











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
Permalink
Introduction
Chilean epidemiological studies have revealed a high total prevalence (tp) of mental disorders in the child-adolescent population (Ministerio de Salud, 2013; Vicente et al., 2012a, b). Tp reaches 38.3% (4 to 18 years old), and only decreases to 22.5% when considering the most stringent impairment algorithm (ip impairment prevalence), according to the diagnostic interview schedule for children, version IV (DISC-IV). Among the most common mental disorders in this population, anxious (tp = 18.5%, ip = 8.3%) and affective disorders (tp = 6.1%, ip = 5.1%) have, in both cases, higher prevalence than those observed globally between 6 and 18 years old (Polanczyk, Salum, Sugaya, Caye & Rohde, 2015; Vicente et al., 2012a, b).
One of the instruments that allows measuring anxiety and depressive mood levels quickly, easily and reliably is the Hospital Anxiety and Depression Scale (HADS). This instrument detects possible cases of anxious or depressive disorders in the general hospital context (not psychiatric), in a brief self-report format to be applied in the period in which patients wait to be seen by their doctors (Zigmond & Snaith, 1983). A particularity in the items selection of the HADS is the exclusion criteria of common symptoms between physical and emotional disorders, so that the scores obtained would not be affected by the physical illnesses of the patients. Nevertheless, the utility of the HADS went beyond medical settings, and tested to be a feasible instrument with individual with non-physical problems (Cosco, Doyle, Ward & McGee, 2012: Norton, Cosco, Doyle, Done & Sacker, 2013).
HADS has also been adapted, validated and used in the global infant-juvenile population, both in clinical and non-clinical samples, being a suitable instrument for screening general authors that this scale has been adapted in the Chilean children and adolescent population, despite having been used with Chilean adolescents (Bonhauser et al., 2005). Also, several investigations show variations on anxiety or depressive mood levels in children and adolescent populations according to variables like age, grade, sex or type of school (Cumsille & Martínez, 1997; Gaeta-González & MartínezOtero, 2014; Britos Esquivel, 2017; González-Salazar, Timón-Guzmán & Riveros-Munévar, 2015; Ospina, Hinestrosa, Paredes, Guzmán & Granados, 2011), which could be useful for identifying risk groups.
Based on the aforementioned background, this research was aimed at adapting and studying the factor structure of the HADS in a representative sample of Chilean children and adolescents. This study also aimed to identify risk groups that might present higher levels of anxiety and depressive moods, which therefore could have a greater probability of developing the associated disorders.
Method
Sample
The sampling used was of a multi-stage type (confidence level: .95), carried-out on schoolchildren from Concepción, Chile. Three main strata were taken into account, corresponding to the three types of schools present in Chile (municipal, private-subsidized and private non-subsidized), sampling being carried out by conglomerates (schools). The final sample consisted of 467 schoolchildren from fourth to the eighth grade, between 8 and 16 years old (average: 11.4 (s.d. = 1.69), from 3 municipals (37.90%), 3 private-subsidized (29.12%) and 2 private non-subsidized (32.98%) schools, representing a 3.20% of the total number of schoolchildren in this educational range in the city of Concepción.
In cognitive interviews, 10 fourth and fifth grade school children, aged 9 to 11 years old (average: 10.00 years old (s.d. = .80)), belonging to two private subsidized-schools participated. There was no need to include 8 years old, as they were about to turn 9 in the next few days.
The samples used for test-retest with an interval of two weeks and one month, consisted of 126 school children from fourth to the eighth-grade, between 9 and 16 years old (average: 11.13 (s.d. = 1.49), 58.73% girls), belonging to 3 schools (1 municipal (23.81%), 1 private subsidized (50.79%) and 1 private non-subsidized (25.40%)), and 227 schoolchildren from fourth to the eighth grade, between 8 and 15 years old (average: 11.1 (s.d. = 1.61), 44.49% of girls), belonging to 4 schools (1 municipal (43.61%), 2 privatelevels of anxiety and depression in this population (e.g., Thabrew, McDowell, Given & Murrell, 2017). Despite its frequent use, one of the problems encountered is the stability of the HADS’ factor structure, similar to that observed with adult samples (Cosco et al., 2012; Norton et al., 2013). The most common consists of a two-factor structure, anxiety and depression (Ambaw, 2011; Chan, Leung, Fong, Leung & Lee, 2010; Mihalca, 2014; Valero-Moreno et al., 2019; White, Leach, Sims, Atkinson & Cottrell, 1999). Nevertheless, some authors have reported a unique global distress factor (Johnston, Pollard & Hennessey, 2000; Razavi, Delvaux, Farvacques & Robaye, 1990). Others have reported a three-factor structure based on the tripartite model, including autonomic anxiety, negative affect and depressive mood (Saez-Flores, Tonarely, Barker & Quittner, 2018).
