











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Thyroid hormones regulate various processes of metabolism, including the synthesis, mobilization and degradation of lipids 1,2. One cause of cardiovascular disease is the dysfunction of thyroid hormones:it is estimated that between 1.3 and 12% of patients with hypercholesterolemia have hypothyroidism 3,4. Previous studies have reported an increased risk of dyslipidemia in association with atherosclerotic cardiovascular disease. Thus, it has been demonstrated that patients with overt hypothyroidism show consistently elevated levels of cholesterol and triglycerides (TG), while hyperthyroid patients show reduced levels of lipids 1,4. Additionally, some studies have shown alterations of lipids in cases of subclinical hyperthyroidism, suggesting that thyroid hormones and thyroid stimulating hormone (TSH) exert independent effects on lipid metabolism 5-7.
Regarding the mechanisms of action of thyroid hormones and TSH on lipids, advances in molecular biology have shown that these hormones can act by inducing the expression of 3-hydroxy-3-methyl-glutaryl-CoA reductase (HMG-CoA) of the low-density lipoprotein receptor (LDLR), lipase, cholesterol ester transfer protein (CETP) and other enzymes and molecules involved as cardiovascular risk factors 8-12. It has also been reported that TSH induces adipogenesis 13 and lipolysis 14 and increases the activity of HMG-CoA 15.
Given that hypothyroidism and hyperthyroidism are some of the most common conditions in the general population, the relationship between thyroid hormones and the lipid profile in the euthyroid population has generated much interest 4,16 because this information can generate knowledge for the prevention of thyroid disease in this population. Although several studies have revealed that free thyroxine (T4), free triiodothyronine (T3) and TSH are significantly associated with the lipid profile regardless of the patient's sex 17,18, most of those studies measured T4, T3 and TSH together 19,20. Therefore, it is not possible to exclude the effects of the interaction between T3, T4 and TSH in association with the lipid profile. However, increasing evidence indicates that this association is partially related to the direct effect of TSH on the lipid profile and is also associated with metabolic syndrome 21-23.
Finally, although alterations of the lipid profile are commonly observed in patients with thyroid dysfunction, current knowledge on the relationship between lipids and both thyroid hormones and THS is insufficient. Thus, the objective of this study was to determine the relationship between dyslipidemias and thyroid disease in an adult population living in rural areas in the department of Quindío.
Materials and methods
A cross-sectional study was conducted in an adult population living in a rural area comprising eight municipalities in the department of Quindío. A representative sample of the agricultural population was calculated, and a total of 819 participants were included in the analysis. The inclusion criterion was no previous diagnosis of thyroid disease; the exclusion criterion was previous diagnostic or therapeutic tests involving iodinated contrast agents.
Anthropometric and biochemical parameters
Blood samples. Samples were obtained by venipuncture after 12 h of fasting and collected into 2 dry tubes. Serum was obtained by centrifugation at 1000 g for 15 min at 4°C, separated in 1.5 mL microtubes and stored at -20°C until use.
Thyroid tests. TSH and free T4 quantification were performed using a commercial kit (Novatec Immunodiagnóstica GMBH) according to the manufacturer's instructions, and the results were read in an ELISA Stat Fax 303/Plus reader at a wavelength of 450 nm. The reference values that were considered normal were 0.3-4.5 mIU/L for TSH and 8-20 ng/L for free T4. Hypothyroidism was classified into overt hypothyroidism (elevated TSH and low T4) and subclinical hypothyroidism (elevated TSH and normal T4).
Lipid profile. Total cholesterol (TC), high-density lipoprotein (HDL) cholesterol and TG were measured by commercial enzymatic methods (HUMAN®) according to the manufacturer's recommendations. For those with TG below 400 mg/dL, low-density lipoprotein cholesterol (LDL-C) was calculated with the Friedewald equation 24.
Body mass index. This value was calculated as (kg/m2).
Statistical analysis. Data were processed and analyzed in SPSS version 19. A descriptive bivariate analysis was performed; for the chi-squared distribution, significance was assumed to be <0.05. A Kolmogorov-Smirnov test was performed for quantitative variables, and parametric or nonparametric techniques were used according to the results. For normally distributed variables, Student's t-test was applied. The correlations of lipid levels with age, number of cigarettes per day, years of smoking and educational level were determined. A multivariate logistic regression analysis was performed to identify a model with variables related to dyslipidemia.
