










Services on Demand
Journal
Article
 Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Latinoamericana de Psicología
Print version ISSN 0120-0534
rev.latinoam.psicol. vol.45 no.1 Bogotá Jan./Apr. 2013
Prediction of Post-Traumatic Stress Symptoms via Comorbid Disorders and other Social and School Problems in Earthquake Exposed Turkish Adolescents
Predicción de síntomas de estrés post-traumático por trastornos comórbidos y otros problemas sociales y escolares en adolescentes expuestos a un terremoto en Turquía
Sefa Bulut
Abant Izzet Baysal University, Turkey
Correspondence to: Sefa Bulut, Abant Izzet Baysal University, College of Education. Department of Guidance and Psychological Counseling. Bolu 14280 Turkey. E mail: sefabulut22@hotmail.com
Recibido: Diciembre de 2012 Revisado: Enero de 2013 Aceptado: Abril de 2013
Abstract
On May 3rd, 2003, a strong earthquake hit the eastern part of Turkey at 03:27 a.m. and lasted 20 seconds. It destroyed a regional boarding school killing 83 students and 1 teacher. Disaster-exposed children are at risk for a variety of mental health, social, and academic problems. This research was designed to investigate the extent of comorbidity among adolescent earthquake survivors. One hundred and ninety-one adolescents were given the Child Post Traumatic Stress Reaction Index and the Behavior Assessment Systems one year after the earthquake. The adolescents were divided into PTSD (Post Traumatic Stress Disorder) positive and non PTSD groups. Multivariate ANOVAs were then conducted to test group and gender differences on the BASC subscales. Correlation analysis revealed some significant associations between the CPTSD RI and BASC subscales. Multiple stepwise regression analysis was used to predict the contribution of each of the BASC SRP A subscales. Depression was the strongest contributor, accounting for 23% of the total variance. The next most significant contributing variable was atypicality, at 6%. This was followed by sensation-seeking, with a 4% variance. Finally attitude to school added another 2% to the prediction for PTSD. These four variables, together, explained 35% of the variance in the CPTSD RI total score (r.585, r²=.35 p<.05). Those variables also correlated with the CPTSD RI subscales of re-experiencing, avoidance and hyperarousal. Cross- cultural implications were also discussed in reference to the disaster and other disorders.
Key words: Comorbid disorder of PTSD, Anxiety and Depression, Predictors of PTSD, Comprehensive Assessment of Survivors.
Resumen
El 3 de mayo de 2003 un fuerte terremoto de 20 segundos golpeó Turquía del este a las 3:27 de la madrugada, éste destruyó un internado regional en donde 83 estudiantes y 1 maestro fallecieron. Los niños expuestos a desastres están en riesgo sufrir una variedad de dificultades con respecto a su salud mental, así como problemas sociales y académicos. El propósito de este estudio fue evaluar el grado de comorbilidad entre los adolescentes sobrevivientes al terremoto. Un año después de la catástrofe 191 adolescentes completaron el Índice de Reacción de Desorden de Estrés Postraumático en Niños CPTSD y el Sistema de Evaluación de Conducta BASC. Estos adolescentes fueron divididos en grupos de PTSD (Desorden de Estrés Postraumático) positivo y grupos que no presentaban PTSD. De esta manera, se llevaron a cabo análisis de varianza ANOVA para probar las diferencias de grupo y de género en las subescalas BASC (Sistema de Evaluación de Conducta para Niños). El análisis de correlación reveló algunas asociaciones significativas entre el CPTSD RI y las subescalas BASC. Múltiples análisis de regresión stepwise (paso a paso) fueron utilizados para predecir la contribución de cada una de las subescalas BASC SRP A. La depresión fue el mayor contribuyente, lo que representa el 23% de la varianza total. La siguiente variable que contribuye significativamente fue atípica al 6%. Esto fue seguido por la búsqueda de sensaciones, con una variación del 4%. Por último, la actitud hacia la escuela añadió un 2% a la predicción para el PTSD. Estas cuatro variables juntas explicaron el 35% de la varianza de la puntuación total del CPTSD RI (r.585, r2=.35 p<.05). Estas variables también se correlacionan con las subescalas de RI CPTSD de re-experimentación, evitación e hiperexcitación. Las implicaciones transculturales también fueron discutidas en referencia a la catástrofe y otros trastornos.
Palabras clave: Trastorno comórbido de PTSD, Ansiedad y depresión, Predictores de PTSD, Evaluación comprensiva de sobrevivientes.
Disasters are natural phenomena that can unexpectedly happen at any time, and in any place. In the last decade, large number of natural disasters took place in different parts of the world causing the loss of a significant number of human lives, destruction of property, and disruption of social networks. Traditionally, disasters, whether natural, technological or man-made, have been studied for their effects on post traumatic stress. Very little attention has been paid to mental health problems other than PTSD. Trauma studies can be grouped into 3 categories in terms of their effects on the victims. The first group is focused on the epidemiologic factors (McFarlane, 1987) and prevalence (Bulut, 2006, 2009, 2010; Bulut, Bulut, & Tayli 2005; Kun, Han, Chen, & Yao, 2009; McFarlane, Policansky, & Irwin, 1987), with the aim of researching the psychological post-effects and the mental health problems that arise, most of these being PTSD. The second body of research concentrated on assessment issues (Cordova, Studts, Hann, Jacobsen, & Andrykowski, 2000; Foa, Riggs, & Gershuny, 1995) and focused on the instruments of trauma and their structures, as well as their psychometric properties. The third area of research aimed to identify comorbid disorders (Hubbard, Realmuto, Northwood, & Masten, 1995; Shalev et al., 1998), school problems (La Greca, Silverman, & Wasserstein, 1998; McFarlane et al., 1987), and other personal and social adjustment problems (Famularo, Fenton, Augustyn, & Zuckerman, 1996; Maida, Gordon & Straus, 1993). Following the calamity. There are also few studies which paid attention to physical health related problems (Dollinger, 1986; Llabre & Hadi, 1997; McFarlane et al., 1987) that emerged after the disasters. On the other hand, some of the studies also focused on longitudinal progress of PTSD and its subsympthoms (Bulut, 2010).
