles. These authors also described that single leg bridge exercise caused greater muscular activation of the buttocks, especially the gluteus medius, in the leg used to support the weight of the body.32 This finding was also observed in the last two weeks of the intervention program used in the present study, when these exercises were implemented to increase the activation of core muscles, as reported by Shirey et al.,33 Shirazi et al.,34 and Page.35 This activation was visually confirmed by the physical therapy specialist in charge of monitoring the performance of the exercises by observing the alignment of the pelvis when raising one of the two legs, indicating a greater activation of the gluteal and core muscles when the right hemipelvis was at the same height as the left hemipelvis.
Finally, Rabelo et al.,25 Bily et al.36 and Schneider et al.37 showed that implementing closed kinetic chain exercise programs using a proper proprioceptive input is effective to improve body functionality, reduce pain and make people more independent in terms of body movement. This was confirmed in the present study, as it found that improving the strength of core muscles helped reduce anterior knee pain and improve lumbopelvic rhythm, because participants' skills for performing the exercises improved in the last two weeks of the training program, showing a better quality of movement, especially at the lumbar-pelvic level, compared to their performance in the first week of the intervention. This in turn allowed improving body stability at the central level and, thus, achieving better distal motor control, mainly due to muscle activation.38
In general, the results of the present study are consistent with the findings of Alba-Martín et al. ,39 Nakagawa et al.,40 Gaitonde et al.,41 Motealleh et al.,42 Rabelo et al.,25 and Khayambashi et al.,43 who reported that conservative (non-surgical) treatments that use physical exercises help patients with PFPS by reducing their pain and improving their body functionality, and that those based on external rotators and hip abductor muscle strengthening exercises have better effects than those based only on strengthening exercises for the quadriceps femoris.
Conclusions
Adding core muscle strengthening exercises to traditional exercise programs for strengthening gluteal muscles, vastus medialis oblique and vastus lateralis of the quadriceps femoris increases the program effectiveness to reduce pain and improve knee functionality in people with PFPS.
Static balance training allows individuals to improve selectively their proprioception at the level of the ankle, the sacroiliac joint and the neck (cervical vertebrae) by reducing the base of support and the available visual information, providing greater stability and neuromuscular control of the lower limbs in daily life activities, such as going up and down stairs.
Preferentially, core muscle strengthening exercises should be included in health rehabilitation or training programs since the activation, coordination and selective control of these muscles may result in greater postural stability, mobility of the upper and lower limbs, and less risk of injury.
Based on the findings of this study, patients with PFPS should continue their core, hip, and knee muscle strengthening exercise program after completing the two-month period outlined here, so that their quality of life improves as they continue to participate in the exercise program.

