











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkThe prevalence of eating disorders (ED) based on the DSM-V criteria (American Psychiatric Association, 2013) in adolescents (aged between 11 and 19 years old) is between 1.2% (male samples) and 5.7% (female samples) (Smink, van Hoeken, Oldehinkel, & Hoek, 2014), with increasing incidence over recent decades. In Spain, the prevalence is between 4.1% and 6.41% in female samples and between 0.27% and 0.90% in male samples between 12 to 21 years of age (Working Group of the Clinical Practice Guideline on Eating Disorders, 2009). In Peru, between 7.3% and 11.4% of teenagers have eating problems (Executive Directorate of Epidemiology, 2010) and the number of new cases registered between 1998 and 2008 has increased eight times, especially in adolescents (Peruvian news agency Andina, 2009). In the metropolitan area of the city of Lima, it was estimated that 16.4% of adolescents are at risk of developing an ED (Martínez, Zusman, Hartley, Morote, & Calderón, 2003). This epidemiological profile suggests an important public health problem (Swanson, Crow, Le Grange, Swendsen, & Merikangas, 2011), particularly considering the negative consequences of ED on physical and mental health (Campbell & Peebles, 2014).
Much research has been focused on the identification of the main risk factors for the onset and evolution of ED, such as perfectionism, internalization of the thinness ideal, dietary restriction, internalization of the beauty standard defined by the media, concern for one's weight and figure, negative affectivity or weight-related teasing (Culbert, Racine, & Klump, 2015; Stice, Ng, & Shaw, 2009). However, fewer studies have analyzed potential protective factors, such as positive body image, high self-esteem, positive self-assessment, rejection of the thinness ideal transmitted by the media and the ability to express opinions and feelings (Gustafsson, Edlund, Kjellin, & Norring, 2009).
A potential protective factor that is increasingly being considered is the frequency of family meals (FFM). On the whole, high FFM has been associated with multiple benefits for adolescents (Bisakha, 2010; Elgar, Craig, & Trites, 2013; Eisenberg, Neumark-Sztainer, Fulkerson, & Story, 2008; Fulkerson et al., 2006; Harrison et al., 2015; Loth, Wall, Choi et al., 2015; Neumark-Sztainer, Larson, Fulkerson, Eisenberg, & Story, 2010; Utter et al., 2013), including emotional well-being, better school achievement, satisfactory social relations, and the reduction of dieting and weight control behaviors. High FFM has also been linked with lower risk of excess weight and ED symptoms, as well as a decrease in the use and abuse of drugs (Berge et al., 2015; Neumark-Sztainer et al., 2004; Neumark-Sztainer et al., 2007). Regarding its implications for therapy program outcomes, increase in the FFM has been associated with greater efficiency in the treatment of ED (Cook-Darzens, 2016; Stice, Shaw, & Marti, 2007).
Regarding the underlying mechanisms facilitating the benefits of frequent family meals on ED, it has been argued that family meals could facilitate positive interactions and better communication between parents and children, and allow greater supervision of the children's eating behaviors; however, these pathways are still not entirely clear and require more research (Elgar et al., 2013; Elran-Barak, Sztainer, Goldschmidt, & Le Grange, 2014). Levin et al., 2012; Neumark-Sztainer et al., 2010; Offer, 2013). Differences in the sex of the adolescents have also been reported in the study of the mechanism underlying FFM, in the sense that boys tend to value the impact of family meals on mood more, while girls value their nutritional value most (Prior & Limbert, 2013).
FFM seems to be a protective factor for ED during adolescence, independent of whether meals are eaten with one or both parents, and it seems stable within the context of dysfunctional families, single-parent families or low socioeconomic levels (Levin, Kirby, & Currie, 2012; Neumark-Sztainer, Larson, Fulkerson, Eisenberg, & Story, 2010). The potential benefits of family dinners have been reported to be greater than family breakfasts and lunches (Burges-Champoux, Larson, Neumark-Sztainer, Hannan, & Story, 2009). Although, authors such as Pearson, Biddle and Gorely (2009) refer to the trend for adolescents to skip breakfast as their age increases, which would result in an increased risk of ED. Hallstrom et al. (2011) have also mentioned that boys reported having breakfast more regularly than girls, which may also influence their lower risk for ED.