Most of the studies were conducted with one or two screening instruments, and they mostly aimed to identify post traumatic stress in a trauma exposed population. Anxiety (La Greca et. al., 1998; Lonigan, Shannon, Finch, Daugherty, & Taylor, 1991) and depression (Goenjian et al., 2001; Llabre & Hadi, 1997) are, together, the second, and most often studied concepts after PTSD; for this reason, anxiety and depression scales are frequently used as screening tools in trauma research (Karabekiroğlu, Akbas, Taşdemir, & Karakurt, 2008; Sabin, Lopes, Nackerud, Kaiser, & Varese, 2003).
However, only few studies have investigated PTSD, and other comorbid disorders, with a broad range of instruments. This is essential to an understanding of the construct and epidemiology of PTSD. However, a few earlier studies did attempt to use more comprehensive tools: For example, Shaw et al. (1995) utilized Achenbach's Teacher Report Form with elementary school pupils; Braun-Lewensohn, Clestin-Westreich, Clestin, Verté and Ponjaert-Kristofersen (2009) used Achenbach's Youth Self-Report and Brief Symptom Inventory with adolescents; McFarlane et al. (1987) administered the parent and teacher form of the Rutter Questionnaire in order to assess school age children's reactions; Hubbard et al. (1995) employed the Structured Clinical Interview of the DSM Axis 1 disorder; Green et al. (1994) used the Psychiatric Evaluation Form and Symptom Checklist 90; Sabin et al. (2003) used the Hopkins' Symptom Checklist with an adult population. Most recent studies have tended to use multiple and more comprehensive tools for possible PTSD and other comorbid disorders (Kim, 2009). It is well established that traumatic events not only cause PTSD reactions and mental health problems, but also affect children's and adolescents' social and academic domains as well. It is therefore imperative to conduct a global compressive assessment, and screening with a multidimensional instrument, with trauma-exposed vulnerable populations. This current study aimed to fill a gap in the literature by assessing for other possible comorbid disorders and adjustment problems that can emerge after a significant traumatic incident.
Even a severe post traumatic stress disorder is listed under Anxiety Disorders in the DSM IV (Diagnostic and Statistical Manual of Mental Disorders, fourth edition) nomenclature, although its symptom structure indicates very diverse symptom groups. Some authors have criticized the heterogeneous construct of PTSD, and the large number of possible diagnostic criteria in some of the symptom groups (Foa et al., 1995). Jenkins and Baird (2002) argue, in a similar vein, that some of the sub-symptoms of PTSD, in particular avoidance (a C criterion), is not readily applicable to all cultures, and that some of the concepts do not exist at all, or else are not very well understood, in some parts of the world.
Furthermore, Kar and Murali (2001) argue that the criteria for PTSD, as used for adults, may be less sensitive if used to detect the disorder in children, so that PTSD in children may be missed due to the application of inappropriate criteria. A factor analysis of various PTSD instruments yields different symptom structures, but all of them, without exception, demonstrate a very heterogeneous construct (Bulut, 2003; Evans, 2002). Comorbidities and sub-clinical syndromes are commonly observed in conjunction with PTSD (Kar, 2009). Anxiety and depressive symptoms are the most common. The current DSM IV PTSD symptom clusters include many symptoms of anxiety and depression. There is an ongoing discussion about the symptom composition of PTSD and mental health experts therefore recommend a revision of PTSD symptoms for the new DSM V (Bulut, 2003, 2010; Tol et al., 2009).
On May 3rd, 2003, an earthquake of 6.4 on the Richter scale hit the eastern part of Turkey at 03:27 a.m. It lasted for 20 seconds and destroyed a regional boarding school, killing 83 students and 1 teacher. Many of the students lost their friends, and were trapped under the rubble for days. The four storey residential building had collapsed in a pan-cake style, and children were saved between the storeys by the presence of steel shelves and bunk beds. One hundred and fifteen children were rescued, some having survived for days.
Bingöl is located in the eastern part of Turkey and has a rural character. The city of Bingöl was severely damaged by the earthquake. Bingöl's community centers, schools, hospitals, business buildings and other government buildings were, to a large extent, destroyed. The disaster completely destroyed 10 buildings, killing 176 people and leaving another 520 people injured.
The magnitude of the disaster was so great, and the post-disaster living conditions so adverse, that it was highly likely that children exposed to such an earthquake would develop PTSD and other comorbid disorders, as well as personal, school and social adjustment problems. The purposes of this study were therefore: (1) to examine for possible occurrence of comorbidity with PTSD, (2) to investigate the strength of association between the BASC sub-scales and the CPTSD RI subscales and total scores, (3) to identify the predictive power of PTSD for comorbid disorders, (4) to compare PTSD and non-PTSD groups on the sub-scales of BASC, (5) to look for gender differences on the BASC SRP A form, and finally (6) to test the appropriateness of the BASC SRP Adolescent form as a multidimensional assessment tool in screening adolescents' reactions.
Method
Subjects
As part of a broader, longitudinal research project, data was collected from a large number of students, at both elementary and secondary levels. However, in order to have a more homogenous group for this research project, only secondary school students who are all adolescents, were included in the statistical analysis. Among the 205 students, 14 of them left blank some of the items in the instruments, and were therefore excluded from the data analysis so that ultimately a total of 191 secondary school students took part in the study The adolescent groups were composed of 72 students in the 6th grade (38%), 66 students in the 7th grade (34%), and 53 students in the 8th grade (28%). There were 37 girls (19%) and 154 boys (81%), with a mean age of 13.43 and a standard deviation of 1.44.
The Governorship of Bingöl Province and the Board of Education were contacted, and the intention of this research was explained to them in a written petition that included the survey packages. Upon receiving their permission, consent forms were sent to homes in order to inform children's families of the nature and scope of the study, and permission was requested for the children to participate. The children were also given a consent form, and the purpose of this study, as well as the procedures involved, were explained to them. They were told that participation was voluntary and that confidentiality was guaranteed. They were told that this information would be used to help themselves, and also other children who had experienced similar traumatic events.
The data set was screened for outliers, missing items and was checked for the ANOVA and MANOVA assumptions of normality, linearity, and homoscedasticity of the residuals. There was no violation of any of these assumptions. Multicollinearity between variables was also not a problem. All of the necessary univariate and multivariate assumptions were satisfied for the statistical procedures employed in this research. A set of correlations, Multivariate ANOVAs and Multivariate Regression Analyses were employed in the data analysis. After entering information from the research protocol forms into the SPSS program they were shredded and destroyed in order to protect the confidentiality of the individuals. The data was then saved and stored in a computer to which only the investigator had access, and for which a pin number was required.
