










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Latinoamericana de Psicología
Print version ISSN 0120-0534
rev.latinoam.psicol. vol.44 no.3 Bogotá Sept./Dec. 2012
Validation of the BASR relaxation technique for the control of craving, anxiety and stress in an experimental nicotine withdrawal set
Validación de la técnica de relajación RBSA para el control del craving, la ansiedad y el estrés bajo condiciones experimentales de abstinencia a la nitcotina
Fernando Calvo Francés
Elba Betancort Tabares
María Dolores Díaz Palarea
Universidad de Las Palmas de Gran Canaria, España
Acknowledgments: upported was provided by TS12005-07764-C02-02 I+D+I grant from the Ministry of Education and Science and the European Regional Development Fund (FEDER). Correspondencia: fcalvo@denf.ulpgc.es
Recibido: Marzo de 2012 Revisado: Abril de 2012 Aceptado: Agosto de 2012
Abstract
Anxiety, craving and stress are associated with a higher risk of recurrence and a success reduction of smoking cessation programs. Relaxation techniques are one of the resources that psychology can bring to bear on these programs. The Brief Automated Suggestive Relaxation technique (BASR) is presented. Its design carries with it the idea of creating a brief and self-applied procedure which allows one to obtain results from the outset with minimum effort by both patient and therapist. This technique is confirmed within the multi-component program for smoking cessation as a confrontation resource for symptoms of anxiety/craving/stress deriving from quit smoking and nicotine Withdrawal Syndrome, its possible effectiveness was studied. There were 45 participants and all were smokers (average age of 43.91, 55.6% women), randomly divided in two groups: BASR condition (15 minutes relaxation session) or control condition (15 minutes rest session). Two standardized tests were used for the evaluation, the Anxiety-State scale (STAI-S) and the Differential Stress Inventory of Adjectives for the Study of Moods (IDDA-EA). An analogical qualification Scale of Smoking Desire was also used. In agreement with findings, a positive effect and the efficacy of the technique employed for the control of craving, anxiety and stress in smokers was corroborated.
Key words: anxiety, craving, relaxation, smoking, stress, withdrawal Syndrome.
Resumen
La ansiedad, el craving y el estrés se asocian con un mayor riesgo de recurrencia y a una reducción del éxito de los programas para dejar de fumar. Las técnicas de relajación son uno de los recursos que la psicología puede aportar a estos programas. Presentamos la técnica de Relajación Breve Sugestiva Automatizada (RBSA), diseñada con la idea de crear un procedimiento breve y auto-aplicado que permita obtener resultados inmediatos y con un mínimo esfuerzo tanto del paciente como del terapeuta. Esta técnica se integra en un programa multicomponente para dejar de fumar como un recurso para la confrontación de los síntomas de ansiedad/craving/estrés que se derivan de dejar de fumar y del Síndrome de Abstinencia de la nicotina. Se estudió su posible eficacia. Participaron 45 fumadores (edad promedio de 43.91, 55,6% mujeres), divididos aleatoriamente en dos grupos: condición RBSA (sesión de 15 minutos de relajación) o condición de control (15 minutos de reposo). Se utilizaron dos pruebas estandarizadas para la evaluación, la escala de Ansiedad-Estado (STAI-S) y la escala de Estrés del Inventario de Diferencial de Adjetivos para el Estudio de Estados de Ánimo (IDDA-EA). También se empleó una escala analógica para la evaluación del Deseo de fumar. De acuerdo con los resultados se constató un efecto positivo y la eficacia de la técnica empleada para el control del craving, la ansiedad y el estrés en fumadores.
Palabras clave: ansiedad, craving, estrés, fumar, relajación, síndrome de abstinencia.
A great smokers' quantity smoke when they are worried, irritable or upset (Tobacco Advisory Group of the Royal College of Physicians, 2000), and this is, in all probability, the way smokers will feel when they face a treatment for smoking cessation.
The presence of anxiety figures into the diagnostic criteria for nicotine withdrawal (American Psychiatric Association 2003; Organización Mundial de la Salud, 2003). Several studies have confirmed it as one of the most common mood alterations for recent former smokers (Cami & Farré, 2003; Hughes, 2007; Hughes, Higgins & Bickel, 1994; Lara, Ramírez, Sansores, Espinosa & Regalado, 2007). Post-cessation anxiety is a key factor for understanding temporary lapses and relapses (Brown, Lejuez, Kahler, Strong & Zvolensky, 2005; Piasecki, 2006). Smokers who are unable to remain abstinent at least one week, compared with those who remain abstinent, manifest a reactive anxiety to bodily sensations of symptoms, which are significantly higher (Zvolensky, Feldner, Eifert & Brown, 2001).
Also there is craving, which could be defined as a desire to experience the effects of a previously used psychoactive substance (Iraurgi & Corcuera, 2008). Therefore, it is noteworthy that smokers use predominantly affective descriptors to characterize their experience of craving. The most common terms are "irritated," "agitated," "frustrated," "tense," "nervous," and "anxious" (Shadel, Niaura, Brown, Hutchinson & Abrams, 2001). Craving to smoke, the most prominent and bothersome symptom experienced during nicotine withdrawal, is central to understand continued smoking and is a significant predictor of smoking relapse. For this reason, craving may impede smoking cessation, and smokers need strategies for reducing craving and increasing abilities to cope with it (Allen, Bade, Hatsukami & Center, 2008; Shiffman, 2000).
