











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Reversible vasoconstriction syndrome (RVS) is made up of a group of disorders which are characterized by intense, sudden-onset ("thunderclap") headaches, with or without focal neurological deficits and reversible multifocal vasoconstriction of the cerebral arteries, which resolve within 12 weeks 1. Several predisposing factors have been described which previously conditioned different nomenclatures, until all of them were unified under the concept of RVS 2, originally 'reversible cerebral vasoconstriction syndrome' (RCVS).
There is a female predominance in the reported cases, especially in middle-aged patients, with a peak incidence between 20-50 years 3; there are also reports in children 4.
The syndrome is likely caused by altered regulation of the cerebral vascular tone which triggers multifocal arterial constriction and vasodilation 1,3. In 60-80% of cases a trigger can be identified, and there is usually a prior history of headaches, including migraines in up to 40% of patients 1. It is generally self-limited and has a low recurrence rate 1,5.
The patient in this case had a history of migraines and frequent use of a vasoconstrictive substance like isometeptene for headache relief. It is likely that this substance was the trigger.
Case presentation
A 57-year-old woman was admitted to the emergency room due to an intense headache which had lasted for three hours with persistent nausea and vomiting. The temporo-occipital headache had a sudden onset and was not relieved by taking a compound which she frequently used containing dipyrone, isometeptene and caffeine, nor with acetaminophen or intramuscular diclofenac. She had repeated episodes of vomiting and a generalized tonic-clonic seizure which resolved spontaneously. She was in pain, without focal neurological deficits, but with elevated arterial blood pressure (165/105), tachycardia (112 per minute), tachypnea (28 per minute) and afebrile (36.8°C) with evident agitation, confusion and disorientation. Her ocular fundus exam was normal as well as the rest of her physical exam.
She had a history of arterial hypertension, dyslipidemia, obesity, sedentarism and episodes of bitemporal headaches which had become more frequent and intense in the previous two weeks. The headache was attributed to a migraine episode. Among her usual medications, in addition to what has already been mentioned, were losartan, hydrochlorothiazide, atorvastatin and aspirin. A simple brain CT was performed due to a suspected intracranial bleed, which was normal (Figure 1A). The lumbar puncture yielded clear cerebrospinal fluid with a pressure of 28 mmHg, 58 mg/dL of glucose, 62 mg/dL of proteins, and 3 lymphocytes/ mm3. There were no red blood cells or xanthochromia.
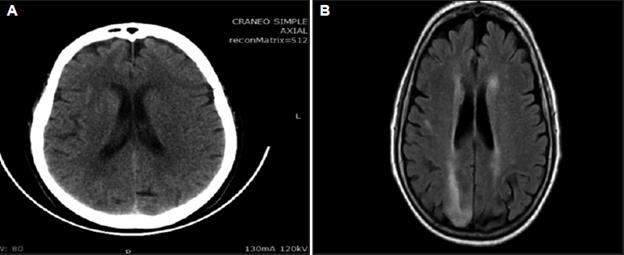
Figure 1 A. Simple brain CT without structural abnormalities. B. Simple brain NMR. FLAIR. Right periventricular and occipital hyperintense zones.
With a normal CT, a simple brain NMR was ordered which showed periventricular and occipital cortical-sub-cortical hyperintense zones along with another small, right parietal one without collections of blood. FLAIR Sequence (Figure 1B).
Due to this finding, cerebral angiography was performed showing areas of multifocal cerebral arterial vasoconstriction, mainly in M2 of the right middle cerebral artery and in segments V3 and V4 of the vertebral artery on the same side (Figure 2).
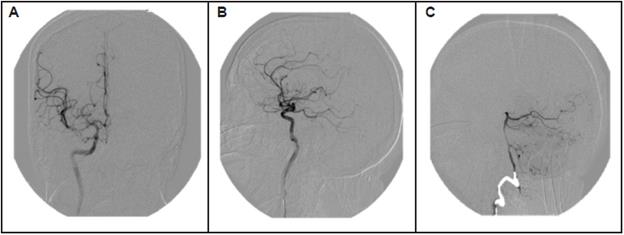
Figure 2 Cerebral angiography. A, B and C. Areas of multifocal arterial vasoconstriction, mainly on M2, of the right middle cerebral artery.
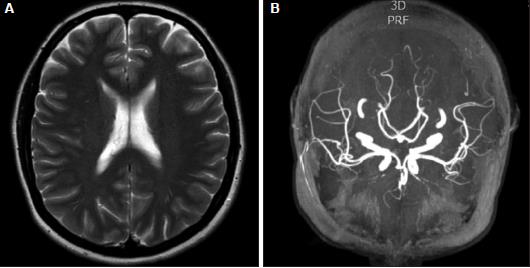
Twelve weeks later, the patient was still asymptomatic. Since she refused a follow-up angiography, angioresonance was performed which did not show the hyperintense zones or the vasoconstriction initially described (Figure 3).