Instruments
The Behavior Assessment System for Children. The Behavior Assessment System for Children (BASC) is designed to facilitate the differential diagnosis and educational classification of a variety of emotional and behavioral disorders on children, and to assist in their treatment plans (Reynolds & Kamphaus, 1992). The manual reports that BASC makes differential diagnoses, corresponding to the Diagnostic and Statistical Manual of Mental Disorders, third edition (DSM-III-R). The BASC is an integrated assessment system consisting of a self-report, a teacher rating scale, a parent rating scale, a developmental history, and an observation protocol, all designed to assess children for the differential diagnosis and educational treatment of emotional and behavioral disorders. The instrument focuses on both adaptive and maladaptive behavior, and different sources and methods are utilized to provide an estimate of functioning (Sandoval & Echandia, 1994). There are two age levels for the BASC-SRP, child (8-11) and adolescent (12-18). In this study, the BASC-SRP (Self Report Protocol) adolescent forms were used. The BASC-SRP combines the child's own statements regarding emotional well-being and self-perception. The SRP takes about 15 minutes to complete. The items are those common to omnibus personality inventories requiring a true-false response (Merenda, 1996). The child level of the BASC has 12 scales and the adolescent level (SRP-A) 14 scales. The SRP is composed of Anxiety, Atypicality, Locus of Control, Social Stress, Attitude to School, Attitude to Teachers, Depression, Sense of Inadequacy, Relations with Parents, Interpersonal Relations, Self-Esteem, and Self-Reliance. The BASC-SRP also yields composite scores in School Maladjustment (Attitude to School, Attitude to Teachers), Clinical Maladjustment (Anxiety, Atypicallity, Locus of Control, Social Stress), and Personal Adjustment (Relations with Parents, Interpersonal Relations, Self-Reliance, Self-Esteem), and an overall score, the Emotional Symptoms Index (ESI), which is a global indicator of emotional well-being. The ESI has both negative scales (clinical) and positive scales (adaptive). The scales can be interpreted with reference to national (US) age norms (General, Male, and Female) or to clinical norms. Special indices are designed to assess the validity of the child's responses: These indices are the F index, the "fake good" index, for SRP-Adolescents only, and the V index, which is designed to detect invalid responses that may be due to poor reading comprehension, failure to follow directions, or poor contact with reality (Reynolds & Kamphaus, 1992). The BASC is available in paper/pencil, computerized, and audiotape forms (Flanagan, 1995). In this study, data were collected in a traditional paper/pencil format but were analyzed by computer. It takes less than 2 minutes to enter items and to get a print-out with subscale graphs. Another reason for selecting the BASC was the suggestion that it is a good screening instrument for children's and adolescents' social skill functioning (Flanagan, Alfonso, & Primavera, 1996).
Validity of BASC-SRP. The BASC-SRP was normed on 5,413 children ages 8-11, on 2,944 children ages 12-14, and on 1,540 adolescents ages 15-18 (Reynolds & Kamphaus, 1992). It has been correlated with other standardized instruments, such as the Minnesota Multiphasic Personality Inventory for Adolescents (MMPI-A) (Hathaway & McKinley, 1943), the Youth Self-Report (YSR) (Achenbach & Edelbrock, 1983), and the Children's Personality Questionnaire, Form A (CPQ) (Cattle & Klein, 1975), with good results, providing support for the construct validity of the SRP.
The current study used the Adolescent form of the BASC-SRP, which is applicable from ages 12 to 18. A Turkish version of the BASC was not available, therefore the investigator and another mental health expert whose native language is Turkish, translated the instrument into the Turkish language and used it in a couple of prior studies. Some items were found not to be applicable to the Turkish culture, so those items were modified to fit better in the cultural context. Several idiomatic, cultural and colloquial expressions were discussed with English and Turkish language experts, and necessary adjustments were made.
Children's Post-Traumatic Stress Disorder Reaction Index (CPTSD-RI). The CPTSD-RI is a 20-item, 4-point Likert-type self-report scale. It was designed to assess the post-traumatic stress reactions of children between the ages of 6 and 16 who have been exposed to different types of traumatic events (Frederick, 1986). CPTSD-RI is widely used in different parts of the world for measuring a broad range of traumatic experiences. The CPTSD-RI has good internal consistency, and it relates well to clinical diagnoses of PTSD (Yule & Udwin, 1991). Its composite score indicates the severity of PTSD symptoms. Scores are classified as "mild" (total scores of 12-24), "moderate" (25-39), "severe" (40-59), or as "very severe PTSD reaction" (above 60). Pynoos (1993) reported that the instrument's "severe" and "very severe" categories correctly identified 78% of the subjects who met the Diagnostic and Statistical Manual of Mental Disorder (DSM), Revised Tird Edition criteria for PTSD. The Cohen kappa inter-rater reliability was 0.87, which indicates high inter-item agreement. The CPTSD-RI was translated into the Turkish language and the statistical properties were established by Erden, Kiliç, Uslu and Kerimoglu (1999). The Turkish version also demonstrated significant correlations between the DSM-IV PTSD criteria and the CPTSD-RI scores. Test-retest reliability was found to be .86 and the Cronbach alpha internal consistency was .75. The scale was also able to capture 80% of the established DSM IV PTSD cases.
Results
Descriptive statistics (Table 1) show that for the whole group the mean of CPTSD-RI, at 43.57, was "severe" and well above the cut-of score of 40. For the BASC-SRP-A the subscales for somatization (61.40) and depression (60.24), indicated symptoms that were above the normal range, and represented a significant level of symptomatology and being "at risk", as suggested in the BASC manual (page 60). The Atypicality (59.24) and Clinical Maladjustment (58.34) subscales also approached the alarming level.