Research found that adult smokers experience periods of elevated stress between cigarettes and that tobacco only restores their stress levels to normal (Hughes, Higgins & Hatsukami, 1990; Office of the U.S. Surgeon General, 1998; Parrott, Garnham, Wesnes, & Pincock, 1996; Schachter, 1978). Nevertheless, soon after smoking another cigarette is needed to maintain normal stress levels, as a matter of fact, if the smoker does not have another cigarette, he begins to experience the tension caused by tobacco abstention. The study suggests that smoking does not relieve stress; in fact, it can contribute to raising it (Parrott, 1999; Tobacco Advisory Group of the Royal College of Physicians, 2000).
The highest Anxiety associated with Withdrawal Syndrome usually appears 24 hours after sudden interruption or decrease of dosage (Hughes et al., 1994) but significant levels of anxiety, craving and other symptoms also could appear even before one hour or in the first six hours after quit (Hendricks, Ditre, Drobes & Brandon 2006; Teneggi et al., 2002). In the following weeks, when the acute phase of the syndrome has been overcome, average anxiety levels fall below levels prior to abandonment (West & Hajek, 1997).
Anxiety, craving and stress are three key factors to keep in mind since they are associated with a higher risk of recurrence and the consequent effect of reducing the success of smoking cessation programs (Hughes, 2007; Lara et al., 2007; Quesada, Carreras & Sánchez, 2002). Possibly all of them contribute to the mechanism of negative reinforcement in the maintenance of smoking behavior. The relief of symptoms after taking up smoking again produces a false sensation that cigarettes have a calming effect. In reality, it only re-establishes acceptable minimum nicotine levels in function of the degree of dependence/tolerance.
Consequently, we can deduce that is very useful for smokers to have some efficient resource management for all of the aforementioned factors after quit, especially in the acute phase of Withdrawal Syndrome, but also to break the negative reinforcement mechanism.
Relaxation techniques are one of the resources that psychology can bring to bear on all of them. The evidence of the effectiveness of relaxation techniques on anxiety and stress is not new (Lichstein, 1988; Öst, 1987; Woolfolk, Lehrer, McCann, & Rooney, 1982). Relaxation techniques are considered, according to different criteria and reviews, well-established treatment or probably well-established for disorders related to anxiety, such as generalized anxiety, panic disorder, obsessive-compulsive disorder and psychosomatic disorders such as migraine and recurrent headache (Chambless & Ollendick, 2001; Natham & Gorman, 1998; Pérez & Fernández, 2001). Also, as regards to stress (Pawlow & Jones, 2005; Ponce et al., 2008) and craving (Cropley, Ussher & Charitou, 2007; McClernon et al, 2004; Ussher, Cropley, Playle, Mohidin & West, 2009), the validity of relaxation techniques has been confirmed.
But, which relaxation training should be used? We have considered various facts. First, different meta-analytic studies have confirmed the significant superiority of the effects of relaxation techniques based on respiration over other techniques (Rosa, Olivares & Sánchez-Meca, 1998; Sánchez-Meca, Rosa & Olivares, 1998a; Sánchez-Meca, Rosa & Olivares, 1998b). It is possible to add that within those respiratory methods, when breathing at rates lower than basal and exhalation is increased until it is twice as long as inhalation (Conde Pastor & Menéndez, 2000) and periods of breathe retention between inhalation and exhalation (Lichstein, 1988), so, better results can be obtained. Secondly, and in accordance with ABC theory (Attentional Behavioral Cognitive) of Smith relaxation (2001), distinct relaxation techniques produce different psychological states of relaxation (R-States) (Amutio, 2002a, 2002b, 2006), and do not produce the same correspondence between physiological measures and subjective measures in all techniques (Fernández-Abascal & Miguel, 1979, 1980; Smith, Amutio, Arteaga & Aria, 1996). This implies that effects on different levels and symptoms of stress and anxiety can be differentiated (Amutio, 2006). Relaxation techniques based on respiration produce R-states of high affective energy indicated for symptoms or problems related to negative affective activation associated with stress, and to increase personal energy levels as well as self esteem (Amutio, 2002a, 2002b, 2006). According to this, relaxation techniques based on respiration are indicated for control of anxiety (negative affective activation) and for detoxification (such as a stressful situation).
This study has taken into account studies on instruction management and suggestion (González-Ordi & Miguel-Tobal, 1998) and the use of music, the positive effects on the relaxation response have been verified (Jaber et al, 2007; Lee, Chung, Chan & Chan, 2005; Twiss, Seaver & McCaffrey, 2006; Wong, López-Nahas, & Molassiotis, 2001).
All of these elements, breathing, suggestion and music form part of the design of Brief Automated Suggestive Relaxation technique (BASR). Its design carries with it the idea of creating a brief and self-applied procedure that permits to obtain results from the outset with minimum effort by both patient and therapist, avoiding, whenever possible, the usually long-term up and down training procedure (Smith, 2001).
Nowadays, cognitive-behavioral multi-component programs are found among first choice treatments for smoking cessation because of their proven effectiveness (Agencia de Evaluación de las Tecnologías Sanitarias, 2003: Becoña, 2003). These programs are characterized by the use of a combined variety of techniques that approach the different factors which help maintain this habit. The Quit Smoking program AIRE (Calvo & Alemán, 2005) is included in this category. Among other procedures, AIRE integrates the above-mentioned BASR brief relaxation technique. This technique is justified within the treatment regimen as a confrontation resource for symptoms of anxiety/craving deriving from nicotine/smoking Withdrawal Syndrome which appears in the first weeks immediately following smoking cessation, and which increases the risk of lapses and relapses.
