











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkAttention deficit hyperactivity disorder (ADHD) is one of the most common childhood neuropsychological disorders and adolescence (APA, 2013; DuPaul, Weyandt, O'Dell & Varejao, 2009; Wolf, Simkowitz, & Carlson, 2009). The prevalence rate, estimated at 5.3%, is similar across european countries and throughout the world (Polanczyk, de Lima, Horta, Biederman, & Rohde, 2007). ADHD is a neurodevelopmental disorder, which is chronic and persistent, and it affects the basic psychological processes involved in learning, social adaptation, and affective adaptation (Lavigne & Romero, 2010a). Based on its manifestations, there are three diagnostic criteria: (1) ADHD, predominantly hyperactive-impulsive presentation (10%); (2) ADHD, predominantly inattentive presentation (30%); and (3) ADHD, combined presentation (i.e. when ADHD meets the criteria for types 1 and 2) (60%). The two latter types are mainly observed the most significant characteristics of ADHD are inattention, excessive activity, and lack of inhibitory control (Rubia, 2011). A child is considered to be diagnosed with ADHD when the aforementioned behaviors stand out, with respect to their frequency and intensity, compared to what is common for the subject's age and development. The result is that the child suffers from maladaptive behaviours (Alda, 2009). There is a generalized tendency to consider ADHD to be a disorder with a neurobiological basis that is characterized by the presence of a deficient development of the regulatory mechanisms of attention, reflexivity, and activity (Mas, 2009). However, we consider that a marked difficulty in psychological processes involved in executive functioning should be added to the aforementioned characteristics (Miranda & Soriano, 2010; Rubia, Smith, Brammer, & Taylor, 2007; Servera, 2005). Traditionally, executive functions have been considered an umbrella term that encompass a series of higher order processes governing action towards an objective, which allows for adaptive responses to novel or complex situations. Barkley (1998) defined them as self-directed actions that the individual uses to promote self-regulation. Executive functions (EF) constitute a set of cognitive skills that are included in a complex multimodal system formed by different elements that interact to achieve problem solving and goal-directed behaviour. In this way, EF receive input from different components, including anticipation and development of attention, impulse control and self-regulation, mental flexibility and use of feedback, planning and organization, and the effective selection of problem solving strategies and monitoring (Anderson, 2008; Bauermeister et al., 2005; Portellano, 2014).
Several models have been proposed to explain executive functions (Tirapu, García, Ríos, & Ardila, 2011) although none have been universally adopted. We briefly summarize these models by pointing out that the first ones tended to conceptualize executive functions from a "unitary" perspective such as the "central executive" model suggested by Baddeley (1986) or the "supervisory attentional system" model proposed by Normal and Shallice (1986). However, this option seems too simple for a construct that is composed of different and inter-related components or dimensions. Furthermore, the model proposed by Miyake et al. (2000), which considers three independent nuclear factors: inhibition, working memory, and flexibility, has been very influential over the last decade. Miyake et al. (2000) examined how independent these three executive functions components were by using conirmatory factor analysis. According to the authors, they focused on these three factors that are easily operationalized and can be studied through common tasks, which avoids "impure measures". They are, however, still involved in performing complex tasks such as the Wisconsin Test or the Tower of London. Similar results were obtained by Lehto, Juujärvi, Kooistra, and Pulkkinen (2003) in a sample of children aged between 8 and 13 and by Manly et al. (2001) with children between 6 and 16.
As shown in the specialized, literature there have been many research efforts aimed at operationalizing and measuring the processes and functions of the executive functioning system involved in ADHD. However, controversies still remain regarding what these neuropsychological variables are and which tools are the most suitable for evaluating them (Félix, 2005, 2006; Miranda, Félix, & Ávila, 2005).
Lately, there has been an increased rate in the diagnosis of ADHD. In Spain, this rate has reached over 9% of the school population between the ages of 5 and 15 (Lavigne & Romero, 2010b). Faraone, Sergeant, Gillberg, and Biederman (2003) note that the diagnostic rate is between 2.4 and 19.8%. In the United States, the number of cases of ADHD has increased by 22%, which means there is a 10% prevalence (García-Peñas, & Domínguez-Carral, 2012). Therefore, the United Nations (UN), through the United Nations International Children's Emergency Fund (UNICEF) and the World Health Organization (WHO), have detected and drawn attention to this increase in the diagnosis rate of ADHD. In addition, ADHD is a disorder that has a high comorbidity (Jensen et al., 2001), and studies such as the one undertaken by Hodgkins et al. (2013) show that more than half of the individuals diagnosed with ADHD manifest three or more comorbidities. Hence, there is a need to know not only the inclusion criteria, but also the exclusion criteria in order to avoid false positives or false negatives in any diagnosis. As a consequence, there are difficulties with regards to finding a consensus on the criteria for elaborating a diagnosis of ADHD as well as with establishing the appropriate evaluation instruments. While it is true that there are tools that help the evaluation of the disorder, few actual facts are known on the usefulness and diagnostic validity of these tools (Clinical Practice Guide, 2010).