Results
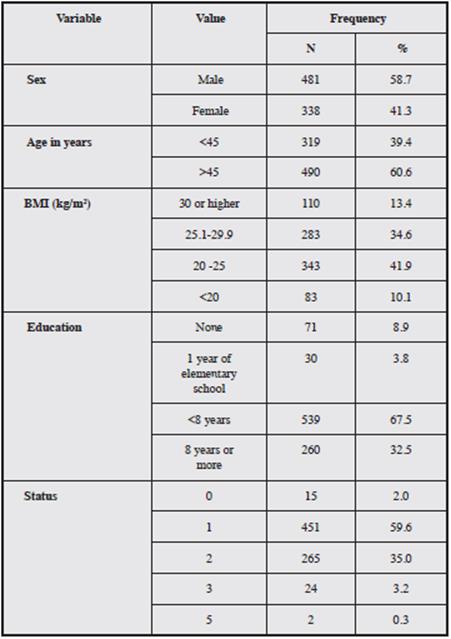
A total of 819 farmers were included; the mean age of the participants was 48.14 years (95% CI: 47.13-49.14), with a minimum of 18 and a maximum of 87. The majority were male (58.7%). The average number of years of education was 5.94 (95% CI: 5.66-6.22); of the total, 67.5% had studied less than 8 years, and 21.6% were illiterate or had completed only elementary school (Table 1).
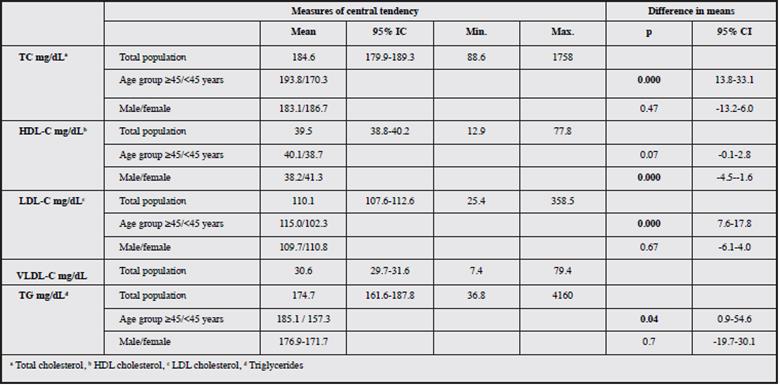
In terms of medical history, only four people reported suffering from "elevated cholesterol or triglycerides"; regarding medication history, six people were being treated for dyslipidemia. In the total population, averages were within normal limits for TC (184.6 mg/dL) and LDL-C (110.1 mg/ dL), low for HDL cholesterol (39.5 mg/dL) and elevated for TG (174.7 mg/dL). The average TC and LDL-C levels were significantly higher in people over 45 years of age (p=0.000), while HDL-C was higher in men (p=0.000) (Table 2).
No correlation was found between lipid levels and age, number of cigarettes per day, years of smoking or educational level.
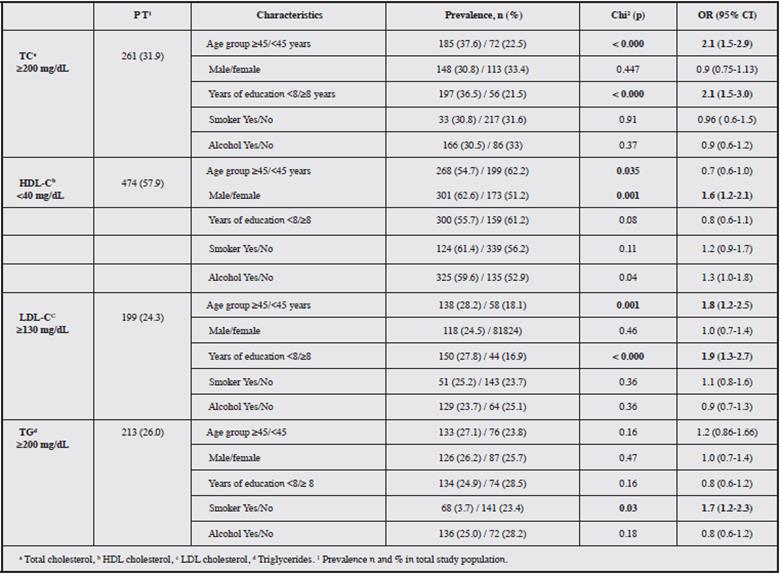
In the total population, the prevalence of alterations in the lipid profile was as follows: elevated TC, 31.9%; HDL-C lower than 40 mg/dL, 57.9%; increased LDL-C in 24.3% (n=199), including levels between 130 and 159 mg/dL in 17.3% (n=141), between 160 and 189 mg/dL in 7.2% (n=59) and above 190 mg/dL in 1.7% (n=14); TG 200 mg/dL or higher, 26% (n=213), including levels between 200 and 499 mg/dL in 24.3% and levels of 500 mg/dL or higher in 1.7%.