Finally, it is possible to conclude that if indeed multi-component behavioral programs, as said before, can be considered as well established treatments; the empirical support for all of the techniques that are made up is not the same. Relaxation is, precisely, one of those which has little known evidence to support (Secades & Fernández, 2001). Its possible effectiveness as a treatment for smoking cessation has not been sufficiently studied (Gil, 2003). The present work, a continuation of two previous studies, (Calvo, Alemán, Díaz & Ramal, 2006; Calvo, Betancort & Díaz, 2009), falls under the most extended process of evaluation by AIRE (Calvo & Aleman, 2005), and has as its objective the deepening and consolidating the consistency of the tests which sustain the validity of BASR as a resource within the program, starting from the hypothesis that people who use this technique significantly decrease anxiety, stress and craving (as urgency to smoke) levels when compared to people who use only repose to achieve the same.
Method
Participants
Participants were recruited in the University Smoking Cessation Unit of the University of Las Palmas de Gran Canaria. The presence of mental disorder or its treatment as exclusion criteria and the fact that participants should be daily smokers from at least one year is established. Sixty people voluntarily accepted to participate in the study and were randomly divided into two groups: control group and experimental group. Fifteen did not show up to the appointment or committed errors while filling out the questionnaires. The final sample was composed of 45 Spanish smokers with an average age of 43.91 years (SD =10.43), 55.6% women. The participants' average score on the Fagerström Nicotine Addiction Test was 5.44 (SD =1.28). Eighteen participants were in the control group (CG) and twenty-seven in the experimental group (EG), both with 55.6% women, average age 42.33(SD=11.10) and 44.96 (SD =10.03) respectively. The average level of addiction in the CG was 5.27 (SD=1.22) and in the EG 5.55 (SD=1.33). There were no significant differences between the two groups related to gender (Chi2 (1, 45) = .000, p = 1), average age (t (43) = .825, p= .640) or average level of addiction to nicotine (U Mann-Whitney = 223.5, p = .640).
Instruments
Two standardized tests were used for the evaluation of experimentally-induced anxiety and stress. The Spanish version of the Spielberger, Gorsuch & Lushene Anxiety-State scale (STAI-S) (1970, 1988) was used to determine the state of anxiety (STAI-S). STAI-S evaluated a transitory emotional state, characterized by subjective, consciously perceived feelings of tense attention and apprehension and by hyperactivity of the Autonomous Nervous System. It is composed of 20 phrases with 4 alternative responses from 0-3 (nothing, something, a little, a lot), where the subject shows how he feels in that "exact moment." The range of direct scores is 0-60. The direct scores were transformed according to the Spanish norm-referenced score interpretation from the test manual. The Spanish version of this scale has an internal consistency between .90 and .93. Values of reliability calculated for the process of the two halves reaches .94. The concurrent validity presents values between .88 and .82.
The stress scale from the Differential Stress Inventory of Adjectives for the Study of Moods (Tous & Pueyo, 1991) was used for the evaluation of stress. The stress scale represents distressing feelings of bodily discomfort or negative emotional responses to the demands. This questionnaire is made up of 28 pairs of antonym adjectives situated on the extremes of a 7-point semantic-differential scale (-3 to +3). The direct scores were transformed according to the Spanish norm-referenced score interpretation from the test manual. The stress IDDA-EA scale has a .81 reliability in men and .91 in women. The concurrent validity of the stress scale offers a significant value of .376.
For the evaluation of the urgency to smoke (craving), an analogical qualification Scale of Smoking Desire with 5 degrees of intensity was used ranging from "without need to smoke" to "urgent need to smoke."
The level of physical dependence on tobacco was measured according to the six items of Fagerstrom's Test for Nicotine Dependence (FTND) (Heatherton, Kozlowski, Frecker & Fagerström, 1991) which gives points from 0-10. The Becoña and Vazquez Spanish adaptation was used (1998). These authors consider that a score equal to or greater than 6 indicates high nicotine dependence. The internal consistence coefficient (Cronbach alpha) ranged between .56 and .64. The correlation coefficient in test-retest was .88. The Pearson correlation coefficients in the validity test converge with specific biological measures (cotinine in urine and alveolar CO) were moderate, ranging between .25 and .40 and with the number of years of the smoker an r = .52 was obtained.
Brief Automated Suggestive Relaxation Technique (BASR) contains music based on soft electronic sounds and the sound of the sea, with instructions guiding the listener through a process of relaxation using suggestions of tranquility and calm, concentrating the attention on breathing and inducing a light, slow rhythm and an invitation to dream of an unspecified idyllic setting ("You are in a wonderful place"). For the present work, an audio CD was provided for personal use (Calvo, 2002).
Procedure
The study was carried out using an experimental design of two independent groups: Control (CG) and Experimental (EG). Group assignment was random. The independent variable had two values: application of BASR and rest period with the same conditions as the relaxation situation. Pre and post measurements were taken in three dependent variables: state of anxiety, stress and craving (level of desire to smoke).
Once informed consent was given for participation in the experiment, first data was collected by telephone interview for social demographics, Fagerström test and tobacco consumption. A random appointment to one of the conditions (BASR or rest) was given. To cause anxiety, craving and stress, the participants underwent a period of abstinence before the experiment. This abstinence period was inversely proportional to the degree of physical addiction measured by the Fagerström test. The participants had smoked the last cigarette the previous night and the appointments were scheduled between 3 and 6 hours after waking. So the real abstinence period ranged between ten to fifteen hours.