Great advances have been made with respect to the analysis of EF. There are tests that evaluate each of the basic components, such as the Trail Making Test (TMT) (Reitan, 1992) or the Tower of Hanoi (TOH) (Simon, 1975) to evaluate planning; the Boston Naming Test (BNT) (Kaplan, Goodglass, & Weintraub, 1983) to evaluate word-finding abilities; the Wisconsin Card Sorting Test (WCST) (Heaton, Chelune, Talley, Kay, & Curtiss, 2001) to measure flexibility; the Token Test (De Renzi & Vignolo, 1962) to evaluate working memory; the Stroop Test (Stroop, 1935; Golden, 2006), the Five Digits Test (FDT) (Sedó, 2007) and the Go/No-Go task (Donders, 1969) to assess inhibition; and the Iowa Gambling Test (IGT) (Bechara, 2007) to assess decision-making ability. The following are examples of neuropsychological batteries that include different aspects: the Behaviour Rating Inventory of Executive Function (BRIEF) (Gioia, Isquith, Guy, & Kenworthy, 2000); the Luria-Nebraska Neuropsychological Battery (LNNB) (Manga & Ramos, 2006); and the Developmental Neuropsychological Assessment (NEPSY-II) (Korkman, Kirk, & Kemp, 2014). Taking into account the state of the literature presented and the relevance of the evaluation of ADHD to diagnose ADHD (Barkley, 1998), in the present study, we chose the Neuropsychological Assessment of Executive Functions in Children battery (Portellano, Martínez-Arias, & Zumárraga, 2009) to evaluate the sample. We chose this because we believe that the set of exercises that make up the battery, and taking into account the model described by Miyake (2000), measure the three components of executive functions (inhibition, working memory, and flexibility) using different exercises.
For the reasons that have been stated thus far, we determined that the ultimate aim of the present research was to assess the usefulness and diagnostic validity-both globally and also separately based on the scales-to support the diagnosis of ADHD in relation to detecting a specific pattern in executive functions that are measured using the ENFEN Battery
Method
Participants
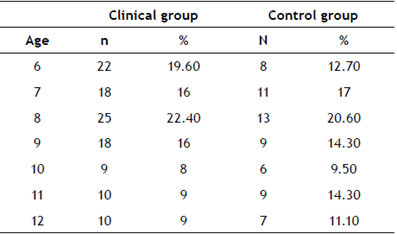
The sample consisted of a total of 175 participants of which 112 belonged to the clinical group and 63 belonged to the control group.
The subjects were aged between 6 and 12 (clinical M=8.39, SD=1.87, and control M=8.78, SD=1.91) (Table 1).
The clinical group comprised 79.50% males and 20.50% females, and the control group comprised 58.70% males and 41.30% females. The ethnicity of the children was 81% Caucasian, 15% sub-Saharan, 7% Romani, and 7% other ethnic groups. All participants were enrolled in various stages of primary education.
Regarding the sociodemographic data that was used in this study, in terms of types of families, 69.3% were nuclear families, 21% were single-parent families, 2.7% were LGBTI families, and 7% were reconstituted families. In terms of members of the families' sex, 45.94% were men and 54.06% were women. The average age of the parents was 43.67 years (dt±8.717); there was a minimum age of 29 and a maximum of 64. The women were aged between 31 and 61, with a mean of 41.61 (dt±7,860). In addition, 74.7% of families lived in urban areas, compared to the 25.3% of families in rural areas.
Fifty-six percent of the families had only one child, compared to 40% that had between two and three children and 12% that had between three and four children.
In terms of family support networks, 41.3% of the families indicated that they had a combination of support networks (parents, siblings, friends, and professional care-givers) compared to 43.3% that only have parents, siblings, or friends as support networks, and 14.7% that indicated having other types of support.