On the other hand, until now, although the scale hasbeen adapted for the Chilean adult population (Villoria & Lara, 2018), presenting an adequate internal consistency (a anxiety = .76; a depression = .84) it is not known to the subsidized (27.75%) and 1 private non-subsidized (28.63%)), respectively.
All participants expressed their willingness to be a part of this study, after signing an Informed Consent together with their parents. The present research was approved by the Ethics Committee of the Psychology Department, from the Universidad de Concepción (ref. 04112016).
Instruments
Hospital Anxiety and Depression Scale, by Zigmond and Snaith (1983), Spanish version (De las Cuevas, García-Estrada & González, 1995). The scale consists of 14 items, with a 4-point Likert response format, seven for anxiety, and seven for depressive mood levels, as experienced during the last week. Regarding its reliability, the average values are a =.83 and a=.82 for the sub-scales of anxiety and depressive mood, respectively (Bjelland, Dahl, Haug, & Neckelmann, 2002). Specifically for the infant-juvenile population, internal coefficient values where around a =.80 for anxiety items, and a =.65 for depressive mood items (Ambaw, 2011; Chan et al., 2010; Mihalca, 2014).
The study was divided into four phases:
(1) Cognitive interviews
Previous to the cognitive interviews, a panel of five experts from the fields of psychology, psychiatry and education were recruited to analyse the HADS contents, its pertinence and response format adequacy. As a consequence, response options were simplified (response options were changed to “Never”, “Sometimes”, “Several times” and “Always or almost always”), maintaining the 4-point Likert format.
Cognitive interviews were carried out to detect problems both in item comprehension and response difficulties, usually associated with children and adolescents (Briceño et al., 2016). Ten children, from fourth and fifth grade, were interviewed. Participants were instructed to read the HADS aloud and ask any questions they could have about the instructions, questions and response options. They were also told that they would be asked questions while they were answering the instrument, in order to check their comprehension. Interviewers used paraphrasing, specifying, comprehension, interpretation, and general exploration techniques to check if the instrument was adequately understood and answered (Smith & Molina, 2011; Willis, 2005). The information was recorded in audio format, to be destroyed later, in order to safeguard the confidentiality of the data.
(2) Confirmatory factor analysis
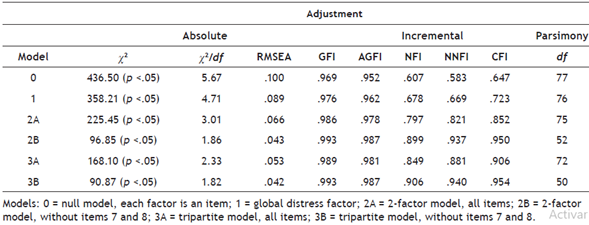
The final version of the HADS was applied to the total sample (N=467), after which confirmatory factor analysis (CFA) was carried out, by using the maximum likelihood estimation method and covariance matrix. The CFA considered 6 models, with acceptance of covariances, which included the presence of 1, 2 and 3 and factors, and a null model. Model 0 was the null model, where each item is a factor, and given that this model was not verified, the other models were studied. Model 1 consisted of a factor of global distress, the two-factor models considered the classic model of anxiety and depressive mood, with (2A) and without (2B) the total of the original items, the three-factor models considered the structure of the tripartite model, with (3A) and without (3B) the total of the original items.
Goodness of fit was assessed according to: absolute adjustment (Chi square (χ2), Chi square/Degrees of freedom (χ2/df), Goodness of fit index (GFI), and Root mean square error of approximation (RMSEA)), incremental adjustment (Adjusted goodness of fit index (AGFI), Normal adjustment index (NFI), Adjusted non-regulated index (NNFI), Comparative adjustment index (CFI)) and adjustment of parsimony (Degrees of freedom (df)) (Lévy, Fuentes & González, 2006). As adjustment indicators we considered: (1) values of χ2 with p values lower than .05 as an indicator of good adjustment; (2) values of χ2/df lower than 2 as an indicator of an excellent adjustment, and between 2 and 5 as a reasonable adjustment (Bollen, 1989; Escurra-Mayaute & Salas-Blas, 2014; Tabachnik & Fidell, 2019); (3) RMSEA values less than .05 as indicators of an excellent fit, and between .05 and .08 as an acceptable adjustment (Browne & Cudeck, 1993; Byrne, 2010; Hu & Bentler, 1999; Lévy et al., 2006); (4) values of GFI, AGFI, NFI, NNFI and CFI close to 1 as an indicator of good fit (Browne & Cudeck, 1993; Byrne, 2010; Lévy et al., 2006; Martínez-López, Conchado-Peiró, Andreu-Vaillo & Galdón-Garrido, 2019); and (5) higher df values with respect to the rest of the models (Lévy et al., 2006). In case the adjustment indicators were highly similar, the choice of the best model corresponded to the most parsimonious, as indicated by higher degrees of freedom (Mulaik, 1998). Once the CFA was performed, the normality of the data was analysed by means of the KolmogorovSmirnov test, which indicated non-normal distributions for both sub-scales (Z anxiety = .15, Z depressive mood = .10, p < .01).