All participants began by completing the STAI-S Anxiety State scale, the IDDA-EA questionnaire, as well as the analogical Scale of Smoking Desire. According to the group, EG or CG, a pre-programmed 15 minutes relaxation session or a rest session with the same duration. The two conditions were exactly the same, carried out in the same room, with attenuated light and sound, lying down on a lounge chair. The key phrase for the CG was, "Now and during the next 15 minutes, remain lying down comfortably with the lights dimmed for rest." For the EG group, the key phrase was, "Now and during the next 15 minutes, remain lying down comfortably with the lights dimmed while listening to the recording, allowing it to help you relax." After this period, the participants filled out the same questionnaires. By utilizing a recording of BASR on CD, the same session was guaranteed for all of the participants (Calvo 2002).
Statistical analyses
The data were analyzed with the SPSS statistical program version 15. Chi Squared and t average difference tests were done not only on independent samples, but also related samples. A probability of ≤ .05 was considered significant. The scales published in the work of Thalheimer and Cook (2002) were used to evaluate the magnitude of the effect and the percent of change.
Results
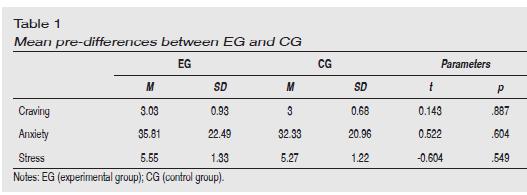
First, research made sure there were no differences in average dependent variables between the two groups. The results of the comparison of measures are shown in Table 1. In all cases the null hypothesis was accepted: There were no significant differences between the groups.
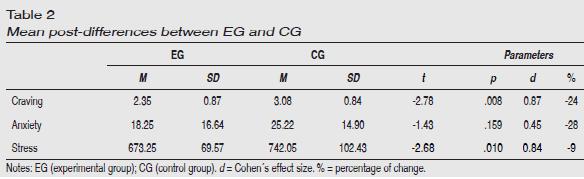
Secondly, the measurements of both groups after the experiment were compared. The results are shown in Table 2. The null hypothesis was rejected in the craving and stress variables, confirming in both a magnitude of "large" and a percentage of change "medium" and "small" respectively. Therefore, major decreases in craving and stress were confirmed in the experimental group. On the other hand, the null hypothesis for the anxiety variable could not be rejected. Though the decrease in anxiety experienced by the experimental group was higher than that in the control group, (the average is visibly lower in the experimental group) and both the size of the effect and the percentage of change had a "medium" magnitude, the difference did not achieve significance.
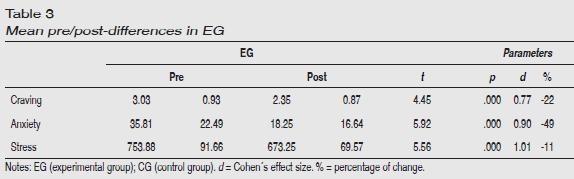
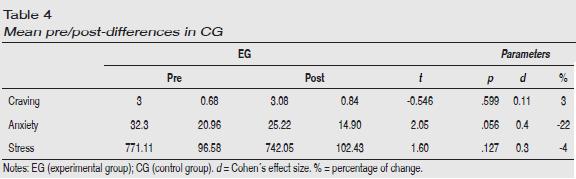
In tables 3 and 4 intra-group comparisons are shown between the pre and post phases. While the EG present significant differences in all measured dependent variables (Table 3), the CG did not reach significance in any of the comparisons (Table 4). In all the comparisons, both in the size of the effect as well as in the percentage of change, the EG showed higher figures than the CG. The value of Cohen d is "large" in all the differences in the EG and "negligible" in all those of the CG. The percentage of change in craving, anxiety, and stress was "medium", "large" and "small" respectively for the EG and "negligible," "medium" and again "negligible" respectively for the CG.
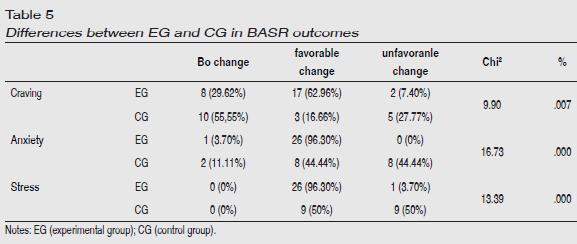
Results were grouped in three categories: favorable change (obtain a decrease in levels of craving, anxiety and stress), unfavorable change (an increase in said levels) and no change. The distribution of data can be seen in Table 5. These results underwent a Chi Squared test to evaluate the distribution differences in both groups, EG and CG. In all cases the distribution differences were significant (craving, Chi2 (45, 2) = 9.90, p= .007; anxiety, Chi2 (45, 2)= 16.73, p= .000; stress, Chi2 (45, 1)= 13.39, p= .000), such that the proportion of participants that showed favorable changes was always superior in the EG and, on the other hand, the larger proportion of unfavorable changes were found in the CG.
