











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
Permalink
Major depressive disorder (MDD) is one of the leading causes of disability and one of the most prevalent mental disorders worldwide. According to the World Health Organization, depression affects nearly 280 million people (WHO, 2021), corresponding to at least 3.76% of the worldwide population (Global Health Data Exchange, 2019). In Colombia, the National Survey of Mental Health (Ministerio de Salud y Protección Social, 2015) found that prevalence rates were 4.3% for major depressive disorder, 1% for minor depression, and 0.5% for dysthymia. These alarming facts underscore the importance of identifying and understanding the etiological and vulnerability factors of MDD to develop more accurate preventive and intervention programs.
Multidimensional theoretical models have been pro-posed to explain the development of MDD (Beck & Bredemeier, 2016). Factors such as a) early trauma experiences; b) information processing biases, such as attributional and inferential styles; c) cognitive schemas; d) biological stress reactivity; and e) genetic risk factors, all have been associated with a predisposition toward developing MDD (Beck & Bredemeier, 2016). However, the design of these studies tends to center on exploring the effects of only one risk fac-tor at a time and are usually measured in samples of healthy or subclinical participants (Hovens et al., 2012; Nelson et al., 2017; Sanjuán & Magallanes, 2007; Soria et al., 2004; Spinhoven et al., 2016).
Adverse family experiences during childhood, confirm the relation between childhood adversity and mental, physical, and behavioral health outcomes (Altintas & Bilici, 2018). Specifically, childhood abuse and maltreatment are consistently associated with increased risk of developing depression, worsening the course of the disease, and negatively affecting response to treatment (Hovens et al., 2012; Nelson et al., 2017; Spinhoven et al., 2016). Adolescents exposed to emotional abuse and domestic violence have four times more chances of developing MDD compared to non-exposed participants (Gallo et al., 2017). A systematic review confirmed that the pooled odds ratio (OR) between any maltreatment and MDD was 2.03; and forecast that a 10-25% reduction in maltreatment could potentially prevent 31.4-80.3 million depression and anxiety cases worldwide (Li et al., 2016).
With respect to cognitive bias, attributional style and the relation to MDD have shown that the interpretation of stressful events as uncontrollable negatively relates to the severity and development of depressive symptoms (Noriega et al., 2014; Sanjuán & Magallanes, 2007). Statistically significant correlations were found between levels of MDD and the negative valence and the unpredictability of the event (Noriega et al., 2014) and structural equation modelling showed that negative attributional style contributes to the development of depressive symptoms (Sanjuán & Magallanes, 2007). In a more recent study, regression analysis showed that the attributional style contributes significantly to the prediction of MDD, even more than only the number of experienced stressful events lived (Gómez Maquet et al., 2020).
Moreover, studies have consistently supported the role of early maladaptive schemas (EMS) in the outcome of psychopathology (Young et al., 2003). A recent systematic re-view examined the relationship between EMS and MDD finding 51 studies that positively correlate EMS with depression, with effect sizes ranging from small to large and accounted for 48% of the variance in the severity of the symptoms for patients with MDD (Bishop et al., 2021). It is relevant to high-light that those 21 studies recruited non-clinical samples (Bishop et al., 2021). The results obtained from this review are consistent with other studies that show that depressive patients exhibit significantly higher scores across the entire spectrum of EMS in comparison to individuals without de-pression (Davoodi et al., 2018; Hawke & Provencher, 2011). Additionally, studies with non-clinically depressed samples have shown that schemas from the domains of impaired autonomy/performance, disconnection/rejection, impaired limits, and other-directedness were associated with the se-verity of depressive symptoms (Calvete et al., 2005; Harris & Curtin, 2002). Also, schema domains of disconnection/ rejection, impaired autonomy/performance, and impaired limits are cross-sectionally related to depression severity (Halvorsen et al., 2009; Renner et al., 2012).
Considering that previous research supports the effect of childhood adversity, EMS, and attributional style in the development of MDD, which emphasizes the importance of exploring the nature of mood disorders from a multidimensional perspective (Insel et al., 2010), and the lack of studies that can measure the effects of these risk factors in co-occurrence and with clinical samples, this study aims to fill the gap by exploring the cumulative effects of child-hood adversity, attributional style, and cognitive schema domains, in relation to the likelihood of developing MDD. The results of this study should evidence how the presence of more than one risk factor in a model that aims to predict the presence or absence of MDD will increase the accuracy, sensitivity, and capacity of prediction and highlight the role of cognitive variables in the development of MDD.
Methods
Design
A retrospective, case-control study was performed to explore the relationship between psychosocial variables (childhood adversity, attributional style, and early maladaptive schemas) and the likelihood of MDD.