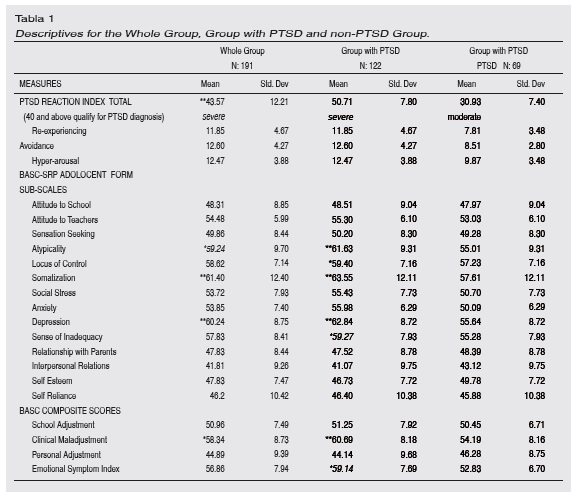
For the group diagnosed with PTSD, the CPTSD-RI mean of 50.71 was "severe". This was well above the clinical cut-of level, and qualified for PTSD diagnosis. For this group, somatization (63.55), depression (62.84), clinical maladjustment (60.69) and atypicality (61.63) all reached clinically significant levels. For this group, locus of control (59.40), sense of inadequacy (59.27), and emotional symptom index (59.14) all approached very close to the significance level.
The group regarded as non-PTSD, showed a CPTSD-RI mean of 30.93, regarded as "moderate". Although this group did not reach the clinical cut of level, some degree of PTSD reactions was evident at moderate levels. Even though none of the BASC-SRP-A subscales scores were high enough to be clinically significant, the somatization (57.61), locus of control (57.23) and atypicality (55.01) scores were quite high. At the same time, the non-PTSD group scored higher than the PTSD group in relations with parents, interpersonal relations, self esteem and personal adjustment subscales, all of which indicated better adjustment and functioning in daily life.
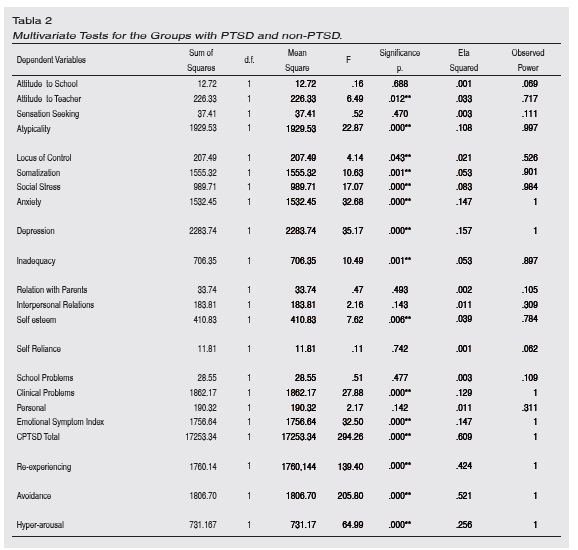
The with PTSD and non-PTSD groups were compared by using the Multivariate ANOVA on the dependent variables of the BASC SPR A subscales (Table 3). The results yielded some significant differences on the subscales for the variables of attitude to teacher, atypicality, locus of control, somatization, social stress, anxiety, depression, inadequacy, self-esteem and clinical problems. These two groups were also compared on the total trauma score and the trauma subscales. The groups differed on the CPTSD RI total scores and on the subscales for re-experiencing, avoidance and hyperarousal. As reported in the descriptive table, the PTSD group scored higher than the non-PTSD group in most of the variables, with the exception of relationships with the parents, interpersonal relations, self esteem and personal adjustment.
Adolescents were also compared for gender differences via the Multivariate ANOVA. The findings revealed that boys and girls differed significantly on the BASC subscales of attitude to school (43 vs. 50), sensation seeking (45 vs. 51) and school problems (47 vs. 52); in all of these three scales the males outscored the females. The depression subscale also approached significance level, but in this scale the females scored higher than the males (63 vs. 60). Gender differences were also observed on the CPTSI RI total scores (46 vs.43) and on the other three subscales, where the girls scored higher than the boys.
A set of Pearson correlations (Table 3) were computed between the CPTSD-RI total score, the re-experiencing, avoidance, and hyperarousal subscales, and the BASC-SRP-A subscales, in order to see the strength of the association and the predictive power of each disorder for PTSD. The correlations between CPTSD RI and depression (.47), anxiety (.46), clinical problems (.46), atypicality (.45), emotional symptom index (.45), social stress (.35), somatization (.34), attitude to teachers (.21), and locus of control (.20) were significantly positively correlated. However, self esteem (-.26) and interpersonal relations (-.17) were reversely associated.
The re-experiencing subscale and the BASC-SRP-A atypicality (.39), anxiety (.37), depression (.36), clinical problems (.36), emotional symptom index (.33), somatization (.24), social stress (.22), attitude to teachers (.18) were positively correlated, while self esteem (-.19) and interpersonal relations (-.15) were negatively correlated.
The avoidance subscale and BASC-SRP-A depression (.45), emotional symptom index (.44), atypicality (.42), clinical problems (.42), social stress (.38), anxiety (.37), inadequacy (.31), somatization (.29), and attitude to teachers (.21) were positively correlated, while self esteem (-.25) and interpersonal relations (-.17) were negatively correlated.
The hyperarousal subscale and BASC-SRP-A clinical problems (.36), anxiety (.34), somatization (.34), depression (.31), atypicality (.31), emotional symptom index (.32), social stress (.25), and locus of control (.19) were positively correlated, while self esteem (-.20) was negatively associated.
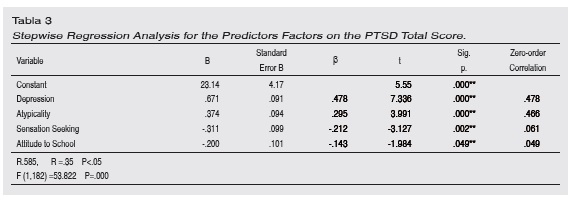
Multiple stepwise regression analyses were employed to determine the relative contribution of each of the BASC SRP A subscales, as independent variables, towards predicting the post traumatic stress disorder reactions. Table 4 shows the R, the change in R2, the standardized regression coeficients (beta), and zero-order correlations. At step 1 the strongest predictor of a PTSD reaction was depression, which accounted for 23% of the total variance. The next most significant contributing variable was atypicality, accounting for another 6%. This was followed, at step 3, by sensation-seeking, which added 4% of the variance. Finally, at step 4, attitude to school made a significant contribution of another 2% to the prediction of variances for PTSD severity. These four variables, together, explained 35% of the variance in CPTSD RI total score (r.585, r²=.35 p<.05) (Table 4).