Regarding education and employment, the following variables were analyzed: educational level, employment situation, and families' monthly income. For educational level, in foster care it can be seen that 82.4% of male carers undertook higher education (professional and university training), compared to 83.9% for female carers. In addition, 68.4% of male carers and 54.1% of female carers had indefinite or open-ended contracts. More than half of the foster care families (50.7%) had incomes ranging between € 2,000 and € 3,000 per month.
Evaluation instruments
The following tools were used in this study:
The Neuropsychological Assessment of Executive Functions in children battery (Portellano et al., 2009). ENFEN is a battery of individual applications that allows executive functions to be globally evaluated by using a variety of elements in children between the 6 and 12. The duration of the ENFEN battery is approximately 20 minutes, and it consists of 4 tests divided into 6 scales: Phonological Fluency (PF) and Semantic Fluency (SF), which evaluate phonological and semantic access, respectively as well as vocabulary amplitude, verbal, and explicit memory; Construction of the Grey Path (GP) and Colour Naming Path (CNP), which evaluate perceptive speed, sustained and selective attention, cognitive flexibility, graphomotor (handwriting) and visual-motor coordination, working memory, and spatial perception; Rings (R), which evaluates planning and sequencing capacity, working memory, and fundamental abstraction capacity; and Interference (I), which evaluates selective and sustained attention, inhibition capacity, and resistance to interference in an essential way. Decatypes includes a profile of these six indices and shows the strengths and weaknesses of what was evaluated. It is noteworthy that the Rings (R) scale was not included due to a technical decision including the reasons explained below. Although the ENFEN manual does not provide data on the reliability and validity of the scales that make up the battery, it does provide the average differences found in the sample scaling with respect to age and sex. The factorial analysis carried out by the authors of the ENFEN manual concluded with a single factor. This was because, due to the characteristics of the prefrontal executive system, it behaves as a unitary system. Furthermore, the factorial analysis using the data in the present study obtained similar results; thus, both studies found it to be a similar unifactorial solution.
ADHD Rating Scale (ADHD-RS) DSM-IV (DuPaul, Power, Anastopoulos, & Reid, 1998) consists of a scale of 18 Likert-type items that includes 4 points (0 = never or rarely, 1 = sometimes, 2 = often, 3 = very often) the basis of which is the DSM-IV diagnostic criteria. The scale measures the dimensions of inattention and impulsivity/hyperactivity in both the family and the school environments through the frequency of how often the nine symptoms appear. The Spanish version of this scale is used (Servera & Cardó, 2007) in the present study, which rates a score of ≥P90 in each dimension to be clinically significant. In the inattention and hyperactivity/impulsivity dimensions, the Cronbach's alpha values (or coefficient alpha) for family members were .85 and .90, respectively; and for teachers, they were .91 and .93, respectively.
WISC-IV Wechsler Intelligence Scale for Children-Fourth Edition (Wechsler, 2003): scale composed of 15 tests. The result from each of the tests relates to the level of cognitive abilities relating to a series of intellectual competences. Five primary index scales are obtained: Verbal Comprehension (VC), Perceptual Reasoning (PR), Working Memory (WM), Processing Speed (PS), and Full Scale IQ (FSIQ).
Procedure
This research was conducted in accordance with the ethical principles that have their origin in the current Declaration of Helsinki. A positive vote of approval regarding the study and its methodology was granted by the institutional review board: the Ethics Committee of the University of Alicante (assigned file number: UA-2018-03-08).
A non-experimental research design was followed for this comparative descriptive study. The subjects who comprised the sample were recruited after being referred by Child and Adolescent Mental Health Units in the provinces of Alicante and Malaga, Spain. The evaluators, four psychologists with extensive experience in the field of evaluation and intervention in learning difficulties, have rigorously implemented the same evaluation procedure and data collection.
The following inclusion criteria were applied:
Present an ADHD diagnosis. To this end, the aforementioned ADHD Rating Scale (ADHD-RS) DSM-IV was given to school caregivers and tutors and based on the DSM-IV diagnostic manual criteria. The subjects with a ≥6 score were selected as is indicated in the test manual. This scoring had to occur in both contexts (family and school), following the diagnostic criteria of the DSM-IV (APA, 2013).