The FFM has decreased significantly over recent years. Between 1999 and 2010, a third of adolescents reported having two or fewer family meals during the week, especially in families with low socio-economic levels (Neumark-Sztainer, Wall, Fulkerson, & Larson, 2013). According to the perception of adolescents, the main barriers to family meals are excessive working hours (of both parents and adolescents), a desire for autonomy, dissatisfaction with family relationships and the dislike of food prepared at home (Prior & Limbert, 2013; Neumark-Sztainer, Story, Ackard, Moe, & Perry, 2000).
Most research on the association of the FFM with ED has been conducted in Anglo-Saxon populations. A recent review conducted by Harrison et al. (2015) pointed out that factors such as geographical location and culture can make a great difference to the FFM profile: while 78% of young Spaniards reported high FFM, the prevalence decreased to 45% for young Americans and 32.9% for young Brits. Another study shows that, in North America, family dinners are more frequent in adolescent males than females, and this activity is more frequent in Hispanic adolescents, followed by Native Americans, Asian Americans and other ethnic minorities (Fulkerson et al., 2006). Finally, a study comparing the FFM between countries found that 36.5% of Latin-American and 18.9% of Spanish females did not eat breakfast, 7.1% of Latin-American and 2.1% of Spanish females did not eat lunch and 22.3% of Latin-American and 6.3% of Spanish females did not eat dinner (Cruz-Saez, Salaberria, Rodriguez, & Echeburua, 2013); this research also concluded that Latin-American adolescents ate less than three main meals during the day and were more afraid of gaining weight than Spanish teenage girls.
In summary, little research has explored the contribution of FFM as a protective factor of ED in different socio-cultural contexts. Particularly, Spain and Peru have differences in terms of food and meal habits, as well as meal schedules, that could contribute to differences in the association between FFM and risk for ED. As far as we know, there are no empirical studies for FFM in Peruvian populations. The present research aims to explore the different contribution of FFM on risk for ED-related variables in adolescents from Spain and Peru. As a secondary objective, we explore the potential moderating effect of the participants' sex and their origin on the contribution of FFM on the risk of ED. Due to the lack of cumulative empirical evidence on the variables of the study (particularly in Peruvian samples), no empirical hypotheses in the concrete sense of strengths for the potential associations have been formulated for the study. Based on the accumulated knowledge, we can only hypothesize that the FFM should influence ED risk measurements at adolescence, and that sex and country of origin could also moderate the potential associations.
Method
Participants
This study includes two samples of adolescents from Spain and Peru. The Spanish sample corresponds to the control group of the MABIC project, a longitudinal study carried out in Barcelona which sought to assess the effectiveness of a preventive program designed to reduce eating and weight-related disorders in adolescents in the general population (for a detailed description see Sánchez-Carracedo et al., 2016). This sample comprises n=703 adolescents recruited from 11 schools (10 public and 1 private) located in five municipalities of Barcelona (corresponding to the third assessment of the control group from the MABIC project in Spain, March 2013). These participants were in the third year of compulsory secondary education, 365 (51.9%) were boys and 338 girls (48.1%), the mean age was 14.9 (SD=0.51), and many individuals (73.2%) belonged to families within the range of mean to low socioeconomic status.
The Peruvian sample was made up of n=213 adolescents recruited in six schools, who were in their second or third year of secondary education (level of study equivalent to the Spanish sample). The number of boys was 51 (23.9%) and 162 were girls (76.1%), the mean age was 13.8 years (SD=0.59), and all the participants belonged to families with mean to low socioeconomic status. Data was collected during the months of April and May 2016.
Instruments
Risk for ED. Eating Disorders Inventory 3 (EDI-3; Garner, 2004). This self-report questionnaire assesses ED symptom levels and related behaviors through 91 items structured in 12 subscales. The present study uses the Spanish version of the scale (Elosua, Lopez-Jauregui, & Sanchez-Sanchez, 2010), which demonstrates adequate psychometrical indexes. We analyzed 3 ED subscale scores (drive for thinness -DT-, body dissatisfaction -BD- and bulimia -B-), as well as the global Eating Disorder Risk Composite (EDRC) score. Internal consistency in our sample was between adequate (Cronbach's a=.72 for B scale) to excellent (a=.88 for DT). It should be pointed out that there are no empirical studies for the validation of the Peruvian EDI-3, only those for the EDI-2 are available (Guerrero-Canale, 2000). The EDI-3 was used in this study because the Spanish data had previously been collected by the MABIC project using the EDI-3, and it was necessary to have the same measurements in Spain and Peru to allow for statistical comparison.