Discussion
As in previous studies (Calvo et al., 2006; Calvo et al., 2009), BASR, compared to a control situation, shows a higher index of deactivation (mostly significant) in dependent variable measurements, verifying a high probability of favorable results for the EG in all of the work. Compared to a previous work (Calvo et al., 2006) we saw that while in the CG none of the smokers experienced a decrease in the intensity of craving, and had an increase in 23% of the cases (27.77% in the current study), in the EG 64.3% of the participants (62.96% in the current work) experienced a decrease in craving, the significant mean between them (p= .025), which was also significant in the current replication of the study (p= .008). The size of the effect was "large" and the percentage of change "medium," exactly the same as in the current study. In 100% of the EG subjects (96.30% in the current work), a decrease in stress levels was produced, and the differences between the groups were significant in both works (p = .011 and p = .010 respectively). It is notable that there was a 61.54% increase in stress (50% in the current work) in the CG. The size of the effect and the percentage of change were "very large," and "large" respectively, somewhat higher than in the present work which were "large" and "small" respectively. In relation to post anxiety, the difference between the CG and the EG was significant (p= .007), with a size effect of "very large" but a percentage of change "small." In the present work, significance was not obtained in the difference in post-anxiety measurements; however, there was a "medium" magnitude in both the size of the effect and the percentage of change. Anxiety decreased in the EG in all cases (somewhat less than in the current work, 96.3%), and in the CG 61.54% (44% in the current work) of the subjects experienced an increase in anxiety. The pre-post differences in the EG were also highly significant as in the present work and, as we have found now, the pre-post differences in the CG were not significant in terms of anxiety and stress (nor in the current work for craving), although yes for craving, however, because in this case craving increased in the CG after rest. In brief, we have obtained quite similar results in the current work in regard to pre-post comparisons and in the distribution of the favorable/unfavorable results and slightly lower in post comparisons.
We must point out that in anxiety no participant in the EG experienced adverse effects and only two people in craving and one in stress reported unfavorable effects. This paradoxical effect, induced by relaxation, is not a new phenomenon, and has been previously described, with possible explanations such as fear of losing control, the loss of internal locus of control, or fear of somatic anxiety keys, especially in people predisposed to generalize anxiety (Braith, McCullough & Bush 1988; Heide & Borkovec, 1984; Wegner, Bromme & Blumberg, 1997). In our study, one patient commented at the end of one of the sessions that the sounds of the sea, which form part of the musical background, reminded him of a family accident. It was impossible for her to relax.
The previous work (Calvo et al., 2009) was not carried out on smokers but rather on a sample of university students. The source of stress was not abstinence, but rather the recurrence of a recent personal, stressful event. Anxiety state as well as cardiac frequency were measured as dependent variables. Post-significant differences between the EG and CG were therefore confirmed for anxiety, but not in cardiac frequency; the size of the anxiety effect "large." There were also significant pre-post differences in both groups, but the effect size was higher in the EG. The qualification was "huge" in the EG as opposed to "medium" in the CG, with a more relevant clinical significance. This established difference, speaking of anxiety, in both works, suggests that BASR has a differential behavior according to the sources of anxiety/stress and/or the type of user. This result is in line with the Smith ABC theory (Amutio, 2006; Smith, 2001).
Considering the meta-analyses done by Eppley, Abrams and Shear (1989), Manzoni, Pagnini, Castelnuovo and Molinari, (2008) and Öst (1987), we see that the general efficacy of the training in some type of relaxation technique (Progressive Muscular Relaxation, Autogenic Training, Applied Relaxation, Meditation, Benson Relaxation and other techniques) for the management of anxiety, expressed as effect size, is of a "medium" level (between 0.43 and 0.57). If we compare the results of our work with these, BASR has the same level of efficacy.
In relation to stress, it was found, in post comparisons between groups, effect sizes from "medium" (Pawlow & Jones, 2005; Pawlow, O'Neill, & Malcolm, 2003) with Brief Progressive Muscular Relaxation, to "huge" with Applied Relaxation (Bastani, Hidarnia, Kazemnejad, Vafaei, & Kashanian, 2005) and Progressive Muscular Relaxation (Sheu, Irvin, Lin, & Mar, 2003). In pre-post comparisons in the experimental group we found "medium" level effects (Pawlow et al., 2003), "very large" (Bastani et al., 2005) and "huge" (Pawlow & Jones, 2005). Remember that in our work we confirmed a "large" effect size in post comparison between the CG and EG as well as the pre-post comparison in the EG. Therefore, we consider that BASR is within the framework of the relaxation techniques, with a demonstrated efficacy for the management of stress. As for the studies on relaxation focused on the control of craving, studies have been done with Controlled Deep Breathing and Body Scan Technique. It has been confirmed that Controlled Deep Breathing alleviates symptoms of abstinence and significantly reduces levels of craving, with an effect size of "huge" (McClernon et al., 2004) in the post CG vs. EG comparison. Body Scan Technique has also been shown to have a reducing effect on craving, with an effect size of "medium" (Cropley et al., 2007) in the post comparison CG versus EG, and "huge" in the pre-post comparison in the EG (Ussher et al., 2009). BASR obtains a "large" effect size in the post as well as the pre-post, within range of the above-mentioned studies.
In conclusion, in agreement with findings, a positive effect and the efficacy of the technique employed for the control of craving, anxiety and stress in smokers is corroborated. Evidence is therefore added, along with that of previous works (Calvo et al., 2006; Calvo et al., 2009), for the clinical utility of Brief Automated Suggestive Relaxation BASR. Nevertheless, additional studies are needed to clarify some aspects, such as the specific pattern for R-State attributable to BASR, effects of longer-term self-training or its possible use for other situations and patients and also improving the assessment of craving with a questionnaire adapted to Spanish population.
