











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Despite the progress recorded in combating HIV and sexually transmitted infections (STIs) over the past two decades, these are still a challenge for many Latin American countries. New infection rates increased by 21% from 2010 to 2019 compared to the Caribbean countries, Central Africa, Europe, and North America, where it decreased significantly (UNAIDS, 2020), In addition, lockdowns, economic restrictions and social isolation associated with the COVID-19 pandemic are having a negative effect on vulnerable populations, including people living with HIV in Latin America (UNAIDS, 2022). A major disparity is the application of strategies that strengthen protective sexual behaviours among populations according to a specific risk. In Colombia, between February 2020 and July 2021, 13864 patients with HIV were diagnosed, which means a reduction of 26.48% compared to the previous year. Of the new cases, 63.09% indicated that they belonged to one or more key population groups and the main mechanism of transmission continues to be sexual (91.24%) (Cuenta de alto costo. Fondo Colombiano de Enfermedades de alto costo, 2022).
In addition, the World Health Organization (2018) estimated that more than 1 million people worldwide have acquired a STI, and there are estimated to be about 376 million new cases registered in 2016, also more than 500 million people worldwide had the herpes simplex virus, and more than 290 million women had human papillomavirus. In Colombia for the year 2011, the last with available data, 9324 people were treated for syphilis; 2788 for gonorrhea; 1313 for chlamydia; 1723 for lymphogranuloma venereum (LGV); 1995 for trichomoniasis; 9766 for herpes; 18221 for anogenital warts; 1279 for hepatitis B; and 19478 by papilloma virus. The highest prevalence was in females from 20-29 years of age (Ministerio Nacional de Salud, 2011). Finally, teen pregnancy is another challenge for Latin American countries. According to the (World Health Organization, 2021) in 2020, the global birth rate was 41 per 1000 in women from 15 to 19 years of age; Unfortunately, in Colombia this rate was even higher, 63 per 1000 women.
The highest rates in Colombia for these three major problems suggests that sex education programmes are not effectively applied or have low efficacy (DeMaria et al., 2009; Ivanova et al., 2016; Nelson et al., 2015). Studies with Colombian youth showed higher scores in the CUES (Condom Use Errors/Problems Survey) that indicate higher rates of errors and problems, a strong influence of cultural beliefs such as machismo due to the traditional practices of couple formation and gender roles on the Colombian coast, the effect of a partner’s disapproval in condom use, and lesser female condom use compared to men (Gómez-Lugo et al., 2020; Morales et al., 2018, 2019; Sanchez-Mendoza et al., 2020).
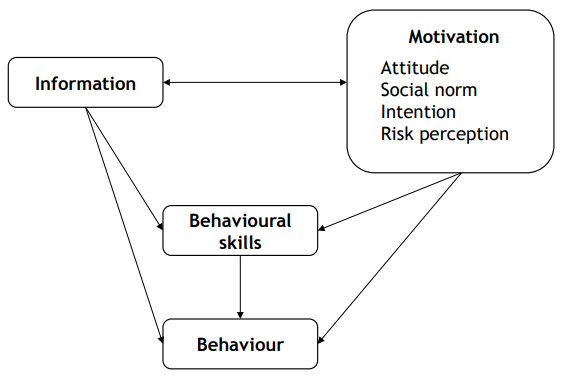
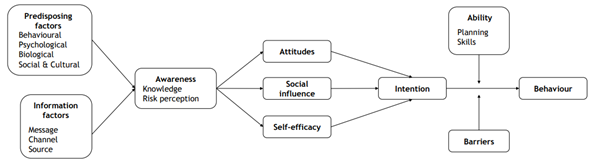
According to the information-motivation-behavioural skills model (IMB) (Fisher et al., 1994) (see Figure 1) and the integrated model for explaining motivational and behavioural change or the I-Change model (ICM) (De Vries et al., 2005) (see Figure 2), self-efficacy, attitudes, and knowledge are the main variables in predicting sexual health promotion among young people and influencing health behaviour and both have been widely used to predict and promote them, coming from personal beliefs to cultural and community practices that impact the overall quality of life (Espada et al., 2014; Jiang et al., 2019; Xu et al., 2017; Yu et al., 2018). HIV/AIDS knowledge and condom self-efficacy form a self-enhancement system over time in which HIV/AIDS knowledge is significantly and causally related to the intention to use condoms through a process mediation of multiple pathways, and self-efficacy and the intention to use condoms during sex forms a positive feedback loop (Chen & Chen, 2022; Negash et al., 2021)
However, there is a significant gap in knowledge regarding HIV/STIs among adolescents due to several erroneous beliefs concerning the inability to experience sexual satisfaction when using condoms, a lack of condom self-use efficacy, misconceptions with respect to the pathways of HIV spread and prevention, and certain differences between gender and immigrant status (Butts et al., 2018; Mahat, 2019; Von Rosen et al., 2018).