In the bivariate analysis of the relationship between altered lipid levels and the included risk variables, a noncausal association was found between age 45 years and older and TC greater than or equal to 200 (OR=2.1, p=0.000), HDL-C less than 40 (OR=1.6, p=0.001) and LDL-C greater than or equal to 130 (OR=1.8, p=0.001). An education level of less than eight years was associated with elevated TC and LDL-C (OR=2.1, p=0.000 and OR=1.9, p=0.000, respectively). TG was significantly elevated among those who consumed alcohol (OR=1.7, p=0.04) (Table 3).
A TSH level of 4.6 mIU/L or greater was found in 8.1% of the study population. The prevalence of overt hypothyroidism (elevated TSH and low T4) was 1.2%, and that of subclinical hypothyroidism (elevated TSH and normal T4) was 6.7%.
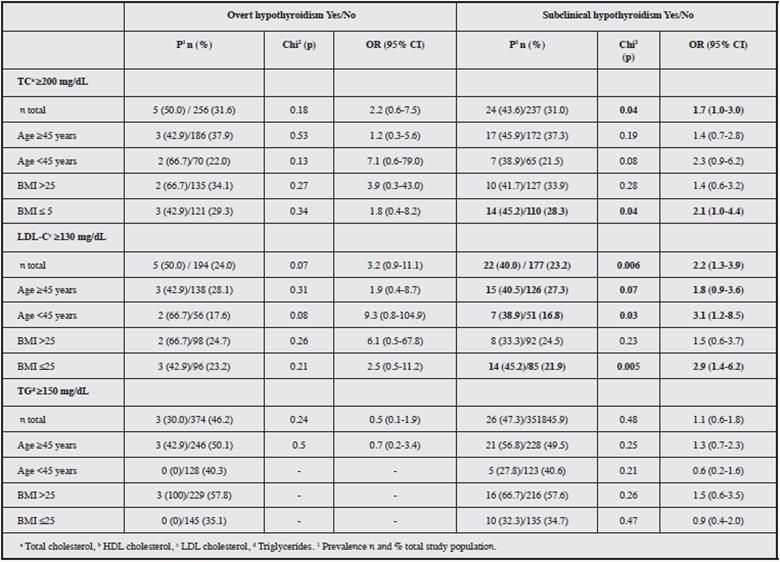
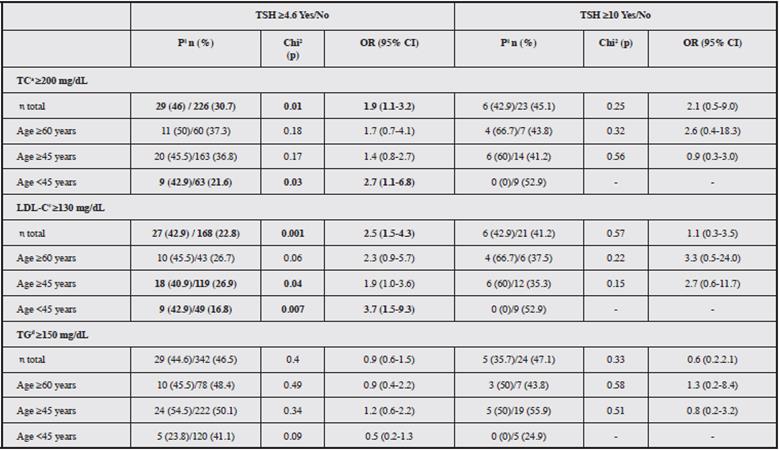
Patients with overt hypothyroidism had a higher prevalence of elevated TC than those without overt hypothyroidism (50.0% vs. 31.6%). This difference was more pronounced in patients younger than 45 years (66.7% vs. 22.0%), and the prevalence of LDL-C greater than 130 mg/ dL was much higher in this age group (66.7% vs. 17.6%); however, these differences were not significant.