Family meal patterns. FFM was assessed with the question "During a normal week (7 days), how many times did all, or most of your family living in your house eat a meal together?" (raw scores were from 0 to 7) (these values correspond to those used in the study of Burges-Champoux et al., 2009). Three measures were considered for the analyses (the participants answered three direct questions): the frequency of breakfasts, lunches and dinners eaten with the family group. The frequency for each family meal was also treated as a categorical variable for descriptive purposes (scores were grouped into three levels: 0-1, 2-4 and 5-7 times) (Eisenberg et al., 2008; Fulkerson et al., 2006). The internal consistency of the raw scores for the three questions was adequate in the study's sample (a=.78).
Other demographic and clinical variables related to risk for ED. The social status of the family was estimated with the Hollingshead Two-Factor Index of Socioeconomic Status (SES) (Hollingshead, 1975), based on combining the parents' educational level and occupational prestige. The adolescents' body mass index was computed as the ratio between weight (kg) and height (m).
Procedure
This study was carried out in accordance with the latest version of the Declaration of Helsinki. The Ethics Review Committee of Clinical Research at the authors' institution approved the study.
After obtaining the written consent to participate in the study from the adolescents and their parents, the adolescents answered the questionnaires in their usual classrooms. The mean time taken to answer the questionnaires was about 60 minutes. In the Spanish sample, weight and height were then registered by trained post-graduate personnel in a private room next door, according to a standardized procedure. In the Peruvian sample, since it was not possible to obtain these measurements on-site at the schools, the adolescents reported these values to the study directly on the day following the assessments.
Statistical analysis
The statistical analysis was carried out with SPSS22 for Windows. Multiple linear regressions measured the contribution of FFM (independent variables) on the risk for ED (criteria). Regressions were adjusted in three blocks/steps: (a) the first block fixed the covariates age, socioeconomic level and BMI, as well as the participants' sex and country of origin (i.e., the origin of the sample); (b) the second block added the independent variables number of family breakfasts, lunches and dinners; and (c) the third block entered and tested the relevance of the interactions family meals-by-sex and family meals-by-country. For relevant interactions, these parameters were retained in the final model and single effects for sex and country were estimated/interpreted. For non-relevant interactions, these parameters were excluded and main effects were estimated. Since the objective of this study is to screen for any possible interaction terms, rather than testing for a hypothesized specific interaction, the p-value to consider relevant interaction terms was fixed at p<0.10 to avoid low statistical power and sensitivity (Kleinbaum, Küpper, Muller, & Nizam, 2013)
Effect size in this study was estimated through Cohens' d coefficient for categorical and mean comparison (small low effect size was considered for |d|>0.20, moderate for |d|>0.50 and high for |d|>0.80), and through the 95% confidence interval (95%CI) for the regression models
Results
The first part of Table 1 includes sociodemographic descriptions for the sample, showing differences between countries for sex, SES and chronological age (the Peruvian group registered a higher proportion of women, lower SES levels and lower mean age). Differences between countries also emerged for the three FFM measures (second part of Table 1), but effect size was only in the moderate to high range for breakfasts (Peruvian participants registered a higher mean than the Spanish; 3.9 versus 1.9) and dinners (the Spanish sample achieved a higher mean than the Peruvian; 5.7 versus 4.3). The comparison for the EDI-3 subscales (third part of Table 1; results obtained through ANOVA adjusted by the participants' sex, age and BMI) also achieved significant differences between countries for body dissatisfaction, bulimia and EDRC index (for these three subscales, mean scores were higher for the Peruvian group, but effect size was in the poor range for the body dissatisfaction score).