Participants
A total of 171 cases were recruited by means of a screening procedure from two psychiatric hospitals in the city of Bogotá, hospitalized for an acute depressive episode ac-cording to the DSM-IV-TR (American Psychiatric Association, 2000), DSM V (American Psychological Association (APA), 2013) or ICD-10 (World Health Organization., 1992). Case inclusion criteria were: 1) Inpatients diagnosed with MDD confirmed by the M.I.N.I. structured interview (Ferrando et al., 2000), 2) Subjects older than 18 years of age, 3) Basic primary school completed or higher. Case exclusion criteria were: 1) Comorbidity with substance abuse or dependence, psychotic disorders, or dementia. 2) Bipolar depression, 3) Delirium. Exclusion diagnoses were ruled out by M.I.N.I. (Ferrando et al., 2000).
The participants of the control group (N = 171) were recruited through an open call in the participant institutions (university and hospitals) and complemented with snowball technique with the administrative staff of the psychiatric institutions considering the following inclusion criteria: 1) Individuals from the community without past or present de-pressive episode, 2) Subjects older than 18 years of age, 3) Basic primary school completed or higher. Control exclusion criteria were: 1) Presence of past or present mental disorder 2) Family relationship with a case subject. Exclusion diagnoses were ruled out by M.I.N.I. as well (Ferrando et al., 2000). The collection of the sample was non-probabilistic for convenience.
Instruments
Personal questionnaire: The personal questionnaire format was designed to evaluate previous family and personal risk factors. It is a self-report questionnaire to be completed with information regarding physical and psychological childhood adversity, and previous history of depression.
M.I.N.I. International Neuropsychiatric Interview (Spanish Version) (Ferrando et al., 2000): The M.I.N.I. is a short structured diagnostic interview designed to explore 17 disorders according to the Diagnostic and Statistical Manual (DSM-IV-TR) criteria (American Psychiatric Association, 2000). For each disorder, one or two screening questions rule out the diagnosis when answered negatively (Lecrubier et al., 1997). Although we recruited depressed in-patients, which guaranteed severe cases with clinical diagnosis, we used M.I.N.I. as a major depression confirmatory instrument. It has been proven that structured interviews are more reliable than semi-structured interviews or clinical diagnosis. The adjusted odds of being classified as having major depression with the M.I.N.I. is approximately twice as high, compared with other structured interviews such as CIDI (Odds Ratio = 2.10; 95% CI = 1.15-3.87) (Levis et al., 2018).
Life Events Questionnaire (Cuestionario de Sucesos Vitales, CSV) (Sandín & Chorot, 2017): The CSV is a self-re-port checklist of 66 items covering a broad range of life experiences. This questionnaire evaluates the occurrence (frequency) of SLEs in the last two years and the intensity (perceived stress) for each event on the scale or each sub-scale corresponding to specific life domains: work, health, love-marriage, family, health, residence, social, legal, and finances. The level of perceived stress is rated for each event on a 0-4-point scale ranging from not at all stressful (0) to highly stressful (4). Additionally, the CSV assesses whether each event is perceived as positive or negative, expected or unexpected, and controllable or uncontrollable. Studies confirm the reliability (Cronbach´s alpha 0.82), normative data, and validity of the CSV (Sandín & Chorot, 2017). In the current sample, Cronbach’s alpha for the total scale was 0.84.
Young Schema Questionnaire-Short Form (Londoño et al., 2010): The YSQ-SF consists of 75 items and assess-es the 15 schemas proposed by Jeffrey Young. It was used to evaluate the presence of early maladaptive schemas in all participants. Each of the scales consists of 5 items and participants are asked to rate them using a six-point Likert scale ranging from 1 (completely untrue of me) to 6 (describes me perfectly). A study aimed to assess the fac-tor structure of the YSQ-SF in a Colombian population con-firmed the existence of the 15 schemas and evidenced good psychometric properties, with a reported Cronbach alpha between 0.73 and 0.88 for the different schemas (Londoño et al., 2010). In the current sample, Cronbach’s alpha for the total scale was 0.94.
Procedure
Consistent with the approval obtained for the research protocol and the informed consent from the ethics commit-tees of the participating institutions and an independent research ethics committee, and adhering to the Declaration of Helsinki, study information was provided to potential participants who met the inclusion criteria. Informed consent was obtained for those participants who expressed interest. The psychologist applied the M.I.N.I. structured interview (Ferrando et al., 2000) to confirm inclusion criteria and rule out exclusion criteria. Eligible participants were administered a battery of questionnaires by one of the trained psychologists of the research team.
