











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Empathy is an attribute that allows dentists and their patients to have a positive inter-subjective relationship,1,2 hence contributing to increased satisfaction and reduced stress levels in patients. It also helps to improve adherence to treatment and create a generally supportive environment for care, among other benefits.3-7
The process of empathy development is complex8-12 because it encompasses both ontogenetic and evolutionary variables.13,14 However, the former are currently more significant, and society in general, and universities in particular, must take advantage of all opportunities for its development and positive consolidation.15-22
It has been established that neuronal development "ends" around the age of 25; however, brain plasticity may be an important factor that prolongs the capacity to acquire empathy over time.10 As a consequence, universities should undertake the training of this skill in their undergraduate and graduate students (particularly in the medical sciences).
One of the most widely used instruments to assess empathy levels in dental students is the Jefferson Medical Empathy Scale S version (EEMJ-S),2,5,9,10-12,14-16 which measures the levels of empathy (E) and its three dimensions -compassionate care (CC), perspective taking (PT), and walking in the patient's shoes (WPS)- and has been well characterized in several studies.1-22
A good diagnosis of empathy is based on an understanding of the distribution of observed levels of empathy (and its dimensions), as well as the factors impacting this distribution. One of such factors is potential variability among students in dental schools or faculties within a country or between different countries. Thus, the specificity of a given distribution of empathy in a student population may be associated with the need of adopting methodologies, approaches, and strategies that are equally specific to the state of empathy in particular.
In this context, the objective of this study is to determine whether there is variability in empathy levels between two populations of dental students and to describe theoretically the general implications of this variability for intervention strategies.
Materials and methods
Study type and population
Exploratory cross-sectional study conducted among first- to fifth-year dental students from the universities Santiago de Cali (USC, Cali, Colombia) and San Sebastián (USS, Santiago, Chile).
The total population of dental students enrolled in USC in 2017 was 647 (N), of which 610 (n) (94.28% of the study population) were administered the culturally adapted scale. According to their year of training, students were distributed as follows: 57 in the first-year, 147 in the second-year, 95 in the third-year, 181 in the fourth-year, and 130 in the fifth-year. The distribution by sex was: 340 women and 270 men.
On the other hand, in the USS (comparison group), the sample consisted of 535 students out of a total of 800 (N) enrolled in 2016 (66.88% of the study population). The distribution according to the academic year they were studying was: 109 in the first-year, 118 in the second-year, 119 in the third-year, 86 in the fourth-year, and 103 in the fifth-year. The distribution by sex was: 349 women and 186 men.
Students who did not agree to respond voluntarily to the instrument, did not sign the informed consent form, and were absent on the day the scale was administered were excluded from sample selection.
Data collection and processing, statistical analysis, and the instrument used to measure empathy levels (EEMJ-S) were the same in both groups. It should be noted that the results obtained from the Chilean students have been published in detail and are easily accessible.1,2,9,16,17
Instrument
The EEMJ-S is a self-administered instrument that was adapted for dental students in Colombia and Chile based on the criteria of Lopez-Pérez et al.1 and Diaz-Narváez et al.,17 respectively. This scale was subjected to a review by judges prior to its administration, so its cultural validity was verified by five ad hoc academics.
The results of the study on psychometrics and invariance of the EEMJ-S three-dimensional latent model for the Caribbean and Central America, including Colombia, were recently published by Diaz et al.,9 while the results from Chile were recently submitted for publication by Diaz-Narváez (Personal Communication). The presence of the three-dimensional model and its invariance across populations and sexes was demonstrated in those research works, allowing us to compare the populations studied in this work.
Procedures
A neutral operator administered the scale in person, ensuring that students could complete the instrument in a quiet and orderly environment, clarifying doubts about how to respond properly, verifying that the questionnaires were handed over with all questions answered, and ensuring that the informed consent form attached to the instrument was signed. It is important to note that the scale was not administered to all students at the same time, but during different sessions based on their year of training.
Data was collected at USC in September and October 2017, and at USS in September and October 2016.
Before being administered, the culturally adapted instrument was tested on 30 dental students from other universities in order to ensure that the participants understood the questions. The characteristics of this application have already been explained in other works.
Statistical analysis
Primary data were tested for normality (Kolmogorov-Smirnov test) and homoscedasticity (Levene). Means and standard deviations were also estimated for analysis. A factorial analysis of variance (three-factor ANOVA, Model II) was performed on the three factors studied: University (U), Course (C), and Sex (S). Data reliability was calculated using Cronbach's alpha coefficient and intraclass correlation coefficient.