Present a General Capacity Index (GCI) higher than >80 because, if it were lower, the results would be affected not only by the executive deficit but also by the cognitive capacity of the subject. The GCI is obtained using the WISC-IV psychometric test (Wechsler, 2003), which has a proved robustness. The GCI is used rather than the intelligence quotient (IQ) because there is evidence that the latter is more affected by the executive dysfunction associated with ADHD (Fenollar, Navarro, González, & García, 2015; Navarro, Fenollar, Lavigne, & Juarez, 2017; Navarro, Fenollar, Carbonell, & Real, 2019).
The control sample was obtained using simple random sampling, carried out in 6 public schools (4 in Alicante and 2 in Malaga) and 2 concerted schools (Malaga). The inclusion criteria consisted of a negative score on the ADHD Rating Scale (ADHD-RS) DSM-IV, and obtained a balanced cognitive pattern using a GCI higher than 80 that was measured using WISC-IV.
Statistical analysis
In order to determine whether or not the sociodemographic variables (sex and age) of the two experimental conditions were homogeneously distributed, contingency tables and the Χ2 test were calculated. Furthermore, an exploratory factor analysis was also calculated to confirm the unidimensionality of the ENFEN battery. Subsequently, the Student's t-test was applied in order to establish the differences between the population means obtained by the clinical group and the control group for the different ENFEN tests. The d (typified mean difference) proposed by Cohen (1988) was included, which permitted the magnitude of the effect of the differences found between groups to be evaluated. The criteria established to assess the d are the following: .20≤d≤.49-this range indicates a low magnitude of differences; .50≤d≤.79-this range points out a clinically significant difference, and; d> .80-this range indicates clinically relevant differences. Finally, a binary logistic regression analysis (BLRA) was undertaken in order to examine (1) which scores on the ENFEN scales were associated with the diagnosis of ADHD and (2) the areas under the curve (AUC) of the Receiver Operating Characteristic (ROC) curves in order to estimate the diagnostic capacity of ENFEN to determine an ADHD diagnosis.
Results
Firstly, we made the contrast that both samples were homogeneously distributed according to age (Χ2 (6) = 2.68, p = .85, Pearson correlation coefficient = .12). However, in terms of sex, we found that the proportion of males and females in the control group and in the clinical group was not homogenously distributed; there was a higher percentage of males in the clinical group (Χ2 (1) = 7.60, p = .01). It is noteworthy that Cramer's V was .22, which indicates low sample effect sizes or low ratios (i.e. low odds ratio, OR). This coincides with the clinical reality since ADHD is more frequent in males than in females (APA, 2013).
Firstly, a factorial analysis was carried out, which proved that all the dimensions could be reduced to a factor. The Kaiser-Meyer-Olkin (KMO, a measure of sampling adequacy) index obtained a value of .78, showing that the matrix was adequate to undertake a factorial analysis. The Bartlett test for sphericity reached a statistically significant value (p<.001). Taking into account the Kaiser Eigenvalue >1 criterion, a unique factor was extracted (accounting for 52.76% of the total variance), which demonstrates the one-dimensional structure of the test.
Secondly, Table 2 shows the results of the differences between the male subjects in the clinical group and in the control group in terms of the five scales of the ENFEN battery's mean scores. As can be seen, the clinical group scored significantly lower than the control group in all of the scales, except for Semantic Fluency (SF), for which the differences did not reach statistical significance. Regarding the magnitude of these differences, large effect sizes were found in all cases. They ranged from d = .82 to 1.78 with the exception of the Grey Path (GP) scale that obtained a value of d = .33.
Table 2 Averages, typical deviations, and effect sizes for the different scalar scores obtained by male subjects in the clinical group and the control group
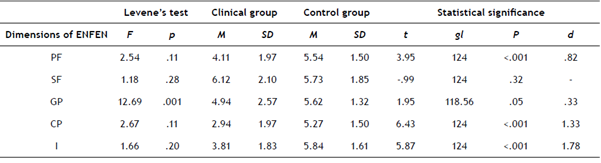
PF: Phonological fluency; SF: Semantic fluency; GP: Grey Path; CP: Colour Naming Path; I: Interference.
Table 3 shows the results for the mean differences in five of the ENFEN battery scales that were obtained by the female subjects in the clinical group and the control group. The results are very similar to those obtained from the male subjects as the clinical group scored significantly lower than the control group in all scales except for Semantic Fluency and Grey Path, for which the differences did not reach statistical significance. Regarding the magnitude of these differences, large effect sizes were found in all cases, ranging from d = .83 to 1.04. Since the results for both groups are very similar, we assume that the differences are due to the conditions of the control group or the clinical group and not to the sex.