Data Analysis
Fisher´s exact tests were used to determine group differences for count variables and T-tests were performed for continuous features. The analysis included age and sex as covariates, since both have been reported as demographic factors associated with depression (Liu et al., 2017; Moreno et al., 2022); specifically, it has been established that the prevalence of the disorder is higher in women as well as in older adults (Kuehner, 2016; WHO, 2017).
A three-stage hierarchical logistic model was fitted to the data to test the research hypothesis regarding the relationship between the likelihood of having depression and reported childhood adversity, attributional style and cognitive schemas. Before the models where fitted preprocessing of the data was conducted, no missing data, outliers or strange values were evidenced. Omnibus tests were conducted to determine the fit of the data in the models. Variance Inflation Factor (VIF) was used to determine the multicollinearity of the data within each model. Finally, a posteriori power analysis with G*Power (Faul et al., 2007) was performed. With the current sample size, to achieve power of 0.80, and alpha of 0.05 the detectable Cohen’s d effect sizes are 0.20, translated to odds ratio equals 1.6 (Champely, 2020; Faul et al., 2007). The statistical analyses were carried out using SPSS Statistics version© 26 (IBM Corp., 2019) and R studio version 1.2.5033 © 2009-201 (R studio Team, 2015).
Results
Demographic and psychosocial variables indicate that of the 171 cases, 114 (66.6%) were female and 57 (33.33%) were male, with a mean age of 34.61 years. Similarly, of the 171 controls, 135 (78.9%) were female and 36 (20.93%) were male, with a mean age of 36.2 years. The female: male ratio in the patient group was approximately 2:1, while in the control group it was 4:1 (Table 1).
Table 1 Demographic and psychosocial characteristics of the study groups
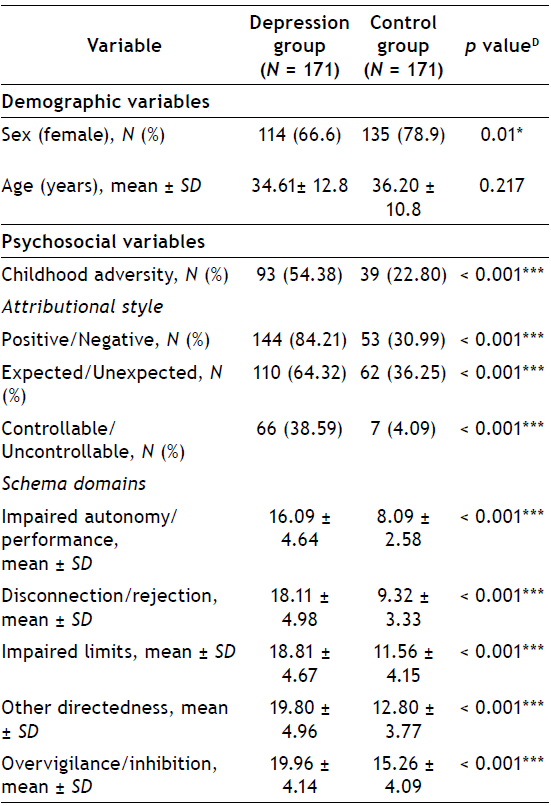
*** p < 0.001; ** p < 0.01; * p < 0.05. D Fisher’s exact test for count data; T test for continuous variables
A three-stage hierarchical logistic model was fitted to the data to test the research hypothesis regarding the relationship between the likelihood of developing depression and reported childhood adversity, attributional style, and cognitive schemas.
The order of the predictor variables entered in the model was determined as it is chronologically plausible that attributional style and cognitive schemas develop throughout childhood and are influenced by the experiences in that specific development stage. Therefore, in step 1, childhood adversity was included. In step 2, the attributional style was added, and in step 3, schemas were incorporated. Age and gender were included in the models as covariate variables. Before the hierarchical logistic regression was performed, all the predictor variables were examined for collinearity.
The Variance Inflation Factor (VIF) evidences that all variables scored less than 5.4 and the tolerance values were more significant than 1.0, which suggests that the models meet the regression assumptions.
The Omnibus test results showed that the three models demonstrate a significant improvement over the intercept-only model (p < 0.00). Regarding the improvement in fit over the previous model, the results show that for model 2, there is a significant fit increase (p < 0.00) compared to the first model, and for model 3, there is also a significant fit improvement (p < 0.00) over the second model, as a result of adding attributional style and schemas.