Data were described by means of simple arithmetic graphs. Eta-squared effect size (ń2) and test power (PP=1-β) were estimated to determine the degree of statistical differences and the probability of type II error, respectively. Calculations were performed using the SPSS 25.0 software. The significance level used was α<0.05 and β≤0.20.
Ethical considerations
The study took into account the ethical principles for medical research involving human subjects established by the Declaration of Helsinki23 and the provisions on health research of Resolution 8430 of 1993 of the Colombian Ministry of Health.24 The research was approved by the Ethics Committee of the Faculty of Dentistry of the Universidad San Sebastián, in accordance with resolutions 2015-02 of January 28, 2015, and 2020-83 of January 20, 2020 (extension of the first resolution).
Results
Tests for normality and homoscedasticity were not significant (p>0.05). Cronbach's alpha estimated for the instrument administered to USC students was satisfactory (untyped: 0.675 and typed: 0.727), so it is possible to infer that the empathy data measured in the participants have internal consistency. Total Cronbach's alpha, if one item (question) was removed, was estimated with replacement items for the next calculation and fluctuated between 0.675 and 0.727. Intraclass correlation coefficient was 0.719 (95%CI: 0.685-0.750; F=3.56; p=0.000l), which confirms the good reliability of the instrument. Reliability results obtained in the comparison group were similar to those found in the present study.17
Table 1 presents the means (total and combined by factor) and the standard deviations for empathy and their dimensions at each of the levels of the factors evaluated, as well as the respective interactions of the two populations studied. This same table details partial and total sample sizes for the U, C and S factors, including their interactions (*).
Table 1 Results of the mean and standard deviation estimation for empathy and its dimensions by university, course, and sex.
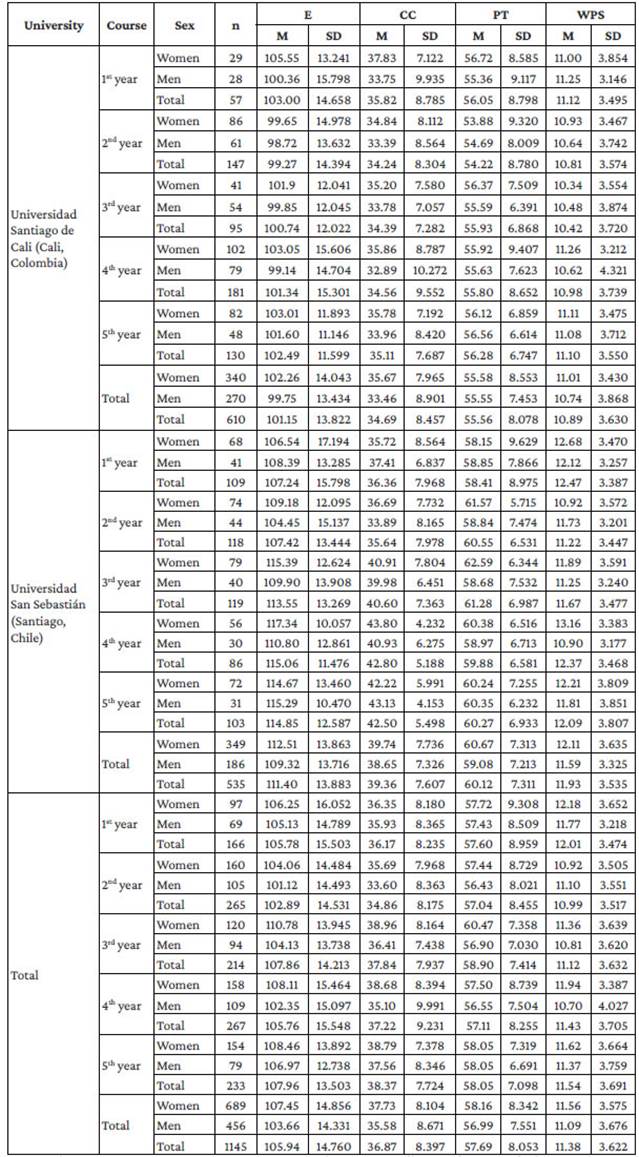
E: empathy; CC: compassionate care; PT: perspective taking; WPS: walking in the patient's shoes; M: mean; SD: standard deviation.
Source: Own elaboration.
Table 2 presents the results of the comparison of the means for empathy and its three dimensions among the U, C and S factors, as well as the estimation of the effect size and power of the test. Only the U, C and S factors and the U*C interaction were highly significant (p<0.01), which means that E values are different between universities, between courses in each university, and between sexes. The presence of interaction shows that there are also differences between equivalent courses of both universities (Figure 1a and 1b). Effect size values were medium and low in U and U*C, respectively, and low for C and S. The probability of committing a type II error was very low in all three factors and in the interaction.