Discussion
The CPTSD RI and subscale scores for the research population were significantly higher than normal, since all of the students were residents of the boarding school and they had all been exposed to the same harsh adversity. This is illustrated by the fact that 95% of students reported that they had lost at least one friend, 92% of them had experienced intense fear during the disaster, 92% had their homes damaged, 90% said their friends mentioned fear frequently, 90% had seen wounded people, 61% had seen dead bodies, 78% had seen damage to their homes, cars and property. Furthermore, they confiirmed that 80% watched TV news, 88% read newspapers and saw pictures in print media, and 59% listened to earthquake and disaster-related news on the radio. The group with PTSD scored higher than the non-PTSD group in all these areas. The same trend was also observed in the BASC subscales. It seemed that adolescents with PTSD demonstrated more mental health, social and personal adjustment problems. Among them, somatization, depression, atypicality and clinical maladjustment scores were serious enough to receive clinical attention (as being above 60). These 4 symptom groups were also significantly correlated with CPTSD RI total scores and with trauma subscales. Anxiety, depression, somatization and atypicality were also significantly correlated with each other. In regression analysis, depression and atypicality were significant predictors of PTSD scores. It appears that symptoms of depression are a significant construct in the PTSD symptom clusters, or in the accompanying comorbid disorders. Likewise, the depression scale was also significantly associated with the avoidance subscale of CPTSD RI. In support of this idea, Llabre and Hadi (1997) found .45 correlations between depression and PTSD scores in children who had experienced civil disturbance in Kuwait. Yule and Udwin (1991) reported similar results among British children after shipwreck accidents. They also mentioned an increase in depression rates in the chronic progression of PTSD. Goenjian et al. (2001) found .74 correlations between CPTSD RI and depressive symptoms in Nicaraguan adolescents after a hurricane. Furthermore, Shalev et al. (1998) believed that depression and PTSD are independent sequelae of trauma, showing similar progression, and working together to increase distress and dysfunction in survivors. There are also other studies reporting co-occurrences of these two constructs. Karakaya et al. (2004) found significant correlation between CPTSD RI and depression and anxiety symptoms in adolescent survivors in Turkey.
Even though, in this study, the anxiety subscale showed a good correlation (.46) with CPTSD RI, and with three other subscales, it did not have any predictive power in regression analysis. However, Lonigan et al, (1994) reported a high anxiety level to be the strongest risk factor for developing severe PTSD. La Greca et al. (1998) found children's predisaster level of anxiety to be a unique predictor of PTSD. In the same way, Evans and Oehler-Stinnett (2008) reported the BASC anxiety subscale as the strongest predictor of another trauma instrument in children exposed to tornados. Similar results were also reported with adult survivors (Green et al., 1994). In sum, it appears that anxiety is a strong correlate and predictor of PTSD and that the one shares common constructs with the other.
Atypicality demonstrated a strong correlation with CPTSD RI total scores (.45) as well as re-experiencing (.39), avoidance (.42), and hyperarousal (.31). This scale measures immature, bizarre and other odd behaviors, as are mostly associated with psychotic behaviors, for example visual or auditory behaviors (Reynolds & Kamphaus, 1992). As can be easily anticipated, atypical behaviors, as described here, fit well with re-experiencing phenomena. Trauma survivors may lose their sense of reality, and time space orientation, due to fashbacks. Similar psychotic-like, or dissociative features are commonly observed in combat veterans. This comparison is valid here since these children lost 83 of their friends and a teacher, and stayed under the rubble for days. Psychologists and school counselors should pay attention to bizarre behavior after significant traumatic events. These behaviors should not be interpreted as "psychotic" but as normal responses to abnormal events.
Sensation seeking was the 3rd strongest predictor, and explained 4% of the variance. Sensation seeking is defined as liking to take risks and seeking excitement. In prior research it was observed that delinquency, stealing, vandalism, looting, aggressive and anti-social behaviors, substance abuse, and early sexual experiences increase in adolescents during and after a disaster (Gramzey & Rutter, 1985; Pelcovitz et al., 1994). Sensation seeking and attempting new experiences can provide a unique future for an adolescent population.
Attitude to school was the weakest predictor, contributing 2% of the variance. This subscale measures alienation, hostility and dissatisfaction with the school atmosphere. Many studies indirectly touch on the issue of school and academic problems after a disastrous event. For instance, after a disaster adolescents demonstrate many functional and academic impairments (Giaconia Reinherz & Silverman, 1995), memory problems (DSM I V, 2000; Moradi, Doost, Taghavi, Yule & Dalgleish, 1999; Pynoos & Nader, 1989;), attention and concentration deficits (McFarlane, 1987; Tuicomepee & Romano, 2008), decreased school performance and achievement (Karabekiroğlu et. al., 2008; Milne, 1977; Shannon, Christopher, Lonigan, Finch, & Taylor, 1994;), academic difficulties (Dyson, 1990), poor attention and memory performance (Scrimin, Moscardino, Capello, & Axia, 2009). All of these are listed as secondary problems to PTSD, depression and anxiety. Since school achievement was not a part of our research interest, we did not collect any quantitative data relating to it.
Working among traumatized adolescents, McFarlane et al. (1987) reported common somatic reactions, while Dollinger (1986) and Llabre and Hadi (2009) reported somatic complaints and sleep disturbances. Likewise, Tuicomepee and Romano (2008) mentioned headaches and tiredness. Psycho-somatic symptoms eventually lead to school absenteeism and truancy (McFarlane et al., 1987). Norris et al. (2001) argued that somatic expressions of distress are common in developing countries. Furthermore, presenting symptoms, such as pain and weight loss, may also constitute somatic expressions of PTSD. According to Van der Kolk, Pelcovitz, Roth, Mandel and McFarlane (1996) somatization is represented, together with PTSD, by dissociation and failure to regulate affect, as part of the adaptation to trauma. It is very common in clinical literature to see that children with PTSD can also develop various forms of somatic symptom, as is seen with the Turkish adolescents in this current research.