In Colombia studies showed that adolescents had a moderate to low level of knowledge with reference to sexual health, due to reported misconceptions about HIV, no perceived HIV risk, reported low self-efficacy in order to prevent the infection, religious beliefs that influenced the decision-making for HIV prevention, and erroneous beliefs regarding the relationship between alcohol consumption and condom use self-efficacy (Cardona-Duque et al., 2015; Castillo-Ávila et al., 2017; Gómez-Lugo et al., 2020; Morales et al., 2018; Rengifo-Reina et al., 2012; Sanchez-Mendoza et al., 2020).
Previous results have shown the importance of recognising what adolescents understand regarding HIV and how to prevent its spread (Gómez-Lugo et al., 2022). The present study has aimed to evaluate the knowledge of HIV and other STIs among Colombian adolescents, to contribute to the characterisations of the Colombian and Latino populations, and to contribute to strengthening school-based health prevention programmes.
Methods
Participants
The project was approved by the ethics and scientific committees of the participating universities. Schools were located in middle-low-income neighborhoods. Some of them were public schools, which meant the tuition fee was at a government-subsidised rate. A total of 2012 adolescents participated in this study and completed the sociodemographic and KSI questionnaires. Inclusion criteria were (a) they had their parent/legal tutor sign the informed consent sheet, (b) they had signed an informed assent, (c) they studied in a school that signed a research participation agreement, (d) they were between 12 and 19 years of age, and (e) they were able to read and write in Spanish.
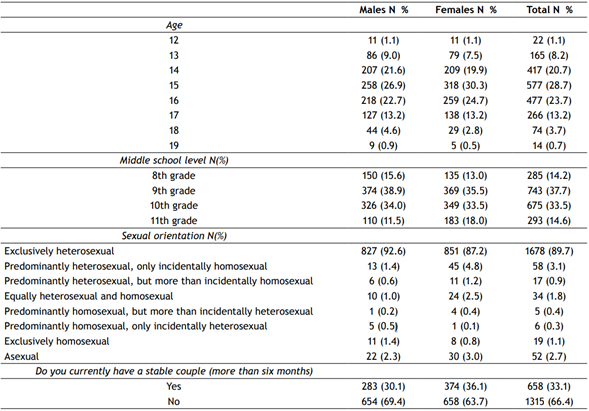
The mean age of the participants was 15.24 years (SD = 1.33). A total of 52.1% (n = 1048) were females and 47.9% (n = 960) were males. No significant differences were observed between sex and age or whether they had a stable romantic partner but differences were observed in sexual orientation (χ2 = 75.92 (14); p < .01; η = .13) and educational level (χ2 = 18.85 (6); p < .01; η = .09). The characteristics of the samples are listed on Table 1.
Instruments
Sociodemographic Variables. An ad hoc questionnaire was created to assess sex, age, nationality, city of residence, educational level, sexual orientation, and whether they had a stable romantic partner. The questionnaire had previously been used in a Colombian context (Morales et al., 2018).
The HIV and Other Sexually Transmitted Infections Knowledge Scale (KSI, Espada et al., 2014). This instrument comprised of 24 items that evaluated aspects related to knowledge of HIV and other STIs. It was developed in Spain and adapted for Colombia. It was answered on a “know” or “do not know” scale. Items are grouped into five subscales: (a) overall HIV knowledge, (b) condom knowledge, (c) HIV transmission knowledge, (d) knowledge about other STIs, and (e) HIV prevention knowledge. Reliability indices in Colombia ranged from .64 to .87. In the current study, Cronbach alphas ranged from .75 to .86.