Table 1 Descriptions for the sample: sociodemographics, FFM and EDI-3 scores in Spain and Peru
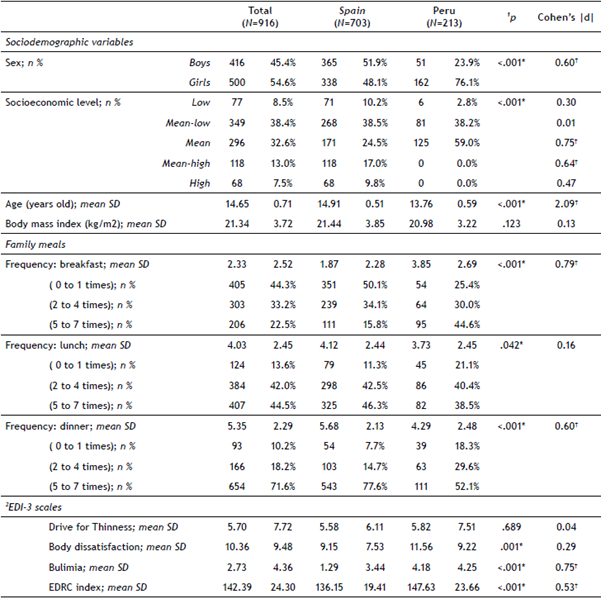
Note. SD: standard deviation. ED: eating disorder. EDI-3: Eating Disorder Inventory. EDRC: eating disorder risk composite.
1Chi-square for categorical variables and t-test for quantitative variables.
2Results adjusted by the participants' sex, age and body mass index.
*Significant difference (.05 level). †Effect size into the moderate (|d|>0.50) to high range (|d|>0.80)
Contribution of family meals in EDI-3 scores:Table 2 includes the results of the multiple regressions that value the contribution of the family meals on the scores of the EDI subscales (Table S1 in the annexed materials includes the complete parameters for the regressions). The model resulting from the criterion EDI-3 DT retained three relevant interaction parameters (breakfasts-by-country, breakfasts-by-sex and dinners-by-sex), supporting the moderator effect of the country and the adolescents' sex. Results for this final regression indicate that high scores in the drive for thinness subscale were explained by low frequency of family breakfasts for Spanish girls, high frequency of family breakfasts for Peruvian boys and low frequency of family dinners for girls only.
Table S1 Associations between frequency of family meals and scores of the EDI subscales: multiple regression
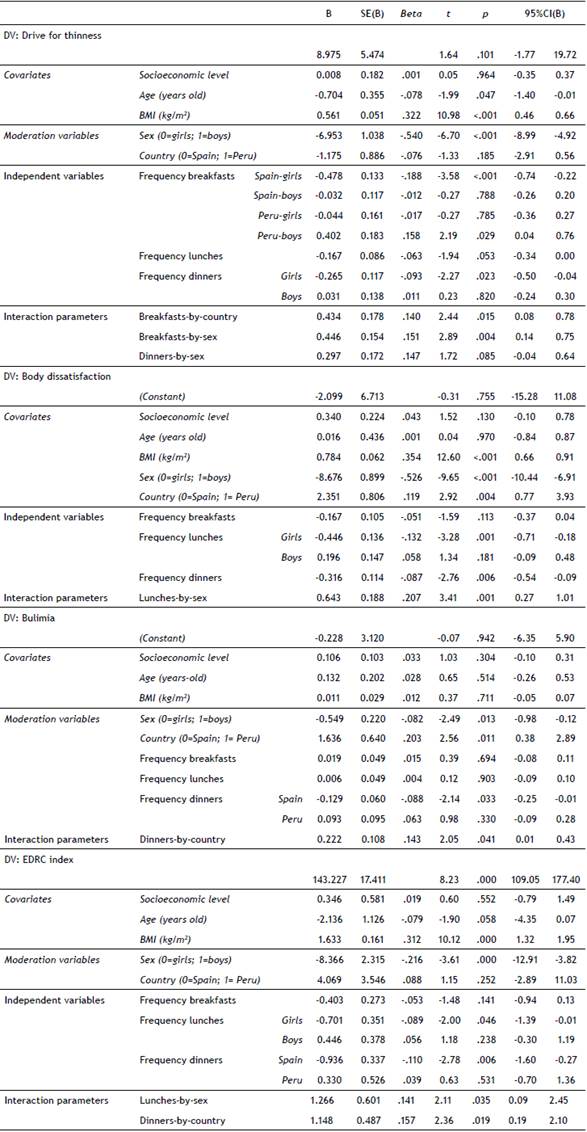
Note. DV: dependent variable (criterion). B: non-standardized regression coefficient. SE: standard error. b: beta coefficient. 95%CI: 95% confidence interval. EDRC: eating disorder risk composite. *Significant parameter (.05 level).