References
Agencia de Evaluación de las Tecnologías Sanitarias (AETS), Instituto de Salud Carlos III, Ministerio de Sanidad y Consumo (2003, septiembre). Evaluación de la eficacia, efectividad y coste-efectividad de los distintos abordajes terapéuticos para dejar de fumar. Madrid: AETS-Instituto de Salud Carlos III. [ Links ]
Allen, S. S., Bade, T., Hatsukami, D., & Center, B. (2008). Craving, withdrawal, and smoking urges on days immediately prior to smoking relapse. Nicotine & Tobacco Research, 10(1), 35-45. [ Links ]
American Psychiatric Association (2003). Manual diagnóstico y estadístico de los trastornos mentales, DSM-IV-TR. Barcelona: Masson. [ Links ]
Amutio, A. (2002a). Relajación y emociones positivas. Ansiedad y Estrés, 8, 59-71. [ Links ]
Amutio, A. (2002b). Estrategias de manejo del estrés: el papel de la relajación. Cuadernos de Medicina Psicosomática y Psiquiatría de Enlace, 62/63, 19-31. [ Links ]
Amutio, A. (2006). Relajación y meditación. Un manual práctico para afrontar el estrés. Madrid: Biblioteca Nueva. [ Links ]
Bastani, F., Hidarnia, A., Kazemnejad, A., Vafaei, M., & Kashanian, M. (2005). A randomized controlled trial of the effects of applied relaxation training on reducing anxiety and perceived stress in pregnant women. Journal of Midwifery & Womens Health, 50(4), 36-40. [ Links ]
Becoña, E. (2003). El tratamiento de la adicción a la nicotina. Papeles del Psicólogo, 24, 48-69. [ Links ]
Becoña, E. & Vázquez, F.L. (1998). Tratamiento del tabaquismo. Madrid: Dykinson. [ Links ]
Braith, J.A., McCullough, J.P. & Bush J.P. (1988). Relaxation-induced anxiety in a subclinical sample of chronically anxious subjects. Journal of Behavior Therapy and Experimental Psychiatry. 19(3), 193-198. [ Links ]
Brown, R. A., Lejuez, C. W., Kahler, C. W., Strong, D. R., & Zvolensky, M. J. (2005). Early lapse following smoking cessation: Relationship to negative affect and distress tolerance. Clinical Psychologycal Review, 25, 713-733. [ Links ]
Calvo, F. (2002). Relajación sugestiva (CD). Las Palmas de Gran Canaria, Colegio Oficial de Psicólogos. D.L.: GC-635-2002. [ Links ]
Calvo, F. & Alemán, J.M. (2005). Programa de Deshabituación Tabáquica A.I.R.E. (Aprendizaje Integrado de Recursos Estratégicos). Colegio Oficial de Psicólogos De Las Palmas: Las Palmas de Gran Canaria. [ Links ]
Calvo, F., Alemán, J.M., Díaz, M.D. & Ramal, J. (2006). Validación de una técnica de relajación automatizada para fumadores en tratamiento de deshabituación. VI Congreso Internacional de la Sociedad Española para el Estudio de la Ansiedad y el Estrés. Benidorm, 21-23 de Septiembre de 2006. [ Links ]
Calvo, F., Betancort, E. & Díaz, M.D. (2009). La técnica de relajación sugestiva breve automatizada: ampliación del estudio de su eficacia a una muestra de universitarios. Ansiedad y Estrés, 15(2-3), 119-130. [ Links ]
Cami, J. & Farré, M. (2003). Drug addiction. New England Journal of Medicine, 349, 975-986. [ Links ]
Chambless, D.L. & Ollendick, T.H. (2001). Empirically supported psychological interventions: controversies and evidence. Annual Review of Psychology, 52, 685-716. [ Links ]
Conde Pastor, M. & Menéndez, F. J. (2000). Estudio experimental sobre el parámetro de frecuencia respiratoria más adecuado para conseguir disminuir la activación psicofisiológica. Ansiedad y Estrés, 6, 153-167. [ Links ]
Cropley, M., Ussher, M., & Charitou, E. (2007). Acute effects of a guided relaxation routine (bodyscan) on tobacco withdrawal symptoms and cravings in abstinent smokers, Addiction, 102, 989-93. [ Links ]
Eppley, K.R., Abrams, A.I., & Shear, J. (1989). Differential effects of relaxation techniques on trait anxiety: a meta-analysis. Journal of Clinical Psychology, 45(6), 957-974. [ Links ]
Fernández-Abascal, E.G. & Miguel, J.J. (1979). Medidas de respiración en diferentes técnicas de relajación. Informes del Departamento de Psicología General, 2, 127-142. [ Links ]
Fernández-Abascal, E.G. & Miguel, J.J. (1980). Medidas dermoeléctricas en diferentes técnicas de relajación. Informes del Departamento de Psicología General, 3, 209-220. [ Links ]
Gil, J. (2003). Guía de tratamientos psicológicos eficaces en el tabaquismo. In M. Pérez, J. R., Fernández, C. Fernández & I. Amigo, I. (Eds.), Guía de tratamientos psicológicos eficaces. Volumen II: Psicología de la Salud (pp. 287-353). Madrid: Pirámide. [ Links ]
González-Ordi, H. & Miguel-Tobal, J.J. (1998). Estrategias de sugestión en el manejo de la activación psicofisiológica: El efecto de las instrucciones y el nivel de sugestionabilidad. Ansiedad y Estrés, 4, 281-298. [ Links ]
