











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
Permalink
Introduction
DRESS syndrome is a rare condition caused by a hypersensitive and disproportionate response of the immune system to exposure to various chemicals, mainly drugs. Its incidence is still unknown, but the risk of presentation in patients exposed to drugs is estimated to be between 1 in 1 000 and 1 in 10 000.1 Due to the lack of clearly defined criteria, it is often considered as a clinical diagnosis of exclusion. According to Husain et al.,2this condition may cause high mortality rates (up to 10%) if not detected in a timely manner.
The term DRESS (drug rash with eosinophilia and systemic symptoms) was coined in 1996 by Bocquet et al.,3 but Chaiken et al.4 described a similar condition associated with the use of phenytoin as early as 1930. Over time, this syndrome was classified as a serious adverse drug reaction, along with other skin reactions such as Stevens-Johnson syndrome, acute generalized exanthematous pustulosis, and toxic epidermal necrolysis.5
The objective of this report is to expose an unusual presentation of DRESS syndrome in order to guide its timely diagnosis, thus avoiding complications arising from the late treatment of these patients.
Case presentation
A 24-year-old man from Calarcá (Quindío, Colombia) visited the emergency department of a secondary care hospital in the municipality where he lived due to a three-day history of unquantified intermittent fever, asthenia, adynamia, anorexia, moderate global headache, myalgia, odynophagia, and non-radiating colicky upper abdominal pain.
The patient had no significant medical, allergic, or family history; however, 20 days before the initial assessment, he was involved in a motorcycle accident and sustained severe cranioencephalic trauma, requiring surgical management with decompressive craniectomy. On that occasion, he had an adequate clinical course in the postoperative period and was discharged 4 days after the procedure with a prescription for non-steroidal anti-inflammatory drugs every 8 hours orally to treat pain and phenytoin oral capsules 100mg orally every 8 hours indefinitely until a new neurosurgery follow-up.
During the assessment made in the emergency department, the patient was febrile, tachycardic, dehydrated, and with evidence of generalized skin rash. Therefore, additional laboratory studies were requested, which revealed elevated transaminase levels and eosinophilia. Since no other alterations were reported, management at the highest level of care was considered necessary, and he was referred the next day to the Clínica Central Del Quindío in the city of Armenia (Colombia).
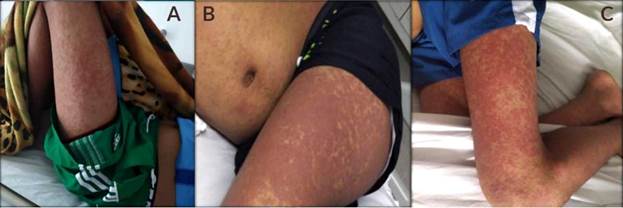
The patient was admitted to the clinic in acceptable general condition with the following vital signs: temperature of 38.8°C, heart rate of 118 bpm, respiratory rate of 25 breath/min, and blood pressure 112/66 mmHg. Physical examination revealed that he was dehydrated (grade II), with pain on deep palpation in the right hypochondrium, no signs of peritoneal irritation, and presence of plaque-like lesions and confluent erythematous urticaria-like papules distributed mainly in the lower limbs and trunk (Figure 1). During the initial approach, laboratory and imaging studies were requested, and the most relevant findings are presented in Table 1.
Source: Document obtained during the course of the study.
Figure 1 Plaque-like lesions and confluent erythematous urticaria-like papules. A) At the time of admission; B) and C) after a few days of hospital stay.
Table 1 Imaging and laboratory findings.
| Test | Relevant findings |
|---|---|
| Blood count | Moderate eosinophilia (1000 cells/microliter) |
| Transaminase level | AST 916U/L - ALT 998U/L |
| Bilirubin | Total: 2.5 mg/dl. Direct: >1.85mg/dl |
| Hepatobiliary ultrasound | Normal |
Source: Own elaboration.
The treatment plan was to administer a single dose of corticoid (hydrocortisone 100mg IV) and analgesics and antipyretics (dipyrone 1g IV), as well as intravenous hydration (1000mL bolus of 0.9% saline). It was also decided to admit the patient to the hospital so that the internal medicine service assessed him. The specialist requested a viral panel to detect hepatotropic viruses, HIV ELISA, serological test for syphilis (VDRL), blood cultures, and urine culture.
During the second day of hospitalization, and while awaiting the report of the studies, the patient continued with intermittent fever, so it was decided to start antibiotic management with ceftriaxone 1g IV every 12 hours for broad-spectrum coverage.