Table 3 Averages, typical deviations, and sample effect sizes for the different scalar scores obtained by the females in the clinical group and the control group
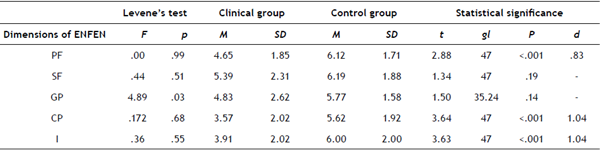
PF: Phonological fluency; SF: Semantic fluency; GP: Grey Path; CP: Colour Naming Path; I: Interference.
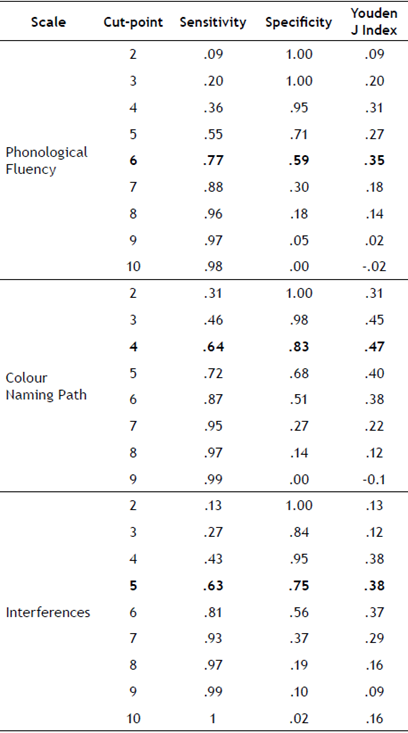
Lastly, using binary logistic regression, we found that the model is significant; this is shown by the dependent variable's range from .42 to .57. Furthermore, it correctly classifies 82.9% of cases; hence, we accept the model. An adequate functioning of Phonological Fluency, Colour Naming Path, and Interferences are associated with protection factors, that is, the subject would have a lower probability of being diagnosed with ADHD. The scales of Semantic Fluency and Grey Path do not increase the probability of being diagnosed with ADHD. Of all the variables, Colour Naming Path best explains an ADHD diagnosis.
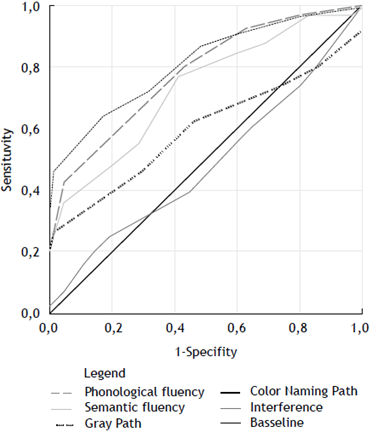
For the ROC curve analysis, the area under the curve is the following: PF=.73, CP=.81, and I=.78, all of which are significant. SF and GP do not have sufficient discriminant capacity.
The optimal cut-point takes into account the balance between sensitivity and specificity for CP=4, I=5 and PF=6 since these are the points that have the highest Youden J Index.
Discussion and conclusions
The executive functions (EF) concept encompasses a set of cognitive abilities that allow planning, programme development, goal setting, activities, and mental problems to be anticipated as well as self-regulation in goal-oriented tasks. The aim is to execute those tasks effectively (Parellada, 2009). As such, the main objective of the present study was to empirically test the usefulness and validity of the ENFEN battery (Portellano et al., 2009) as a tool to diagnose ADHD on the basis of the executive dysfunction that is presented by the individuals with this disorder.
Firstly, based on the presented results, we can conclude that there are significant differences in our sample between the clinical group and the control group. This is consistent with previous results obtained by Lozano et al. (2015) and Reyes, Barreyro, & Injoque-Ricle (2014) in their respective investigations. This demonstrated that the ENFEN Battery presents adequate sensitivity when discerning the execution level of executive functions with or without ADHD present.