Reliability was determined through Cronbach’s alpha, which was interpreted as questionable (.60<a<.70), acceptable (.70<a<.80), good (.80<a<.90) or excellent (.90<a) (George & Mellery, 2003). Additionally, the correlation between sub-scales was studied by calculating Spearman’s coefficient. Both measurements, Cronbach’s alpha and Spearman’s coefficient, were obtained for the total sample, for the subgroups of girls and boys, children (8 and 9 years old), early adolescence (10-13 years old) and middle adolescence (14-16 years old) (Gaete, 2015). The possible differences between these measurements were studied through the cocron function (Diedenhofen & Mush, 2016) and Fisher’s transformation, respectively.
(3) Test-retest with 2 weeks and 1-month intervals
Temporal stability was analysed through test-retest, with intervals of 2 weeks and 1 month, using the non-parametric Spearman correlation analysis. The correlation ranges used corresponded to low (from .00 to .25), weak (from .25 to .50), moderate (from .50 to .75) and strong (from .75 to 1.00) correlations (Martínez, Tuya, Martínez, Pérez & Cánovas, 2009).
(4) Characterization by sociodemographic variables
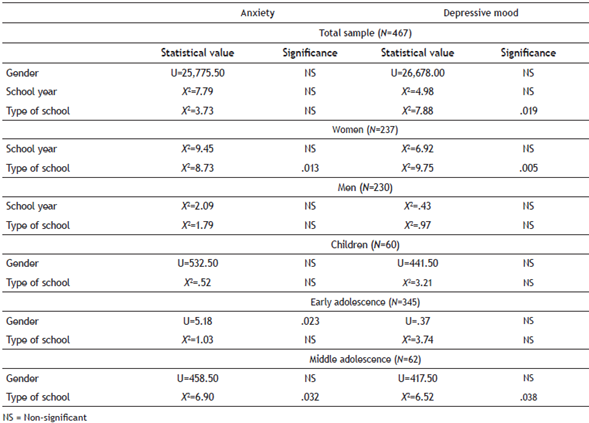
To characterize the variables under study, the nonparametric tests of Mann-Whitney´s U (gender) and KruskalWallis (school year and type of school) were used, as general scores of anxiety and depressive mood were not normally distributed. In the case of the Kruskal-Wallis test, in those variables that indicated significant differences, a posthoc analysis was performed, applying the Bonferroni correction, to prevent obtaining random significant differences. Regarding age, the Spearman correlation coefficient was used, considering the total sample, as well as its division into boys and girls, children, early and middle adolescence, and the possible differences between the correlations were studied through r to z Fisher’s transformation.
The data analysis was carried-out using the statistical package SPSS v23 and in the case of the CFA, this was done using the RStudio software.
Results
(1) Cognitive interviews
The application of cognitive interviews led to the modification of 8 items, most of which consisted of replacing words whose meaning was not clear with synonyms that were effectively interpreted. Some of these changes included modifying “I feel optimistic about the future”, to “I thought things would turn out well”, since the word “optimistic” was not understood. Another modification was in the item “sudden feelings of panic assault me” for “sudden feelings of panic or a lot of fear come to me”, since the use of the word “assault” confused some of the participants, and the word “panic” generated some doubts about its meaning.
(2) Confirmatory factor analysis
Models 0 and 1 did not present adequate values of absolute and incremental adjustment. When testing the models of 2 (2A) and 3 (3A) factors, in both cases 2 items were identified (items 7 and 8) as not being grouped in the correct factor. Based on the above, the same models were tested, but eliminating those items (2B and 3B). The best models, according to indicators of absolute and incremental adjustment, were Models 2B and 3B, and between these two, the best was the classic of two factors, since it was the most parsimonious (Table 1).