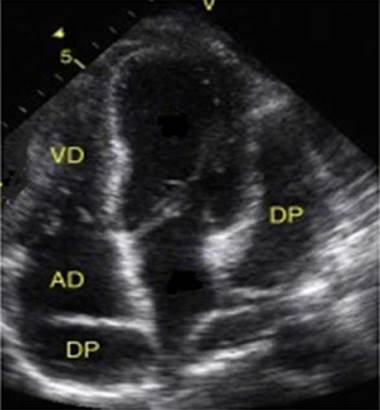
On the third day of hospital stay, HIV, VDRL, and culture test results were negative, and other causes of fever, including an autoimmune origin, were considered. Anti-nuclear antibodies, extractable antibodies, and anti-DNA antibodies, as well as an aprocalcitonin test, were requested as part of the care protocol in patients with fever of unknown origin. A possible endocardial infection focus was also considered, so a transthoracic echocardiogram was requested, the results of which were obtained the next day and revealed mild pericardial effusion located in the posterior wall of the right atrium, moderate pericardial effusion adjacent to left cavities (Figure 2), and no signs of tamponade, constriction, or hemodynamic effects.
Source: Document obtained during the study.
Figure 2 Transthoracic echocardiogram showing mild pericardial effusion in the posterior wall of the right atrium and moderate adjacent pericardial effusion adjacent to the left cavities. AD: right atrium; RV: right ventricle; PD: pericardial effusion.
In view of this relevant finding, on the fourth day of hospitalization and with all the laboratory results, a new evaluation of the case was carried out considering the possible differential diagnoses. After evaluating the patient's condition, it was decided to rule out both infectious and autoimmune etiologies due to negative laboratory test reports, the absence of fever for more than 24 hours, and the negative polymerase chain reaction (PCR) test. Therefore, other drug-related causes were considered, including DRESS syndrome, which was proposed as a diagnostic option due to the fulfillment of the three main characteristics of the disease: skin lesions, presence of eosinophilia, and multisystem involvement presumably associated with the use of anticonvulsants (phenytoin), which were suspended to subsequently initiate therapy with glucocorticoid methylprednisolone (500mg IV every 24 hours for 3 days).
On the third day of treatment, skin lesions had almost completely disappeared, and liver function and eosinophilia had normalized; therefore, it was decided to discharge the patient with a prescription of prednisolone 1 mg/kg/ day for 5 days and gradually taper off, to discontinue the anticonvulsant medication, and to schedule an outpatient visit 15 days later. During the follow-up consultation, it was found that the patient had progressed satisfactorily and had no subsequent complications.
Discussion
DRESS syndrome is a severe drug hypersensitivity syndrome that causes cutaneous and systemic manifestations. Its pathophysiology is not clearly understood, but it has been suggested that it may be related to drug metabolism enzyme deficiency, impaired drug detoxification, lymphocyte activation, herpes virus reactivation, genetic predisposition, among others.2
According to reports from the RegiSCAR study, conducted between February 2003 and May 2006, the genesis of this syndrome is related to approximately 316 therapeutic components, finding a stronger relationship with aromatic antiepileptic drugs (35%), followed by allopurinol (18%), and sulfamides (12%).6
In terms of clinical presentation, organ dysfunction is relatively rare in DRESS syndrome, but it primarily affects liver and kidney function and causes myocarditis, pneumonitis, and, less frequently, meningoencephalitis.7 Likewise, electrocardiographic findings such as T-wave alterations, sinus tachycardia, low ejection fraction, elevated troponin I, systolic dysfunction, biventricular heart failure and, in very rare cases, pericardial involvement have been described as unusual heart abnormalities.8
Due to the wide spectrum of symptoms generated by this syndrome, attempts have been made to establish criteria for its definition; however, currently only three key features have been proposed for its diagnosis: multisystem involvement, drug-related skin lesions, and eosinophilia or the presence of atypical lymphocytes. However, the time of onset of symptoms, their relationship to the start of drug administration, and the improvement after medication discontinuation have been considered as possible new criteria.9
Regarding differential diagnoses, it should be noted that the symptoms observed during the course of this condition are similar to those seen in other syndromes, such as those resulting from bacterial infections, viral infections by cytomegalovirus, HIV, Epstein-Barrvirus, viral hepatitis, connective tissue diseases, and febrile rash;10 thus, these diseases should be considered and ruled out using diagnostic and laboratory aids, as in the case presented here.
Regarding the treatment of DRESS syndrome, the first step is to discontinue the related drug, followed by the administration of corticosteroids at doses equivalent to 1-2 mg/kg per day of prednisone.11 Other treatments, such as antiviral drugs, immunoglobulins, cyclosporine, cyclophosphamide, azathioprine and rituximab or the use of plasmapheresis, have not yet been approved due to their poor efficacy.12,13
Finally, it should be kept in mind that prospective studies recommend long-term follow-up after treating the acute episode, since this syndrome has been associated with various autoimmune diseases, including Graves' disease, systemic lupus erythematosus, type 1 diabetes mellitus, and autoimmune hemolytic anemia, which may occur in 3-5% of patients.14
Conclusion
Although DRESS syndrome has a low incidence and poses a diagnostic challenge, mainly because of its heterogeneous clinical presentation, it should always be suspected, especially in patients with cardiac and pericardial involvement. This case, in particular, demonstrates that, while pericardial involvement is rare, it has a major impact on these patients because adverse outcomes and mortality may increase significantly. Therefore, timely diagnosis and appropriate treatment are critical, as in the present case, as they allowed avoiding adverse outcomes and long-term sequelae.