Heatherton, T.F., Kozlowski, L.T., Frecker, R.C., & Fagerström, K.O. (1991). The Fagerström Test for Nicotine Dependence: A revision of the Fagerström Tolerance Questionnaire. British Journal of Addiction, 86, 1119-1127. [ Links ]
Heide, F.J. & Borkovec, T.D. (1984). Relaxation-induced anxiety: mechanics and Theoretical implications. Behavior, Research and Therapy, 22(1), 1-12. [ Links ]
Hendricks, P.S., Ditre, J.W., Drobes, D.J. & Brandon, T.H. (2006). The early time course of smoking withdrawal effects. Psychopharmacology, 187(3), 385-396. [ Links ]
Hughes, J.R. (2007). Effects of abstinence from tobacco: valid symptoms and time course. Nicotine Tobacco Research, 9(3), 315-327. [ Links ]
Hughes, J.R., Higgins, S.T. & Bickel, W. (1994). Nicotine withdrawal versus other drug withdrawal syndromes: similarities and dissimilarities, Addiction, 89, 1461-1470. [ Links ]
Hughes, J. R., Higgins, S. T., & Hatsukami, D. (1990). Effects of abstinence from tobacco: A critical review. In L. T. Kowzlowski & H. M. Annis (Eds.), Recent advances in alcohol and drug problems (Vol. 10, pp. 317-398). New York: Plenum. [ Links ]
Iraurgi, I. & Corcuera, N. (2008). Craving: concepto, medición y terapéutica. Norte de Salud Mental, 32, 9-22. [ Links ]
Jaber, S., Bahloul, H., Guétin, S., Chanques, G., Sebbane, M., & Eledjam, J.J. (2007). Effects of music therapy in intensive care unit without sedation in weaning patients versus non-ventilated patients. Annales Françaises d'Anesthésie et de Réanimation, 26, 30-38. [ Links ]
Lara, G., Ramírez, A., Sansores, R.H., Espinosa, A.M. & Regalado, J. (2007). Indicadores de síntomas de abstinencia en un grupo de fumadores mexicanos. Salud Pública de México, 49(sup 2), 257-262. [ Links ]
Lee, O.K., Chung, Y.F., Chan, M.F. & Chan, W.M. (2005). Music and its effect on the physiological responses and anxiety levels of patients receiving mechanical ventilation: A pilot study. Journal of Clinical Nursing, 14, 609-620. [ Links ]
Lichstein, K.L. (1988). Clinical Relaxation Strategies. New York: Wiley. [ Links ]
Manzoni, G.M., Pagnini, F., Castelnuovo, G., & Molinari, E. (2008). Relaxation training for anxiety: a ten-years systematic review with meta-analysis. BMC Psychiatry, 8(41). Advance online publication. DOI: 10.1186/1471-244X-8-41. [ Links ]
McClernon, F. J., Westman, E. C., & Rose, J. E. (2004). The effects of controlled deep breathing on smoking withdrawal. Addictive Behaviors, 29, 765-772. [ Links ]
Natham, P.E. & Gorman, J.M. (Eds.) (1998). A Guide to Treatments That Work. New York: Oxford University Press. [ Links ]
Office of the U.S. Surgeon General. (1988). Nicotine addiction. Washington, DC: U.S. Government Printing Office. [ Links ]
Organización Mundial de la Salud (2003). Clasificación Estadística Internacional de Enfermedades y Problemas Relacionados con la Salud, Décima Revisión. Washington, D.C.: Organización Panamericana de la Salud. [ Links ]
Öst, L.G. (1987). Applied relaxation: Description of coping technique and review of controlled studies. Behavior, Research and Therapy, 25, 397-409. [ Links ]
Parrott, A.C. (1999). Does Cigarette Smoking Cause Stress? American Psychologist, 54, 817-820. [ Links ]
Parrott, A. C, Garnham, N. J., Wesnes, K., & Pincock, C. (1996). Cigarette smoking and abstinence: Comparative effects upon cognitive task performance and mood state over 24 hours. Human Psychopharmacology, 11, 391-400. [ Links ]
Pawlow. L.A. & Jones, G.E., (2005). The Impact of Abbreviated Progressive Muscle Relaxation on Salivary Cortisol and Salivary Immunoglobulin A (sIgA). Applied Psychophysiology and Biofeedback, 30(4), 375-387. [ Links ]
Pawlow, L. A., O'Neil, P. M., & Malcolm, R. J. (2003). Night eating syndrome: effects of brief relaxation training on stress, mood, hunger, and eating patterns. International Journal of Obesity 27, 970-978. doi:10.1038/sj.ijo.0802320. [ Links ]
Pérez, M. & Fernández, J.R. (2001). El grano y la criba de los tratamientos psicológicos. Psicothema, 13(3), 523-529. [ Links ]
Piasecki, T.M. (2006). Relapse to smoking. Clinical Psychology Review, 26, 196-215. [ Links ]
Ponce, A.N., Lorber, W., Paul, J.J., Esterlis, I., Barzvi, A., Allen, G.J., & Pescatello, L.S., (2008). Comparisons of Varying Dosages of Relaxation in a Corporate Setting: Effects on Stress Reduction. International Journal of Stress Management, 15(4), 396-407. [ Links ]
Quesada, M., Carreras, J.M., & Sánchez, L. (2002). Recaída en el abandono del consumo de tabaco: una revisión. Adicciones, 14(1), 65-78. [ Links ]