Table 2 Associations between the FFM and the EDI raw scores: multiple regressions
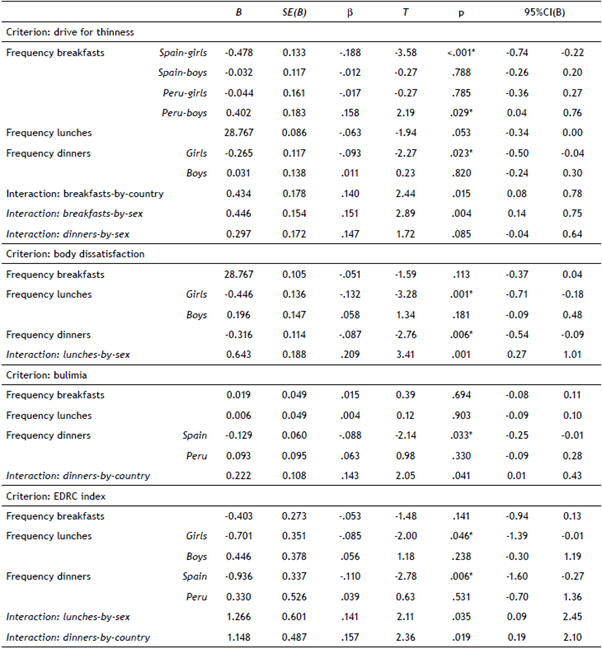
Note. B: non-standardized regression coefficient. SE: standard error. β: beta coefficient. 95%CI: 95% confidence interval. EDRC: eating disorder risk composite. *Significant parameter (.05 level).
One relevant interaction parameter was retained in the model resulting from the criterion EDI-3 BD (lunches-by-sex). The resulting regression indicates that high scores in the body dissatisfaction score were registered for patients with low frequency of family lunches (for girls only) and low frequency of dinners.
For the EDI-3 B score, one interaction parameter was retained in the final multiple regression (dinners-by-country), and results indicate that the highest scores in the bulimia score were related to the lowest frequencies of dinners (for Spanish participants only).
Finally, the model registered for the EDI-3 EDRD composite score showed that higher risk indexes were registered for girls who reported lower frequencies of family lunches and Spanish participants who reported lower frequencies of family dinners.
Discussion
This research sought to explore the FFM with adolescents recruited in Spain and Peru and the contribution of this measure to the risk of ED-related variables. Firstly, our results are consistent with data showing that the family dinners are more frequent than other family meals during adolescence (Burges-Champoux et al., 2009), with family breakfasts being the least frequent meal (Lazzeri et al., 2016). Secondly, this study provides evidence on the specific role of the adolescent's country of origin and their sex on the specific associations between the FFM and the eating measurements.
Regarding the origin of the sample, Spanish adolescents reported higher frequencies of family dinners: more than 75% of the participants in this group eat dinner with their family between 5 and 7 times a week, compared to just over half of Peruvian adolescents. With regard to breakfast, more than 50% of Spanish adolescents eat with their family at least once a week, compared to 25% of Peruvian adolescents. These differences could be due to the food and meal habits of each country. In Spain, dinners are perceived as the main family meal (MERCASA, 2008), and usually occur between 08:30 pm and 11:00 pm (Moreno, 2010; Díaz-Méndez & Callejo, 2014), while in Peru breakfast is of great importance (RPP News, 2013) and dinners are perceived as less relevant than other meals (occuring between 7:00 pm and 9:00 pm) (The Trade, 2011). Regarding dinners, Peruvian adolescents have more time after this meal before going to sleep, which would increase the likelihood of dining out or having dinner alone. This is in agreement with data from the National Statistics Institute of Peru, which shows that eating outside the home has become an everyday occurrence among Peruvians, especially among males (Peru 21, 2015), and that around 40% of Peruvians tend to eat in the street several times a week (RPP News, 2012). However, more research is needed to clarify this issue.