In sum, PTSD can impair adolescents' daily functioning and worsen the psycho-social health of survivors. And the effect of traumatic events may last longer than it is expected (Bulut, 2010). Secondary stressors in the form of adverse living conditions may also aggravate the situation. As a result, children's social, cognitive and emotional development may be at risk (Delamater & Applegate, 2000). Multiple major disruptions can emerge as a result of PTSD, which can be expressed as academic and social impairment in functioning, increased aggression, sexually inappropriate behavior, learning difficulties, social withdrawal, losing a sense of reality, and severe family dysfunctions (Famularo et al., 1996).
Generally, people tend not to discuss their feelings, and there is a very little overt expression of any kind of emotional reaction in Turkish society (Bulut, 2003). Similar reactions are also reported among Chinese survivors (Wang et al., 2000). Feelings may occasionally be consciously experienced by people, but remain unexpressed. Those who do not fit these expectations may be seen as "different" or mentally challenged. Turkish people use different coping strategies to manage their conscious feelings and disappointments.
In Turkey, it is generally believed that the harmful aspects of negative emotional experiences are associated with weak psychological health. A common coping mechanism among Turks is to avoid potentially distressing situations, and to attempt to remain calm. If those situations are unavoidable, a conscious attempt is made to neither talk nor think about the potentially upsetting events. This was also confiirmed in a longitudinal study conducted with the same participants (Bulut, 2010). Therefore, we can therefore assume that internalizing problems is more common than any other form of psychological problem.
It is also commonly believed that excessive rumination, distress, and anxiety are the possible causes of mental and physical disorders. It is very normal for a Turk to talk and think about the absence or loss of loved ones, about financial difficulties, paying debts, affording education for the children, and to discuss the news about political and social issues. However, the death of a spouse, offspring, or sibling, is the most stressful and painful experience in someone's life due to the collective nature of the culture and the strong family ties among Turkish people. It seems that, even though an overwhelming majority of Turks live in urban areas and have a very modern life style, with highly individualistic and high mobility patterns, family ties remain strong, and this obviously protects individuals coping with stressful life events.
Norris et al. (2001) argued that somatic expressions of distress are widespread in developing countries. In previous research, psychiatric records indicated that Turkish people had complaints such as dizziness, headaches, disturbed sleep, loss of appetite, gastrointestinal problems and high blood pressure after a major earthquake (Bulut, 2003). This proves that the internalizing of problems, such as anxiety and depression or other somatic problems is more common than the externalizing of symptoms. Similar results were also reported by Braun-Lewensohn et al. (2008). In fact, as the BASC subscales of anxiety, depression and somatization show, these symptoms are easily recognizable, even in adolescents. Karancı and Rüstemli (1995) mentioned depression, anxiety and somatization among adult Turkish survivors. Similarly, Karakaya et al. (2004) also reported anxiety and depression as a comorbid disorder in Turkish earthquake survivors, after a different earthquake.
Unlike in some European and Oriental cultures, homicide or suicide, even in the form of an attempt, or the contemplation, is considered disgraceful both for the victim and family. It needs to be remembered that crime, homicide and suicide are exceptionally low in Turkey, and any news regarding incidents of this nature will traumatize the whole society. Homicides or suicides were not observed in the region after the disasters. In contrast, many citizens and civil and voluntary organizations rushed to help the students and the residence in any way they could. The school building was rebuilt and the students were moved to another city for a summer school, then, in the following September, they were able to return to their restored school. Donations to charities are seen as very common traditional and religious duties, and especially after such a huge disaster, people feel obligated to help the sufferers.
Recognized indicators of mental disorders include aggressiveness, quietness, talking or laughing to themselves, sexually inappropriate talk and gestures. Those are believed to be the result of extensive rumination and prolonged emotional stress. While some of these neurotic symptoms may be expressed by some Turkish individuals, psychosis is relatively infrequent in Turkey. In fact, the Turkish language does not even have the specific psychological terms that are needed to describe emotionally, or mentally disturbed psychotic mental states. This has also been reported by other western mental health experts (Jenkins & Baird, 2002).
There are many culturally constituted mechanisms for coping with distressful situations. For example, Hochschild (1979) coined the term "emotion work," as the purposeful and conscious act of trying to change, in degree or quality some emotion or feeling. It is a vigorous effort to evoke, shape, or suppress certain feelings. It is normal for Turkish people to be calm, and not very expressive, especially verbally. It seems that they do quite a lot of "emotion work" and manage their own emotional states and find ways to soothe others through the same approach. Another strategy is to intentionally suppress, or avoid troubling feelings and actions. A third strategy involves spirituality; they may be reminding themselves that God will restore peace and tranquility to their lives. Survivors seek refuge in fatalism when there is nothing else, and belief is a last resort. The city of Bingöl is situated in the eastern part of Turkey and has a traditional and rural character; it is therefore possible that people also sought and found comfort in spiritual and religious activities.
The fourth strategy is the conscious and deliberate avoidance of potentially upsetting situations. This was observed as both physical and emotional avoidance in previous studies conducted in Turkey (Bulut, 2003, 2010). Another aspect to consider is that, even though today Turkish lives and institutions are westernized, they have many traditional characteristics: For example, family and social structures are very hierarchical; therefore elderly and authority figures are highly respected. Similarly, confrontations with friends and colleagues, expressive language, showing of afection in public places, and assertive behavior are definitely discouraged at every level and in every kind of relationship. Accordingly, in a collectivist society individuals construct their own internal coping systems (Bulut, 2003).