Rosa, A.I., Olivares, J. & Sánchez-Meca, J. (1998). Efectos diferenciales de las técnicas de relajación sobre la ansiedad: Una revisión meta-analítica. Ansiedad y Estrés, 4, 97-110. [ Links ]
Sánchez-Meca, J., Rosa, A.I., & Olivares, J. (1998a, julio). Eficacia diferencial de los diferentes tipos de relajación en problemas de salud: un estudio meta-analítico en España. Comunicación presentada al II Congreso Iberoamericano de Psicología. Madrid: Colegio Oficial de Psicólogos. [ Links ]
Sánchez-Meca, J., Rosa, A.I., & Olivares, J. (1998b). Las técnicas de relajación en el campo clínico y de la salud en España: Una revisión meta-analítica. Cuadernos de Medicina Psicosomática, 45-46, 21-36. [ Links ]
Schachter, S. (1978). Pharmacological and psychological determinants of smoking. In R. E. Thornton (Ed.), Smoking behavior: Physiological and psychological influences (pp. 208-228). Edinburgh: Churchill-Livingstone. [ Links ]
Secades, R. & Fernández, J.R. (2001). Tratamientos psicológicos eficaces para la drogadicción, nicotina, alcohol, cocaína y heroína. Psicothema, 13, 365-380. [ Links ]
Shadel, W.G., Niaura, R., Brown, R.A., Hutchinson, K.E. & Abrams, D.B. (2001). A content analysis of smoking craving, Journal of Clinical Psychology, 57(1), 145-150. [ Links ]
Sheu, S., Irvin, B. L., Lin, H. S., & Mar, C. L. (2003). Effects of progressive muscle relaxation on blood pressure and psychosocial status for clients with essential hypertension in Taiwan. Holistic Nursing Practice, 17(1), 41-48. [ Links ]
Shiffman, S. (2000). Comments on craving. Addiction, 95, S171-S175. [ Links ]
Smith, J.C. (2001). Entrenamiento ABC en Relajación: Una guía práctica para los profesionales de la salud. Bilbao: Descleé de Brouwer. [ Links ]
Smith, J.C., Amutio, A., Arteaga, J.P. & Aria, L.A. (1996). Relaxation: Mapping an uncharted world. Biofeedback and Self-Regulation, 21, 63-90. [ Links ]
Spielberger, C.D., Gorsuch, R.L., & Lushene, R.E. (1970). STAI Manual for the State Trait Anxiety Inventory (Self Evaluation Questionnaire). Palo Alto California: Consulting Psychology Press. [ Links ]
Spielberger, C.D., Gorsuch, R.L., & Lushene, R.E. (1988). Cuestionario de Ansiedad Estado-Rasgo. Madrid: Tea Ediciones. [ Links ]
Thalheimer, W., & Cook, S. (2002, August). How to calculate effect sizes from published research: A simplified methodology [Portable Document File version]. A Work-Learning Research Publication. [ Links ]
Teneggi, V., Tiffany, S.T., Squassante, L., Milleri, S., Ziviani, L. & Bye, A. (2002). Smokers deprived of cigarettes for 72 h: Effect of nicotine patches on craving and withdrawal. Psychopharmacology, 164(2), 177-187. [ Links ]
Tobacco Advisory Group of the Royal College of Physicians (2000). Psychological effects of nicotine and smoking in man, en Tobacco Advisory Group of the Royal College of Physicians (Eds.) Nicotine Addiction in Britain (pp. 67-78). London: Royal College of Physicians of London. Retrieved from http://www.rcdoplondon.ac.uk/pubs/books/nicotine/3-psychol.htm. [ Links ]
Tous, J.M. & Pueyo, A.A. (1991). Inventario Diferencial de Adjetivos para el Estado de Ánimo. Madrid: TEA Ediciones. [ Links ]
Twiss, E., Seaver, J. & McCaffrey, R. (2006). The effect of music listening on older adults undergoing cardiovascular surgery. Nursing Critical Care, 11, 224-231. [ Links ]
Ussher, M., Cropley, M., Playle, S., Mohidin, R., & West, R. (2009). Effect of isometric exercise and body scanning on cigarette cravings and withdrawal symptoms. Addiction, 104, 1251-1257. [ Links ]
Wegner, D.M., Broome, A. & Blumberg, S.J. (1997). Ironic effects of trying to relax under stress. Behavior Research and Therapy. 35(1), 11-21. [ Links ]
West, R. & Hajek, P. (1997). What happens to anxiety levels on giving up smoking? American Journal of Psychiatry, 154(11), 1589-1592. [ Links ]
Woolfolk, R.L., Lehrer, P.M., McCann, B.S., & Rooney, A.J. (1982). Effects of progressive relaxation and meditation on cognitive and somatic manifestations of daily stress. Behaviour Research and Therapy 20(5), 461-467. [ Links ]
Wong, H.L., Lopez-Nahas, V., & Molassiotis, A. (2001). Effects of music therapy on anxiety in ventilator-dependent patients. Heart Lung, 30, 376-387. [ Links ]
Zvolensky, M.J.,Feldner, M.T. Eifert, G.H. & Brown, R.A. (2001). Affective style among smokers: understanding anxiety sensitivity, emotional reactivity and distress tolerance using biological challenge. Addictive Behaviors, 26, 901-915. [ Links ]