On the other hand, the scales that have shown the lowest predictive value for ADHD are Grey Path and Semantic Fluency. This may be due to the fact that these are less demanding tests at the executive level since the former is based on a simple task being executed, which, while not being very novel, does demand sustained attention and vigilance. However, in Colour Naming Path, Inhibition, Cognitive Flexibility, and Working Memory, the executive system's psychological processes that are impaired by ADHD play a key role (Lavigne & Romero, 2010a). For Semantic Fluency, it is necessary to use semantic recovery processes (i.e. "words that belong to the semantic category of animals"). Semantic Fluency differs from analog Phonological Fluency for which the subject must retain a slogan (i.e. "name words beginning with the letter m") while accessing declarative memory semantically. Thus, the subject performs a search strategy using a complex language code. In addition, verbal fluency is the last of the executive functions that children develop (Jurado & Rosselli, 2007); it is only between 14-15 that verbal fluency reaches a level similar to that of an adult (Matute, Rosselli, Ardila, & Morales, 2004), which could explain the lack of differences with respect to the normative sample.
The presented results coincide with those of Lozano et al. (2015), who found that children between 6-12 have a high production of Semantic Fluency, regardless of their condition, and require less time to complete the Grey Path while achieving higher scores.
Regarding the interferences task, Reyes et al. (2014) note that the scale is non-significant. However, in the present study this has not been the case. The difference may be because the oldest child in the sample was 9 years old. This means that if there was a large number of 6 year-olds, the results shown by the subscale would be contaminated because, for there to be interference, there must be a good reading domain. If there is not a good reading domain, then the subject only identifies the colour of the word without encountering any variable that could modify that description.
Other studies have also found a relationship between the executive functions and ADHD while making the comparison using different scales. The interference test is derived from its predecessor: the Stroop test (Stroop, 1935; Golden, 2006). López-Villalobos et al. (2010) conducted a study on subjects diagnosed with ADHD and evaluated their performance using the Stroop test. The result was that the subjects presented a lack of flexibility and inhibitory control with respect to the control group. These findings coincide with those of Abad-Mas, Caloca-Catalá, Mulas, & Ruiz-Andrés (2017). In their study, Ramos and Pérez (2017) conclude that clinical subjects also commit a greater number of errors in the Go/No-Go task, which is the case in the experiment by Simon (1990). They also present a deterioration in all scales of the Behavior Rating Inventory of Executive Function (BRIEF) (Gioia et al., 2000). Pedreira and Peña (2011) used the Five Digits Test (FDT) (Sedó, 2007), which is an alternative to the Stroop test, and obtained the same results.
There is a Spanish-language test known as the TESEN (Spanish acronym) that is closely related to the Trail Making Test (TMT) (Reitan, 1992). In their paper, Frazier, Demaree, and Youngstrom (2004) analyse not only the TMT, but also many other tests that are highly related to the use of EF such as the aforementioned Stroop Test, the Rey Complex Figure (RCF) (Rey, 1987), or the Wisconsin Card Sorting Test (WCST) (Heaton et al., 2001). The results of the present study coincide with the results of previous studies; the finding is that there is a greater affectation in all of the tests for the subjects with ADHD.
In addition, Fenollar et al. (2015) conducted a study with subjects with ADHD using the WISC-IV test (Wechsler, 2003). The results highlight that, while the General Capabilities Index (GCI) is very similar in both the clinical group and the control group, significant differences appear in the Cognitive Competence Index (CCI). This is due to the fact that the indexes most linked to the disorder, which make up the ICC, are the Working Memory Index and the Processing Speed Index: processes that require a greater demand for Executive Functioning (Bustillo & Servera, 2015; Mayes & Calhoun, 2006; Navarro, Fenollar, Lavigne, & Juarez, 2017).
The limitations of this study include that, given the collected data is part of a screening process for ADHD, the intervention teams by way of a technical decision used the predecessor of the Rings (R): the Tower of Hanoi (Simon, 1975). This made it impossible to compare these means with the rest of the data. Conversely, although the sample size is considerable, the representativeness is limited. Hence, in future studies it would be interesting to expand the work using a greater number of participants.
Therefore, from the perspective of the present work's results, it can be concluded that children with ADHD tend to present a characteristic performance profile in the ENFEN battery; this is something that has already been verified both with this test and other similar ones for different disorders. (Garcia & Rubio, 2011; Ortiz et al., 2013). The practical implication of this is the assumed support that the presented data offers for the clinical diagnosis that is carried out in mental health units as well as the instruments having an educational orientation. In addition, it helps professionals in a school environment to become more aware of which areas of cognitive development a student diagnosed with ADHD will have more difficulties in. And, by doing so, they can take more adjusted and effective psychopedagogical measures when it comes to supporting the student in their adaptation to the school environment.
In future research, it would be interesting to establish the test profile differences for the different subtypes of the disorder and their comorbidities as well as making a comparison with other tests that have the same characteristics.