Reliability analysis of both sub-scales was performed, by calculating Cronbach’s alpha. General coefficients for the total sample were a =.75 for anxiety items, and a =.65 for depressive mood items; when analysing the alphas according to gender (a anxiety =.84 and a depressive mood =.68, in girls; a anxiety =.76 and a depressive mood =.62, in boys), significant differences were observed according to the cocron function only in the alpha for anxiety items (a2 = 6.77 (p <.05)). The analysis of the alphas according to groups of children (a anxiety =.71 and a depressive mood = .58; N = 60), early adolescence (a anxiety = .76 and a depressive mood = .60; N = 345) and middle adolescence (a anxiety = .87 and a depressive mood = .80; N = 62), indicated a tendency for greater reliability as age increased, in addition to significant differences in the anxiety alpha of the groups of children and middle adolescence (x2 = 6.68 (p <. 05)), in the alpha of depressive mood among children and early adolescence (x2 = 7.46 (p < .05)), and among children and middle adolescence (x2 = 13.84 (p < .05)).
Additionally, Spearman’s coefficient was calculated (r =.07, p>.1), not observing a significant correlation between both scales in the total sample or when analysing by gender or age group.
(3) Test-retest with 2 weeks/1month intervals
Test-retest analysis with a 2-week interval indicated positive and significant correlations of .67 (p<.001) and .43 (p<.001) for anxiety and depressive mood, respectively. In the 1-month interval, coefficient levels were similar to those observed in the 2-week interval (.64 and .49, respectively).
(4) Sociodemographic variables characterization
The Mann-Whitney U and Kruskal-Wallis tests initially only indicated differences in depressive mood levels in the total sample, when analysing according to type of school. The differences according to type of school indicated higher levels of depressive mood in municipal schools with respect to private subsidized and non-subsidized schools, and after. post-hoc analysis the difference between municipal and private non-subsidized schools was maintained.
After analysing the total sample, the possible differences within the groups of boys and girls were analysed separately. Regarding the type of school, lower levels of anxiety and depressed mood were observed in girls and adolescents attending private non-subsidized schools, with respect to those attending municipal and private subsidized schools, and after post-hoc analysis only the differences between private-subsidized and municipal schools were maintained. When studying how sociodemographic variables behaved according age group, it was found that in children (younger than 10 years old) there were no differences, whereas in early adolescence only gender differences were observed in anxiety levels (higher levels in girls), whereas in the middle adolescence, differences were observed according to the type of school for anxiety levels (higher in municipal compared to private subsidized schools according to post-hoc analysis) and depressive mood (initially higher in private subsidized schools compared to non-subsidized schools; however, this is not maintained after post-hoc analysis) (Table 2).
Regarding age and its relationship with anxiety and depressive mood levels, the Spearman coefficient indicated significant correlations only in anxiety levels, with values of .12 in the total sample, .15 in girls (p < .05), and a nonsignificant correlation in boys.
Discussion
On the present study the HADS factor structure was examined on a Chilean child-adolescent sample, considering the need for having highly efficient instruments that are able to identify emotional problems linked to anxiety and depression, within a population that currently has a high prevalence of mental disorders.
The validity assessment of the adapted HADS by means of CFA indicated that the most appropriate model, consisted of the classic two-factor model (anxiety and depressive mood), which has also been reported in most of the studies conducted in children and adolescents (Ambaw, 2011; Chan et al., 2010; Mihalca, 2014; White et al., 1999), as well as in other age ranges (Bjelland et al., 2002) compared to the three-factor model (tripartite model), which has been less represented (Saez-Flores et al., 2018). The fact that 2 items needed to be eliminated (7 and 8) also corresponds to other studies carried out in the adolescent population, which indicate that these items would also present problems (Ambaw, 2011; Chan et al., 2010; Mihalca, 2014; Mihalca & Pilecka, 2015; Valero-Moreno et al., 2019; White et al., 1999).
Regarding reliability, the anxiety subscale attained an acceptable internal consistency, whereas the depression subscale, despite obtaining a coefficient close to .70, its internal coefficient is questionable. These data were similar when analysed by gender, but tended to be higher as age increased. These values were similar to those reported in other studies with non-clinical child or adolescent population, which in the sub-scale of anxiety indicates values around .80, while the sub-scale of depressive mood attained lower values than the anxiety sub-scale. Also, greater variability was observed with depressive mood items (Ambaw, 2011 (a anxiety = .80 and a depressive mood = .77), Chan et al., 2010 (a anxiety= .80 and a depressive mood = .63); Mihalca, 2014 (a anxiety = .80 and a depressive mood = .49)). As evidenced by the data, the depression subscale contents need a more exhaustive analysis, and eventually, if there is an intrinsic variability in depressive symptoms as part of depression nature and its life-span development (GarcíaVelázquez, Jokela & Rosentröm, 2019; Schaakxs et al., 2018; van Eeden, van Hemert, Carlier, Penninx & Giltay, 2019).