Procedure
The KSI required an informed consent from the parents and requested an informed assent from the adolescents and was self-administered in classrooms using a printed form. Psychologists and psychology students accompanied the process. The process lasted 25 minutes and was voluntary and anonymous, hence, teachers were not present in the classroom during the evaluation, and parents did not know the answers. The maximum number of students evaluated per group was 35.
Data Analysis
All analyses in this study were performed using the R language and Rstudio (R Core Team, 2022). The use of the packages ggplot2 (Wickham, 2016) and ggstatsplot (Patil, 2021) is highlighted.
Results
The average score was 41.32% (SD = 22.65), and in the range from 0 to 24, the observed mean was 9.90 (SD = 4.64). This indicated a rather moderate to low average knowledge.
As shown in Figure 3, the percentage of success and error in the items was variable. In general, adolescents failed many questions on the subscale of other STIs. Some items stood out, such as question 15, in which 75% of adolescents did not know whether a tongue-kiss led to HIV infection, and question 11, in which 82% of adolescents did not know whether the vaginal ring and the Copper T were both effective methods for preventing HIV/AIDS. Additionally, almost half of the adolescents did not know whether contraceptive pills prevented HIV, but they knew that HIV could be transmitted through sexual pathways.
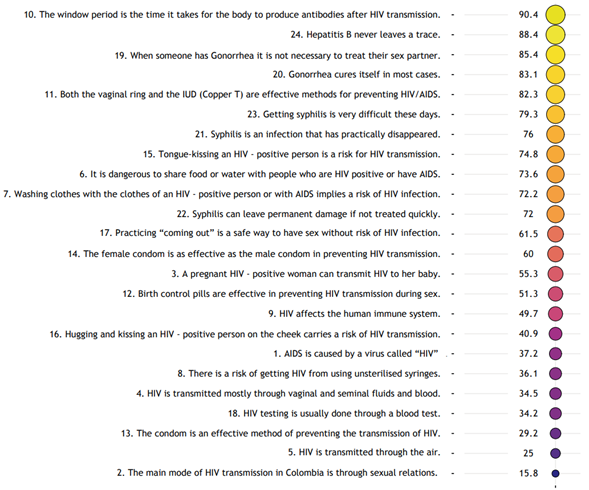
Note. Participants knowledge regarding HIV and other STIs is shown.
Figure 3 Heat map of the percentage of known/not known items answered
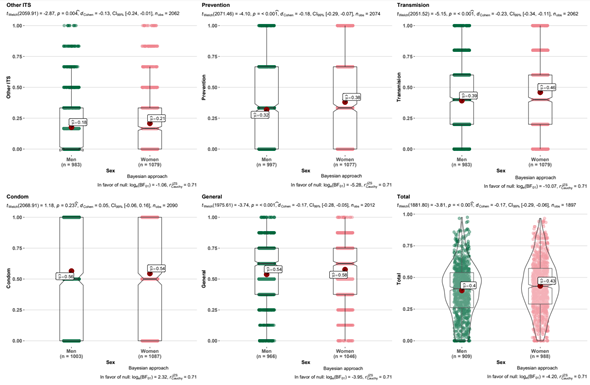
Finally, Figure 4 shows the fields in which sex education should concentrate the most. Questions regarding other STIs or HIV prevention and transmission were the dimensions with the greatest accumulation of error. Some differences were also found by sex (except for the condom dimension), where women showed more knowledge than men. However, the small effect sizes observed did not suggest differentiated interventions.