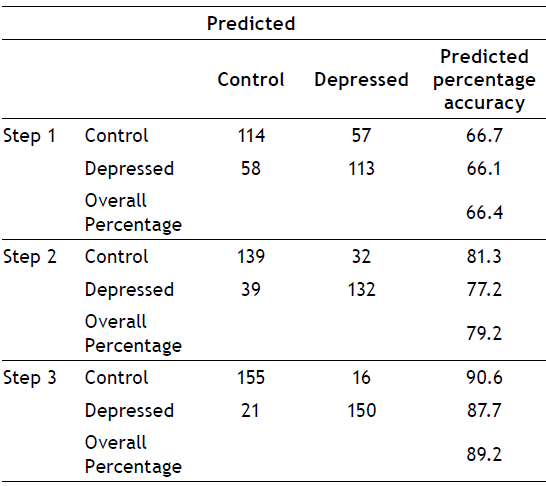
According to the classification table, the accuracy of prediction increases due to the addition of predictor variables to the models, as shown on Table 2. For the first model, there is an accuracy of prediction of 66 %. The final model classifies the data into the corresponding groups of depressed and non-depressed with an accuracy of 89%. Further analysis showed that the prediction is 90% correct when assigning this data to the control group and 87% correct when assigning this data to the depressed specific group for the third model.
According to the Akaike Information Criterion (AIC) score, the third model received the lowest value (AIC = 184.323), indicating that it is the most parsimonious model for the data analyzed (see Table 3). Therefore, an analysis of the specific predictor variables for this model is relevant.
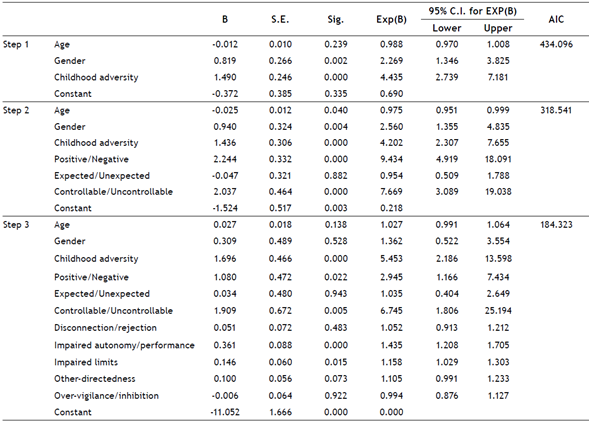
As shown by the Odds ratio reported on Table 3 of the third model, the predictor variables that contribute significantly to the prediction of depression are childhood adversity, an attributional style characterized by interpreting stressful events as negative and uncontrollable, and the cognitive schemas of impaired performance/ autonomy and impaired limits.
The log of the odds of a person who has suffered childhood altreatment is positively related to the development of depression. They have 5.3 (OR = 5.3, CI (95 %) 2.18-13.5) more chances of developing depressive symptoms than an individual who has not. Regarding attributional style, the odds indicate that an individual who judges stressful events as negative and uncontrollable has 2.9 (OR = 2.9, CI (95%) 1.16-7.4) and 6.7 (OR = 6.74, CI (95%) 1.80-25.19) more chances of developing depression, respectively. Finally, cognitive schemas are also significant predictors in the model, and evidence shows that schemas such as impaired autonomy/ performance and impaired limits increase the chances of developing depression by 1.43 (OR= 1.43 CI (95%) 1.20-1.70) and 1.15 (OR = 1.15 CI (95 %) 1.02-1.30), respectively.
Discussion
The present study aimed to explore the cumulative effects of childhood adversity attributional style, and cognitive schema domains, and the likelihood of developing MDD. Most studies examine each risk factor for MMD individually without adjusting for possible confounders. This study examined psychosocial and cognitive risk factors simultaneously. Our findings support what has already been reported in the literature for each risk factor independently related to the association between with MDD and provide a combined model of association of these factors with MDD. The association between each factor with MDD will be discussed and address the implications of the final model as a whole.
Regarding childhood adversity, our results evidenced that patients report significantly higher rates compared to controls. Being a victim of childhood adversity was highly associated with MDD, indicating that the odds of developing depression for those who suffered adversity is much high-er. This leads to the confirmation that adverse events in childhood have a significant influence on MDD, supporting previous evidence (Hovens et al., 2012; Nelson et al., 2017; Spinhoven et al., 2016). This would lead to insist on the importance of improving childhood adversity prevention programs, as underscored in the systematic review by Li et al. (2016).