A situation comparable to that of E occurred in the CC dimension: the same factors and interactions were highly significant in both (p<0.005): U, C, S, and U*C. In addition, effect size for U was considered medium, but low in the other factors that were significant; therefore, there are significant differences between the mean scores of the two groups studied for this dimension, although the differences in the other factors (C and S) and in the U*C interaction were small (Figures 1c and 1d). The probability of committing a type II error in these comparisons was low or null.
Finally, in the PT and WPS dimensions, the only factor that was highly significant was U (p<0.005), with medium effect size values for PT (Figure 1e and 1f) and low for WPS (Figures 1g and 1h).
Table 2 Results of the comparison of the means of Empathy and its dimensions between the factors University, Course and Sex, and estimation of the effect size and power of the test.
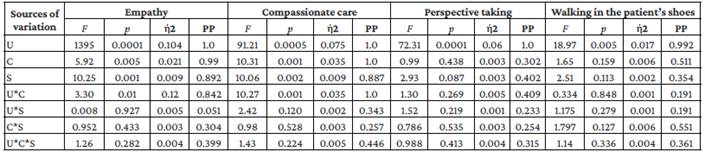
U: university; C: course; S: sex; f 2: effect size coefficient (eta-squared); PP: power of the test or type II error (1-β)
Note: The asterisk (*) represents the interaction between factors; p<0.05 was considered significant, p<0.01 was considered very significant, and p<0.005 was considered highly significant.
Source: Own elaboration.

Discussion
It is important to stress that empathy is the result of the active synthesis of its components, including cognitive (PT and WPS) and emotional (CC) aspects.12,14,16 As a consequence, if any (manifestation) of these dimensions is "depressed" for any reason, it not only causes a decrease in the values of the global empathy measure, but it also leads the empathy "system" to enter into what could be called a state of "imbalance" and prevents its expression as a whole.
The aforementioned situation limits, to varying degrees, empathic attitudes; therefore, the observed score is always an external reflection of the "development of empathy" of a student or student population, although it does not explain much of the actual state of empathy. For example, if someone gets the highest score in CC (49 points), the highest in PT (70 points), and only 3 points in WPS (maximum of 21), where the EEMJ-S has a maximum total of 140 points, this person's scores would sum up to 122 and could be classified as having high levels of empathy. However, it is clear that such a person has an extremely depressed WPS dimension, and as a result, they may be compassionate for what another person is suffering while also avoiding empathy contagion by avoiding obnubilation, but they have a severely diminished capacity to understand and comprehend what the other person is feeling and thinking.
On the other hand, if empathy is considered an open system, then it is possible to infer that it is subject to the pressure of both external and internal factors (derived from neurophysiological functioning) that influence its shaping and consolidation process.12,13,16
This influence need not be the same everywhere, nor do the same factors affect the ontogenetic development of an individual student or a student population everywhere.
On the basis of the above, the concept of empathy expression variability takes on a theoretical basis and that should be explained. One way of doing this could be to understand or study the internal and external factors that influence empathy and how they can modulate its expression in a positive or negative way;2,6,7,9-19 such understanding could indirectly lead to a causal explanation (at best) or observation of a certain degree of dependency or association of empathy with a given factor or factors.
Actually, if the present study takes into consideration differences that simultaneously mark significant statistical differences, acceptable values (medium and low) of the effect size24-26 and high levels of statistical power of the test as consistent differences (variability) between the factors studied in both universities,24 variability would be present only in the U, C and U*C factors in E and in the CC dimension. In the other dimensions, differences were found only in factor U. These findings constitute empirical evidence confirming the results of variability that have been systematically found by other authors in dental students1,2,17,27-30 and other health sciences specialties in Latin America.10-12,15,16,19 In relation to the differences found in factor C, it was observed that the variability is also evident in relation to the process of "evolution" of empathy levels throughout the courses, which is called "decline in empathy."31
This process is associated with the phenomenon called "erosion of empathy,"32 which consists of the decrease in the levels of empathy among students as they move into more advanced courses. This has been attributed to several possible causes,33 including the existing curriculum, excessive academic load, bully professors, academic harassment, the students' family situation, or their personality type, among many others.1,2,11,12,14,16,17,29-32,34 However, the presence of a generalized decline in empathy has been called into question in various research conducted both in Latin America,1,2,12,16,17,19,27,30,34,35 and other regions of the world.36-38
It is necessary to clarify that the existence of this process is not denied, but what is questioned is its absoluteness; in other words, decline is believed to be another manifestation of the trends towards change in levels of empathy and its dimensions throughout the courses.34 As shown in Figure 1 (Figures 1a-1h), trends in the change of empathy levels in both groups were variable: there was a steady increase in empathy levels in some cases, a specific decrease in others, and the classic decline model proposed by Hojat et al.31 and by Hojat et al.32 in another. Thus, it is possible to say that the fact that the statistically significant differences between the sexes in E levels and its three dimensions have near-zero effect size values implies that these differences are small.