In those with subclinical hypothyroidism, significant differences were observed for both elevated TC (43.6% vs. 31.0%, p=0.04) and elevated LDL-C (40.0% vs. 23.2%, p=0.006); the difference in LDL-C was significant for patients younger than 45 years. Likewise, significant differences in the prevalences of TC and elevated LDL-C were observed in those with a BMI below 25 (Table 4).
A significant relationship was found between TSH 4.6 mIU/L or higher and elevated TC (OR=1.9, p=0.01) and elevated LDL-C (OR=2.5, p=0.001) for the entire study population. Additionally, elevated LDL-C was 2.2 times more prevalent in people with subclinical hypothyroidism compared to those with normal levels of thyroid hormones (Table 5).
In the multivariate analysis, the following factors were associated with hypercholesterolemia: age younger than 45 years (OR 1.8 95% CI=1.2-2.5) and education less than eight years (OR=1.7, 95% CI=1.2-2.4); regarding elevated LDL-C, age less than 45 years (OR=1.4, 95% CI=1.0-2.1) and education (OR=1.6, 95% CI=1.1-2.5) remained in the final model, but the most important factor was TSH greater than or equal to 4.6 (OR=2.2, 95% CI=1.3-3.7) in one model and subclinical hypothyroidism (OR=2.0, 95% CI=1.2-3.6) in the other. Hypertriglyceridemia was associated with age younger than 45 years (OR=1.4, 95% CI=1.1-1.9) and BMI above 25 (OR=2.6, 95% CI=1.9-3.4).
Age younger than 45 years stood out as an independent factor associated with hypercholesterolemia, elevated LDL-C and hypertriglyceridemia; this age group had a risk approximately 1.5 times higher than that of older participants. In this study, dietary habits were not assessed, but it is possible that the people in the older age group had a healthier diet. In the multivariate model, alcohol consumption was also included, but no associations with hypothyroidism were found.
Similarly, an education level less than seven years was associated with both TC and elevated LDL-C. A BMI above 25 was only associated with hypertriglyceridemia.
The alteration of thyroid hormones, both the isolated elevation of TSH to above 4.6 mIU/L and the presence of subclinical hypothyroidism, the most important factor for the elevation of LDL-C in the multivariate models; com-pared with people with normal hormone levels, those with thyroid hormone alterations had a two-times-greater risk of elevated LDL-C.
Discussion
The leading cause of mortality worldwide is cardiovascular diseases, many of which are conditioned by persistent elevated lipid levels in the blood; the literature reports that more than 30% of the world's population suffers from dyslipidemia (25), and a very important cause of dyslipidemia is thyroid hormone dysfunction 3,4.
In this study, the relationship between dyslipidemia and thyroid hormones in agricultural workers was explored. Although it has been suggested that farmers tend to have fewer alterations in plasma lipids due to their physical activity levels, several studies have shown that there are no such differences between farmers and nonfarmers 25,26. In our study, 31.9% of the participants had elevated TC; 57.9% had HDL-C less than 40 mg/dL, 24.3% had elevated LDL-C and 26% had hypertriglyceridemia. Only 1% of the participants received drugs for the treatment of dyslipidemia; this proportion of dyslipidemias is very similar to those described for other populations in the region 27.
The prevalence of lipid abnormalities was significantly higher in farmers aged 45 years and older (TC, OR=2.1; HDL-C less than 40, OR=1.6; LDL-C greater than 130, OR=1.8). An education level less than eight years was also associated with elevated TC and elevated LDL-C (OR=2.1 and 1.9, respectively). These changes in lipid levels according to age and sex have also been reported by different authors 27-29. Landázuri et al. showed that in a group of patients and their first-degree blood relatives, the group of relatives under 18 years of age had lower TC and LDL cholesterol levels than the group of relatives older than 18 years 27. Goh et al. found sex differences in all lipids and lipoproteins; men had significantly higher levels of TC, TG and LDL-C and lower levels of HDL-C than women 28. Goh also found that although the levels of lipids and lipo-proteins in men did not differ among different age groups, women over 50 years of age showed significantly elevated levels of lipids and lipoproteins, especially TC, LDL-C and TC/HDL-C, compared with the corresponding levels in women aged between 30 and 46 years 28.