Concerning attributional style, we found a significant difference between the MDD cases and the healthy controls, indicating that depressive patients perceive a stressful situation as negative, and unexpected. Previous studies in attributional style show contrasting results, one suggests that it is not indicative as a risk factor for the development of depression, instead it is related with the current affective mood (Ball et al., 2008). However, others sustain that the interpretation of uncontrollability given to the event predicts the intensity of depression symptoms com-pared to the event by itself (Noriega et al., 2014; Sanjuán & Magallanes, 2007). In addition, Cámara and Calvete (2012) demonstrated that biased attributional styles explain a significant proportion of the variance of unipolar depression and are a vulnerability factor for MDD, which is consistent with the results found in this study, which emphasize that perceiving a stressful situation as negative and uncontrollable is relevant to differentiate depressive individuals from healthy controls.
Regarding EMS, we found that depressed patients com-pared to healthy controls showed significantly higher means in each domain, which is in line with a meta-analysis that established that all 18 early maladaptive schemas were positively correlated with depression (Bishop et al., 2021). In addition, the study by Chen et al. (2019) found that all five domains correlate significantly with the severity of depression but it also highlighted that impaired autonomy/ performance, disconnection/rejection, and over-vigilance/ inhibition are significantly associated with the persistence of depressive disorder, and the domain of impaired limits was significantly high for major depressive disorder and persistent depressive disorder. Similarly, our study showed that the presence of impaired autonomy/performance and impaired limits domains increased the likelihood of depression significantly. This result was also consistent with the findings of a longitudinal study with clinically depressed and previously depressed patients compared with controls which found that, in addition to impaired autonomy/performance and Impaired limits domains, other directedness explains the variance in depression severity (Halvorsen et al., 2009). It also established that after nine years of follow-up, the do-main of other directedness is a better vulnerability marker of depression severity and impaired Limits is a better mark-er for episodes of Major Depression (Halvorsen et al., 2009). Based on Young’s (Young et al., 2003) theoretical model, it could be inferred that the domain of Disconnection/rejection could be a risk factor for depression, and the domain of impaired autonomy/performance could be a risk factor for anxiety. However, our study shows that the impaired autonomy/performance domain has a significant OR. This result may be explained by the high comorbidity between depression and anxiety, considering that both disorders are categorized as internalization disorders (Eaton et al., 2010). The tripartite model of anxiety and depression establishes that both disorders share negative affectivity and a characteristic that identifies or defines each other (Clark & Wat-son, 1991). The internalization spectrum is characterized by inhibitory symptoms such as sadness, social inhibition, and somatic discomfort (Willner et al., 2016). Therefore, it is expected to find comorbidity between disorders such as depression and generalized anxiety (Eaton et al., 2010), explaining that domains typically found in anxiety are also present in a model for MDD.
Our main contribution is the evidence of the likelihood of depression explained by a multifactorial model of a cumulative effect of childhood adversity, attributional style, and cognitive schema domains with adequate accuracy. The aforementioned means that having experienced adversity in childhood is a risk factor for depression; this risk is in-creased by valuing events as negative and specifically un-controllable, and this by the presence of schema domains of impaired autonomy/performance and impaired limits.
These findings are consistent with the diathesis cognitive stress model of depression.
This data may give important information to identify at risk individuals for MDD. The identification of risk factors for MDD is a contribution for clinicians to accurately delimit the disorder. Major depressive disorder has a broad clinical presentation and severity, and its accurate diagnosis is a challenge in a clinical setting. There is evidence that only about half of the cases with major depression are correctly identified by general practitioners (Mitchell et al., 2009). Additionally, these findings could have potential preventive implications given that early identification of a cognitive susceptibility could lead to the design of prevention interventions based on cognitive models. Finally, it may help to create awareness of the extent of the implications of childhood adversity and encourage the development of positive and flexible family dynamics which according to Young (2003) will result in more adaptive schema domains.
A limitation of this study is that the results from the models are derived from cross-sectional data. Therefore, the results are associations between the variables and should not imply causation. Another limitation includes the use of retrospective questionnaires to inquire about past stressful situations, which may bias the data. Additionally, there was a risk of selection bias, which could have affected the sample of healthy controls, if there is a reason to participate was to seek help. However, this was controlled with the MINI International Neuropsychiatric Interview to rule out a clinical diagnosis of depression. Also, interviewing hospitalized cases could have overestimated the severity of SLEs, as well as the score obtained on other scales, due to the high negative affectivity present in an acute depressive episode. Although many measures were obtained by clinical interviews, some variables were self-reported, which also constitutes a limitation. Finally, each interviewer was not masked/blinded for either case or control group subject, a fact that could account for interviewer severity bias.
In conclusion, our data sustain that childhood adversity, negative and uncontrollable appraisal of SLE and cognitive schemes domains such as impaired autonomy and/or performance, and impaired limits are cumulative risk factors that increase the likelihood of MDD1 2.