References
Achenbach, T M., & Edelbrock, C. (1983). Manual for the Child Behavior Checklist and Revised Child Behavior Profile. Burlington: University of Vermont, Department of Psychiatry. [ Links ]
Braun-Lewensohn, O., Clestin-Westreich, S., Clestin, L. P., Verté, D., & Ponjaert-Kristofersen, I. (2009). [ Links ]
Adolescents' mental health outcomes according to different types of exposure to ongoing terror attacks. Journal of Youth and Adolescence, 38, 850-862. [ Links ]
Bulut, S. (2003). Underlying dimensions and prevalence of post traumatic stress disorder among 4th and 5th grade children who experienced the 1999 Turkish earthquakes. Doctoral Dissertation, Oklahoma State University, Stillwater, OK, USA. International Dissertation Abstracts. [ Links ]
Bulut. S. (2006) Comparing the earthquake exposed and non-exposed Turkish children's post traumatic stress reactions. Anales de Psicologia, 22(1), 29-36. [ Links ]
Bulut, S. (2009). Comparing children posttraumatic stress reactions in terms of gender and age after an earthquake. Turkish Journal of Counseling and Guidance, 4(31), 43-51. [ Links ]
Bulut, S. (2010). Children's posttraumatic stress reactions and sub-symptoms: Three years of longitudinal investigation study after a direct exposure to an earthquake and school's collapse. Turkish Journal of Psychology, 25(66), 87-100. [ Links ]
Bulut, S., Bulut, S., & Tayli, A. (2005). The dose of exposure and prevalence rates of post traumatic stress disorder in a sample of Turkish children eleven months after the 1999 Marmara earthquakes. School Psychology International, 26(1), 55-70. [ Links ]
Cattell, R. B. & Klein, T. W. (1975). A check on hypothetical personality structures and their theoretical interpretation at 14-16 years in T-data. British Journal of Psychology, 66, 131-151. [ Links ]
Cordova, M.J., Studts, J. L., Hann, D.M., Jacobsen, P.B., & Andrykowski, M.A. (2000). Symptom structure of PTSD following breast cancer. Journal of Traumatic Stress, 13, 301-319. [ Links ]
Delamater, A., & Applegate, B. (2000). Child development and posttraumatic stress disorder after hurricane exposure. Traumatology, 6. Retrieved October 14, 2000, from http://fsu.edu/~trauma/a3v5i3.htm. [ Links ]
DSM IV (1994). Diagnostic and Statistical Manual of Mental Disorders. 4th ed. DSM-IV. Washington, D.C.: American Psychiatric Association, 1994. [ Links ]
Dollinger, S. J. (1986).The measurement of children's sleep disturbances and somatic complaints following a disaster. Child Psychiatry and Human Development, 16, 149-153. [ Links ]
Dyson, J. L. (1990). The effect of family violence on children's academic performance and behavior. Journal of the National Medical Association, 82, 17-22. [ Links ]
Erden, G., Kiliç, E. Z., Uslu, R. I., & Kerimoglu, E. (1999). The validity and reliability study of the Turkish version of child posttraumatic stress reaction index. Çocuk ve Gençlik Ruh Sagligi Dergisi (Turkish Journal of Child and Adolescent Mental Health), 6, 143-9. [ Links ]
Evans, L., S. G. (2002). Theoretical constructs of posttraumatic stress disorder as assessed in children in a natural disaster involving in their communities. Unpublished doctoral dissertation, Oklahoma State University, Oklahoma. [ Links ]
Evans, G. L., & Oehler-Stinnett, L. (2008). Validity of the OSU posttraumatic stress disorder scale and the behavior assessment system for children self-report of personality with child tornado survivors. Psychology in the Schools, 45(2), 121-131. [ Links ]
Famularo, R., Fenton, T., Augustinian, M. & Zuckerman, B. (1996). Persistence of pediatric posttraumatic stress disorder after 2 years. Child Abuse and Neglect, 20, 1245-1248. [ Links ]
Flanagan, D. P. (1995). A review of the Behavior Assessment System for Children (BASC); Assessment consistent with the requirements of the Individuals with Disabilities Education Act (IDEA). Journal of School Psychology, 33, 177-186. [ Links ]
Flanagan, D. P., Alfonso, V. C., & Primavera, L. H. (1996). Convergent validity of the BASC and SSR: Implications for social skills assessment. Psychology in Schools, 33, 13-23. [ Links ]
Frederick, C. J. (1986). Children traumatized by catastrophic situations. In S. Eth, & R. Pynoss (Eds.), Posttraumatic stress disorder in children (17-44). Washington, DC: American Psychiatric Press. [ Links ]
Foa, B.E., Riggs, S.D., Gershuny, B.S. (1995). Arousal, numbing, and intrusion: Symptom structure of PTSD following assault. Journal of American Academy Psychiatry, 152, 116-120. [ Links ]
Giaconia, R. A., Reinherz, H. Z. & Silverman, A. B. (1995). Trauma and posttraumatic Stress disorder in a community population of older adolescents. Journal of American Academy of Child and Adolescent Psychiatry, 25(3), 384-392. [ Links ]
Goenjian, K. A., Molina, L., Steinberg, A. M., Fairbanks, L. A., & Alverez, M. L., et al. (2001). Posttraumatic stress and depressive reactions among Nicaraguan adolescents after Hurricane Mitch. American Journal of Psychiatry, 158, 778-794. [ Links ]
Gramzey, N. & Rutter, M. (1985). Acute Reactions to Stress. Child and Adolescent Psychiatry. Second Edition. Oxford: Blackwell. [ Links ]
Green, B. L., Grace, C. M., Vary, G. M., Kramer, T. L., Glesser, G. C., & Leonard, A. C. (1994). Children of disaster in the second decade: A 17-year follow-up of Bufalo Creek Survivors. Journal of American Academy of Child Psychiatry, 33, 71-79. [ Links ]
Hathaway, S. R, & McKinley, J. C. (1943). The Minnesota Multiphasic Personality Inventory. [ Links ]
Hochschild, A. (1979). Emotion work, feeling rules, and social structure. American Journal of Sociology, 85, 551-575. [ Links ]
Hubbard, J., Realmuto, G. M., Northwood, A. K., & Masten, A. S. (1995). Comorbidity of Psychiatric diagnosis with posttraumatic stress disorder in survivors of childhood trauma. Journal of American Academy of Child and Adolescent Psychiatry, 34(9), 1116-1173. [ Links ]
Kar, N. (2009). Psychological impact of disaster on children: Review of assessment and interventions. World Journal of Pediatrics, 5(1), 5-11. [ Links ]