Both sub-scales were not significantly correlated, which differs from other studies in children and adolescents where moderate weak positive correlations have been found (Ambaw, 2011; Chan et al., 2010; Mihalca, 2014; White et al., 1999). This could be due to the fact that in the present study, items 7 and 8 that were loaded into the opposite sub-scales were eliminated, which, when included in other studies, could lead to significant positive correlations.
The test-retest analysis of the HADS indicated that the anxiety sub-scale would possess an appreciable stability, with lower levels for the depressive mood sub-scale. A similar study with test-retest applied with an interval of 1 week indicated a moderate stability in both cases (Mihalca, 2014). Regarding sociodemographic variables, for anxiety levels, it was found that: (1) during early adolescence, girls have higher levels than boys, and (2) in middle adolescence the type of school indicates differences, with higher levels in those who attend municipal schools, than those who attend private non-subsidized schools.
In the case of depressive mood levels, it was observed that: (1) there are higher levels in girls attending municipal schools than in those attending private non-subsidized schools, and (2) during middle adolescence there are higher levels in those who attend municipal schools with respect to private non-subsidized schools.
Considering gender differences in anxiety levels during early adolescence (higher in girls), studies have reported similar results (Chan et al., 2010; Gaeta-González & Martínez-Otero, 2014; White et al., 1999), which is also associated with a higher prevalence of anxious disorders observed in Chilean girls (4-18 years old, Vicente et al., 2012a,b). As for the absence of gender differences during childhood, this may be due to anxiety levels being similar in both girls and boys; however, once puberty starts (in late childhood) this might influence the anxiety levels of girls for the most part, which is especially reflected during early adolescence (Reardon, Leen-Feldner & Hayward, 2009). This might also be supported by the positive correlation between age and anxiety levels observed in the girls that participated in the present study.
With regards to the absence of gender differences in depressive mood levels (in the total sample and in the groups of children, and early and middle adolescence), the results of the present study differ from the trend observed in other studies, which indicate higher levels in girls (Chan et al., 2010; Cumsille & Martínez, 1997; Fernandez & KrönerHerwig, 2013; Ge, Conger & Elder, 2001; Hankin, 2009; White et al., 1999).
In the case of the school year of participants, the absence of significant differences in anxiety and depressive mood levels, as well as the poor correlation only in anxiety levels in girls, might indicate that, in general, both symptomatology would occur in the same degree during the course of adolescence in the general population (González Salazar et al., 2015), differing from the prevalence patterns observed in the associated mental disorders (Angold, Costello & Worthman, 1998; Copeland, Angold, Shanahan & Costello, 2014; Costello, Mustillo, Erkanli, Keeler & Angold, 2003; Fleitlich-Bilyk & Goodman, 2004; Ford, Goodman & Meltzer, 2003; Green, McGinnity, Meltzer, Ford & Goodman, 2004; Hankin et al., 2015; Vicente et al., 2012a and b; Wickramaratne, Wessman, Leaf & Holford, 1989).
Analysis by type of school indicated that depressive mood levels were higher in municipal rather than private non-subsidized schools, and that anxiety levels only differed according to the type of school during middle adolescence, where again municipal schools would present higher levels than private non-subsidized schools, similar to what has been observed in Colombian students (Ospina et al., 2011). This study has several limitations, such as the sample size and the fact that psychometric analysis in a clinical population was not included, where the cut scores that could distinguish possible or probable anxiety and depressive disorders might have been obtained, as well as a comparison of the reliability of the instrument between both populations.
Future research could examine the psychometric properties of the infant-juvenile clinical population, and contrast the characteristics of the instrument with other variables measured during late adolescence and early adulthood.
Conclusions
Based on the obtained results, it is concluded for the adapted HADS instrument, that it is better represented by a two-factor structure (anxiety and depressive mood). The anxiety sub-scale is reasonably reliable in both children and adolescents, while the depressive mood sub-scale is more reliable during middle adolescence.
In girls, anxiety levels increase between middle childhood and adolescence, and there are differences in anxiety and depressive mood levels among female students from municipal and private non-subsidized schools, especially in the former.