These results may be considered as a manifestation of variability. Indeed, a study comparing levels of empathy and its dimensions in 18 dental schools of Latin American universities found both differences (in some cases favorable to men and in others to women) and similarities among them.39 Therefore, the absence of sex differences can be considered as a form of variability. The possible causes of these results have been described in other papers,1,2,16,17,19,22,27-30,34,35,39 but there is still controversy about the possible explanations that give rise to the characteristics of variability between men and women, since the results cast doubt on whether empathy levels depend strictly on a stereotypical approach to gender. As a matter of fact, the construction of gender identity is a complex process involving biological, social, cultural and psychological factors,40 and the development of empathy is not alien to the influence of these factors.2,11-17,21,34,35,40-47
If universities have the comprehensive training of their students as their social mission, then they also have the obligation to foster the development of empathy in them and to consider the possibility that empathetic behavior varies within each country or across Latin American countries, as evidenced by some studies conducted in other regions.15,48
As empathy is the product of many factors that influence the training of a particular student or population of university students,2,11,12,14-16 the materialization of the concern for professional training in universities must begin with the articulation of strategy empathy development. This training should begin with a rigorous diagnosis of empathy that, in general, starts with an understanding of the characteristics of empathy level (and its dimensions) distribution in students and the evaluation of the factors that could theoretically explain the observed positive or negative distribution.
A second step could be to obtain a new diagnosis of empathy that also involves new factors "suspected" of impacting empathy and its dimensions, based on the results of the initial diagnosis. Then, an intervention could be done to help students develop empathy, to an adaptive level, to stimulate positive factors while attenuating or eliminating negative factors, and finally to determine whether the intervention had the desired effect.10,19,20
The complexity of empathy would mean, theoretically, that a successful intervention is not a short-term achievement, nor is it the result of a single intervention, but rather of a series of interventions.2-4,9-17,19-21 characterized by the application of extension (during undergraduate training) and in-depth interventions, which may prove the need to revise the curriculum and use active teaching-learning strategies.
As a result, the methods to be employed to improve empathy and its dimensions depend strictly on the concrete and precise diagnosis of empathy in a student population, since not every method will increase the reduced dimensions identified during the diagnostic phase. On the other hand, there is no single discipline that can devise the type of intervention and properly choose the methods (or create them, if necessary) resulting from a specific diagnosis.
Thus, the empathetic strategy requires the application of an interdisciplinary and complex approach that would involve the use of different methods to achieve a specific strategic orientation derived from the empathy level found in a given student population (diagnosis of empathy). Consequently, the application of methods designed to raise empathy without considering the prior performance of a diagnosis of empathy and an intervention strategy that is not in line with such diagnosis will, in theory, fail. Moreover, if such "interventions" are short-term, they will also be a reason for failure. The characteristics of the empathy attribute and the theoretical-conceptual characteristics of the empathy construct13-15,41-48 make it necessary to carry out in-depth and extended interventions over time, so the effectiveness of such an intervention can only be verified when the students are already exercising their profession.
Conclusions
The results obtained in the present study, based on the administration of the EEMJ-S, show that there is variability in the levels of empathy and its dimensions between the two groups studied. Differences between sexes were also evident, but these are not significant because they had very low effect size values. However, the lack of differences can be considered as a manifestation of variability if this study is placed in the context of Latin America.
The responsibility of raising the levels of empathy (and its dimensions) requires some steps logically derived from the theoretical-conceptual apparatus of the empathy construct, which consists, in general, in obtaining an accurate diagnosis of empathy; carrying out an intervention or successive interventions perfectly adapted to the characteristics of the diagnosis or subsequent diagnoses; and the implementation of approaches that help guide strategies and choose appropriate methods for this purpose.
It should be noted that the conclusions described have limitations that derive from the differences between sample sizes in both populations, which determine that the estimation of parameters is affected, specifically in USS students. As a result, comparison results may have a certain degree of sampling error; however, these same results show consistent trends.