Discussion
The present study shows that Colombian adolescents have moderate to low knowledge of HIV and other STIs. Using the KSI (possible scores ranging from 0 to 24), the group mean level of knowledge regarding HIV and other STIs in our sample was considered moderate to low, M = 9.90 (SD = 6.64). This result was consistent with the baseline level of knowledge on HIV and other STIs reported in other studies performed with the participation of a Colombian sample of equivalent sociodemographic characteristics (Abello-Luque et al., 2021; Cardona-Duque et al., 2015; Castillo-Ávila et al., 2017; Morales et al., 2018; Rengifo -Reina et al., 2012)
However, the level of knowledge with respect to HIV and other STIs of Colombian youth is significantly lower than that reported in studies that used the same instrument (KSI) in adolescents in Spain, due to the application of a prevention programme (COMPAS) that includes a description of how HIV affects the body, a self-talk activity, a guided visual imagery activity, and styles of communication applied to dealing with risky sexual situations (e.g., assertive, passive, and argumentative) aimed at school students (Espada et al., 2017; Espada, Escribano, et al., 2015; Espada, Morales, et al., 2015).
Knowledge regarding HIV and other STI transmissions and prevention in the adolescent population is an important feature of sexual behaviour and health. However, it might not be sufficiently protective in and of itself, because the behavioural component made up of actual skills as well as the perception of self-efficacy is a model component that also determines the adolescent’s self-care behaviour (Fisher et al., 1994).
Inadequate knowledge of STI protection practices is a risk factor for lack of condom use in the adolescent population, (Espada, Morales, et al., 2015; Morales et al., 2018) and misconceptions can result in unprotected sex with an infected partner and early sexual intercourse initiation due to an incorrect self-confidence of invulnerability (Lescano et al., 2020; Ma & Malcolm, 2016).
In this study, some differences have been found by gender, being that women had a slightly higher the knowledge than men (except for condom dimensions), possibly due to the active role of parents in the sexual education of daughters and in the educational processes of schools aimed at preventing early pregnancy focusing on female adolescents. However, the small effect sizes do not suggest differentiated interventions. Other studies showed similar results (Cardona-Duque et al., 2015; Castillo-Ávila et al., 2017; Espada, Morales, et al., 2015).
There is evidence that knowledge regarding HIV and other STIs is lower in the new generations of young people than in the previous generations, even though more information is currently available (Espada, Escribano, et al., 2015). These results suggest a scarcity of interventions to promote sexual health and that those that are implemented do not achieve the expected results (DeMaria et al., 2009; Ivanova et al., 2016; Nelson et al., 2015).
New interventions should involve parents and school community members in order to share clear and reliable information with respect to HIV/STIs at both homes and schools and find spaces for safe conversations concerning these topics in places with strong cultural and religious beliefs, without stigmatisation or discrimination against adolescents. Training in condom use also needs to be strengthened, emphasising that this does not promote early sexual intercourse initiation in adolescents.
This study has strengths related to data analysis, multicultural population, participants in different stages of adolescent development, and equivalence in the male and female samples, which contribute to the understanding of the state of knowledge of Colombian adolescents in a broad way and strengthens prevention strategies carried out by different professionals linked to the field of quality of life, education, and sexual healthcare.
Limitations
The main limitation of this study is the sampling. Since, it is a non-randomized sampling, conclusions should not be generalized to other populations. Thus, the results should be interpreted with caution. In addition, students who did not attend the lectures, probably those with the most gaps in knowledge regarding this topic, were not evaluated. Finally, we underscore the use of self-report measures, because participants may make the more socially acceptable answer rather than be truthful, and the answers may be related to recent or significant experience and other factors.
Conclusion
Existing literature on the knowledge regarding HIV and other STIs in adolescents showed moderate to high levels in developed countries. In Colombia, the results showed a moderate to low knowledge. Some reasons can be related to the lack of a policy regarding adolescent sexual healthcare and gaps in state policies on sex education in schools. Colombia’s great challenge is to coordinate economic and social development and targeting resources, contributing to eradicating inequality in access to health promotion and prevention services.
This study showed the relevance of strengthening school-based programmes in which parents and teachers break gender stereotypes, wrong beliefs, and cultural practices that affect rational decision-making with regard to adolescent sexual behaviour. In addition, there are some differences in knowledge between genders, but we did not find a size effect that indicated the need for differential training. It is imperative to instruct adolescents on the proper use of a condom, the use and effects of birth control pills, and finally, the promotion and prevention services available in the country1.