Karancı, N. & Rüstemli, A. (1995). Psychological Consequences of the 1992 Erzincan (Turkey) Earthquake. Disasters, 19(1), 8-18. [ Links ]
Kar, N., J. & Murali, N. (2001). Post-traumatic stress disorder in children following disaster. Kerala Journal of Psychiatry, 16, 7-14. [ Links ]
Karabekiroğlu, K., Akbas, S., Taşdemir, G. N., & Karakurt, M. N. (2008). Post-traumatic stress symptoms in adolescents after two murders in a school: A controlled followed-up study. International Journal of Psychiatry Medicine, 38(4), 407-424. [ Links ]
Kim, B. N., Kim, J.W., Kim, H. W., Shin, M. S., Cho, N. H., & Ahn, H. et al. (2009). A 6- month follow-up study of posttraumatic stress and anxiety/depressive symptoms in Korean children after direct or indirect exposure to a single incident of trauma. Journal of Clinical Psychiatry, 70(80), 1148-1154. [ Links ]
Kun, P., Han, S., Chen, X., & Yao, L. (2009). Prevalence and risk factors for posttraumatic stress disorder: a cross-sectional study among survivors of the Wenchuan 2008 earthquake in China. Depression and Anxiety, Epub ahead of print. [ Links ]
La Greca, A. M., Silverman, & Wasserstein, S. B., (1998). Children's predisaster functions as a predictor of posttraumatic stress following Hurricane Andrew. Journal of Consulting and Clinical Psychology, 66, 883-892. [ Links ]
Lonigan, C. J., Shannon, M. P., Finch, A. J., Jr., Daugherty, T. K., & Taylor, C. M. (1991). Children's reactions to a natural disaster: Symptoms severity and degree of exposure. Advances in Behavior, Research and Therapy, 13, 135-154. [ Links ]
Llabre, M. M., & Hadi, F. (1997). Social support and psychological distress Kuwaiti boys and girls exposed to the gulf crisis. Child Abuse and Neglect, 26, 247-253. [ Links ]
Llabre, M. M. & Hadi, F. (2009). War-related exposure and psychological distress as predictors of health and sleep: a longitudinal study of Kuwaiti children. Psychosomatic Medicine, 71(7), 776-783. [ Links ]
Maida, C. A., Gordon, N. S., & Strauss, G. (1993). Child and parent reactions to the Los Angeles area Whittier Narrows Earthquake. Journal of Social Behavior and Personality, 8, 421-436. [ Links ]
McFarlane, A. C. (1987). Family functioning and overprotection following a natural disaster: The longitudinal effects of post-traumatic morbidity. Australian and New Zealand Journal of Psychiatry, 21, 210-218. [ Links ]
McFarlane, A. C., Policansky, S., & Irwin, C. (1987). A longitudinal study of the psychological morbidity in children due to a natural disaster. Psychological Medicine, 17, 727-738. [ Links ]
Merenda, P. F. (1996). BASC: Behavioral Assessment System for Children. Measurement and Evaluation in Counseling and Development, 28, 229-232. [ Links ]
Milne, G. (1977). Cyclone Tracy: I. Some consequences of the evacuation for adult victims. Australian Psychologist, 12, 39-55. [ Links ]
Moradi. A. R., Doost. H. T., Taghavi. M. R., Yule. W., & Dalgleish. T. (1999). Everyday memory deficits in children and adolescents with PTSD: performance on the Rivermead Behavioral Memory Test. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 40(3), 357-61. [ Links ]
Norris, H. F., Weisshaar, M., Conard, L., Diaz, E. M., Murphy, A. D., & Ibanez, G. E. (2001). A Qualitative analysis of posttraumatic stress among Mexican victims of disaster. Journal of Traumatic Stress, 14, 741-756. [ Links ]
Pelcovitz, D., Kapan, S., Goldenberg, G., Mandel, F., Lehane, J. & Guerrera, J. (1994). Posttraumatic stress disorder in physically abused adolescents. Journal of American Academy of Child and Adolescent Psychiatry, 33(3), 305-312. [ Links ]
Reynolds, C. R., & Kamphaus, R. W. (1992). Behavior Assessment System for Children: Manual. Circle Pines, MN: American Guidance Service, Inc. [ Links ]
Pynoos, R. S., & Nader, K. (1989). Case Study; Children's memory and proximity to violence. Journal of American Academy of Child and Adolescent Psychiatry, 28, 236-241. [ Links ]
Sabin, M., Lopes, C. B., Nackerud, L., Kaiser, R. & Varese, L. (2003). Factors associated with poor mental health among Guatemalan refugees living in Mexico 20 years after civil conflict. Journal of American Medical Association, 290(5), 635-642. [ Links ]
Sandoval, J., & Echandia, A. (1994). Behavior assessment system for children. Journal of School Psychology, 32, 419-425. [ Links ]
Shaw, A. J., Applegate, B., Tanner, S., Perez, D., Roth, E., Campo-Bowen, A., et al. (1995). Psychological effects of Hurricane Andrew on an elementary school population. Journal of American Child and Adolescent Psychiatry, 34, 1185-1192. [ Links ]
Shalev, A. Y., Freedman, S., Peri, T., Brandes, D., Sahar, T., Orr, S. et al. (1998). Prospective study of posttraumatic stress disorder and depression following trauma. American Journal of Psychiatry, 155, 630-637. [ Links ]
Shannon, M. P., Christopher, P. D., Lonigan, J., Finch, A. J. Jr., & Taylor, C. M. (1994). Children exposed to disaster: Epidemiology of post-traumatic symptoms and symptom profile. Journal of American Child and Adolescent Psychiatry, 33, 80-93. [ Links ]
Tol, W. W., Kohrt, B. A., Jordans, M. J., Tapa, S. B., Judith, P., Upadhaya, N. & et. al. (2009). Political violence and mental health: A multi-disciplinary review of literature on Nepal. Social Science Medicine, (Epub ahead of print). [ Links ]
Tuicomepee, A., & Romano, J. L. (2008). Thai adolescent survivors 1 year after the 2004 tsunami: A mixed methods study. Journal of Counseling Psychology, 55(3), 308-318. [ Links ]
van der Kolk, B. A., Pelcovitz, D., Roth, S., Mandel, F. S., & McFarlane, A. (1996). Dissociation, affect dysregulation and somatization: the complex nature of adaptation to trauma. Trauma Information Pages, Retrieved from http://www.trauma-pages.com/vander5.htm. [ Links ]
Wang, X., Gao, L., Shinfuktu, N., Zhang, H., Zhang, H., & Shen, Y. (2000). Longitudinal study of earthquake-related PTSD in randomly selected community sample in North China. American Journal of Psychiatry, 157, 1260-1266. [ Links ]
Yule, W., & Udwin, O. (1991). Screening child survivors of post-traumatic stress disorders: experience from the "Jupiter" sinking. British Journal of Clinical Psychology, 30, 131-138. [ Links ]