Considering the EDI-3 scores, Peruvian adolescents reported higher means in BD, B and in the overall EDRC index. These results agree with the prevalence reported in the literature for a higher occurrence of eating-related problems in Peruvian adolescents (Cruz-Saez et al., 2013; Dirección Ejecutiva de Epidemiología, 2010). The reason for these differences could be the greater levels of body dissatisfaction and fears of gaining weight in Latin-American female samples, who tend to be shorter and usually achieve a higher concentration of muscle, fat and weight, even at young ages (Cruz-Saez et al., 2013).
On the whole, we found that higher FFM is associated with a decreased risk of ED, especially in the female sub-sample and in Spanish adolescents (for many of the variables of the study). As already mentioned, Spanish adolescents eat more frequently with their family than Peruvians, probably for reasons related to the countries' different schedules. This higher frequency of family dinners in Spanish adolescents could contribute to the adolescents staying at home after dinner, which could in turn favor greater interaction and communication between the members of Spanish families (this factor seems to be a key component for the protective effect of FFM) (Offer, 2013). On the other hand, since Peruvian teenagers dine earlier, they have more time to perform other activities after dinner, which would result in less time for interaction with the family. In addition, it has been observed that the distribution of the adolescents' time is influenced by the socioeconomic level of the family: the higher the educational and economic level, the greater the connection between parents and children and the better organization of the adolescents' time, even for meal times, facilitating family meals (Wight, Price, Bianchi, & Hunt, 2009). In the present study, there is no presence of high socioeconomic levels in the Peruvian sample, while 28% of the Spanish sample belong to high or medium-high levels. This data could explain the moderating effect of the country on the relationship between FFM and the ED risk.
Our data also shows that the association of higher FFM with lower scores in the different ED risk variables is relevant only in the female population (concretely, the frequency of family breakfasts and DT, the frequency of family dinners and DT, the FFM and BD, and the frequency of family lunches and EDRC). These results could suggest that the potential protective effect of FFM associated with communication among family members affects the female population especially, who may perceive family meals as an opportunity to share their problems and discuss nutritional topics (Prior & Limbert, 2013). Studies such as Harrison et al. (2015) agree that the effects of frequent family meals benefit females more than males, while other research, such as Eto, Koch, Contento and Adachi (2011), agrees that females have better motivations and a more positive attitude with respect to family meals compared to males.
Limitations and strengths
This study has several limitations. The data analyzed has a cross-sectional design, which makes causal interpretations difficult. Regarding the measurement tools, weight and height was self-reported for Peruvian participants, which compromises its reliability. We could not use the EDI-3 version in the Peruvian population due the lack of empirical evidence for this adaptation (only data referring to the EDI-2 version is available). Spanish and Peruvian samples present some differences in sociodemographic variables that could affect the interpretation of the results. However, in order to control this possible bias, in the analysis, these variables were introduced as covariates. Finally, it should also be mentioned that although the size of the samples is different according to country of origin (Spain or Peru), this aspect should not be considered as a limitation since the sizes of the groups are large enough to guarantee statistical power. In fact, we considered it to be preferable to use the maximum number of subjects from each country to contribute to the improvement of the external validity of the research (selecting subjects in order to have equivalent sample size could introduce an unnecessary selection bias to the research) (Hocking, 2013; Maas & Hox, 2005).
The main strength of this study is that the FFM has been studied for the first time in a large sample of adolescents recruited in two different countries. Therefore, the empirical evidence of the research can be considered to be a starting point for future research about the protective factors for the onset and evolution of ED, particularly the effects of the FFM on the health of children and adolescents. Promising results have been reported in pioneer studies (DeBar et al., 2012; Dwyer, Oh, Patrick, & Hennessy, 2015; Rosenkranz & Dzewaltowski, 2009; Sánchez-Carracedo, Carretero, & Conesa, 2016. Future research should include other relevant information such as the quality of the interactions during the family meals. On the other hand, since during the school period some children and adolescents are at school for lunch, it would also be interesting for future research to obtain empirical evidence on the risk/protective factor of eating at school on eating disorders.
Implications
The results obtained in this study reinforce the relevance of including family meals in preventive and therapeutic programs in the area of eating problems and eating disorders. A recent public policy initiative implemented in Spain has focused on the promotion of family meals as a key message for the prevention of ED (Sánchez-Carracedo et al., 2017). Family meals should be valued for more than their function to satisfy hunger. They are also an excellent opportunity to promote family interactions, solve problems, learn good eating habits and contribute to physical and psychological health.