Regarding thyroid function, in the present study, 8.0% of participants had elevated TSH levels, 6.7% had subclinical hypothyroidism, and 1.2% had overt hypothyroidism. These figures are lower than those described by Londoño et al. 30 and Builes et al. (18.5% and 36.8%, respectively) 31; these studies were performed in the general populations of Quindío and Bogota, respectively. This discrepancy could be attributed to the fact that the present study used different selection criteria and included a study population that was more homogeneous than the general population. Similarly, Fardella et al. 32 examined a group of workers from different Chilean companies and found that 6.8% had abnormal serum levels of thyroid hormones and TSH, 1% had hypothyroidism, 5.6% had subclinical hypothyroidism, and 0.2% had hyperthyroidism, figures very similar to those described in the present study.
In terms of the relationship between lipid alteration and thyroid function, it was observed that 11.4% of the patients with hypercholesterolemia had elevated TSH (p=0.017) (overt), and 9.2% had subclinical hypothyroidism (p=0.039). Other studies have demonstrated an association between hypercholesterolemia and thyroid dysfunction and have reported that individuals with this type of dyslipidemia have a prevalence of thyroid changes that varies between 1.4 and 13% 3-5.
This relationship may be based on the effect of thyroid hormones on lipid metabolism; thus, T3 is required for the metabolism of cholesterol and LDL-C because this hormone controls the expression of the gene encoding the receptor 1,33. Consequently, the persistent and progressive decrease in circulating levels of thyroid hormone greatly increases the concentrations of cholesterol and TG 1. Tan KC et al. 34 demonstrated that HDL subfractions are also affected by thyroid dysfunction; while the HDL2 subfraction was reduced in patients with hyperthyroidism, it was increased in patients with hypothyroidism. The treatment of both types of patients reversed these findings. It is believed that changes in HDL subfractions are mediated by the effect of thyroid hormone on hepatic lipase 34.
It was noteworthy that significantly higher values of TC and LDL-C were found in participants with subclinical hypothyroidism and that these differences were more marked among those younger than 45 years of age; this behavior was not as evident in cases of overt hypothyroidism. The differences in TC and LDL-C were very evident and significant in patients with TSH above 4.6 mIU/L but were not when TSH values were 10 or higher, possibly because in the latter case, the number of patients was very low. Subclinical hypothyroidism is characterized by elevated serum levels of TSH and normal levels of free T3 and T4; it is common in the general population, especially in older women 35. Several authors have suggested an association between subclinical hypothyroidism and cardiovascular disease 23,35; this association is still controversial, although some data suggest that patients with THS>10 mU/L may have an increased cardiovascular risk 35. The study by Nair et al. in the Hindu population found no association between subclinical hypothyroidism or increased TSH and 10-year cardiovascular risk using the Framingham scale 36. The same study did not observe differences between the groups with respect to the lipid profile, but it did find that an increased TSH was significantly correlated with moderate worsening of the lipid profile 36, suggesting that TSH exerts an independent isolated effect on the metabolism of lipids 23. Although several studies have demonstrated a strong association between TSH and TG 6,21, the association between TSH and cholesterol is still controversial 37,38. However, our study found a causal association between elevated TSH and hypercholesterolemia (OR 1.9) and elevated LDL-C (OR 2.5), and the latter is 1.2 times more common in people with subclinical hypothyroidism.
The alteration of thyroid hormones, both the isolated elevation of TSH to levels of 4.6 mIU/L or higher and the presence of subclinical hypothyroidism, was the most important risk factor for elevated LDL-C in the multivariate models; individuals with thyroid hormone alternations had twice the risk of elevated LDL-C compared with individuals with normal hormone levels.
The literature reports that patients with TSH values between 5.1 and 10 mIU/L have significantly higher total average cholesterol and LDL-C levels compared to euthyroid subjects 39. The mechanisms by which this occurs are under investigation, but there is a consensus that dyslipidemia is mainly caused by an imbalance characterized by an increase in cholesterol synthesis compared with the rate of degradation; this leads to the inhibition of the LDL receptor and consequently to an increase of this lipoprotein in plasma, which provides the substrate for peroxidation of lipids by reactive oxygen species (ROS), which further results in oxidative stress and can lead to cardiovascular disease 39,40.
The association of LDL-C with abnormal TSH levels confirms the need for surveillance and control not only of overt hypothyroidism but also of subclinical hypothyroidism. Various related specialist associations recommend screening for hypothyroidism in patients with dyslipidemia before initiating treatment 3 to contribute to the reduction of morbidity and mortality from cardiovascular events.
Given agricultural workers' very particular socioeconomic conditions, it is important to design screening programs for biomarkers that allow the early detection of changes in thyroid hormones, TSH and lipid profiles so that relevant medical measures can be implemented.