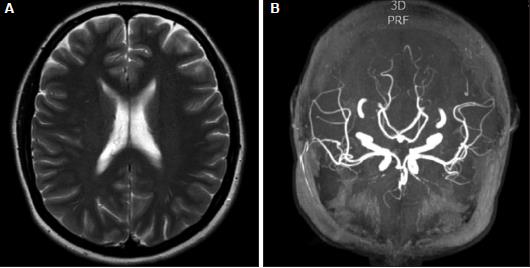
Figure 3 Cerebral angioresonance. A and B. Disappearance of the hyperintense zones and vasoconstriction.
Further tests were performed, including blood tests for HIV, syphilis, herpes simplex virus type 1 and 2, cytomegalovirus, HBsAg and Epstein-Barr virus, all of which were negative. Moreover, the CBC, blood glucose level, creatinine, C-reactive protein, urinalysis, kidney function test, liver profile, electrolytes, PT, PTT and arterial gases were within normal limits. Tests for antibodies such as ANAs, anti-DNA, anti-Ro, anti-La, anti-RNP, anti-SM, IgG and IgM cardiolipins, p-ANCAs and c-ANCAs were negative. Her chest x-ray and electrocardiogram were normal. Hypercoagulability studies and an EEG were not performed.
The seizures did not recur during hospitalization, and the headache gradually decreased, disappearing completely on the seventh day. In addition to the inpatient symptomatic treatment given, nimodipine 60 mg every four hours, by mouth, was used. She continues to take this medication at a lower dose, even though she was instructed to discontinue it.
Discussion
As knowledge has advanced, RVS has been increasingly recognized in the last few years, but continues to be an unsuspected condition, and therefore undiagnosed in many emergency rooms and hospital wards 3. Moreover, most physicians, including some neurologists, have a limited knowledge of RVS.
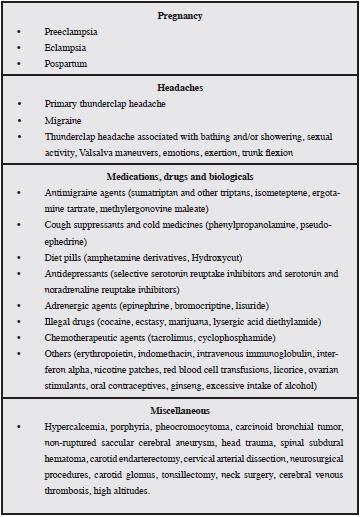
It is a syndrome which was probably misinterpreted in past decades because it was attributed on the one hand to a primary vasculitis of the central nervous system, and on the other, to an aneurysmal subarachnoid hemorrhage, due to the overlapping clinical manifestations in addition to the cerebral angiographic narrowing 6. This narrowing has also been described in other disorders, leading to different eponyms such as acute benign cerebral angiopathy, Call-Fleming syndrome, drug-induced angiopathy, migraine vasculitis, postpartum angiopathy, primary sexual headache, bath-related headache and others 1. "Thunderclap" headaches have various causes, including RVS 1,3,5. See the differential diagnosis in Table 1 7.
Our case has similar characteristics to those described in the literature as "thunderclap" headaches, which are sudden and severe headaches which reach their maximum intensity in one minute or less 7. It is one of the most frequent and characteristic symptoms of the syndrome, presenting in 94 to 100% of patients 3,8,9. Our patient had a history of migraines, which is seen in up to 40% of cases 1,9; she had a seizure, which has been reported in 1 to 17% of patients 9,10; she had no residual focal neurological deficits, although in other case series this has been documented in 8 to 43% of patients 9; and she had a history of arterial hypertension, a condition which has been considered to be comorbid. Often, when RVS presents, blood pressure readings are high 10, as in this case. However, it is unclear if these high blood pressure readings are part of the events leading to an episode of RVS, or if this is a physiological response 1,10.
Most of the reported cases are in women, but the reason for this prevalence is unknown 3.
The patient habitually took an isometeptene-based compound to relieve the pain of migraine episodes, and both migraines as well as isometeptene are considered to be conditions which may trigger RVS 1,3,9,10. We believe that the frequent use of this substance was the trigger in a patient with the premorbid base of migraines.
Table 2 shows the associated conditions and precipitating factors of RVS.
Table 2 Triggers and conditions associated with reversible cerebral vasoconstriction syndrome. (Reference 8).
Despite the gradual knowledge of RVS which has been obtained, the exact pathophysiology is still unknown 1,9. Since RVS is a group of similar clinical-radiological syndromes, it is probable that the underlying mechanisms are multifactorial 1. Proposed mechanisms include vascular tone regulation disorders caused by endothelial dysfunction, where sympathetic hyperactivity would play an important role, interacting with a genetic predisposition and precipitating or associated factors 1,3.
The diagnosis of RVS requires, besides the characteristic "thunderclap" headache, proven segmental vasoconstriction of the cerebral arteries and its complete or almost complete reversibility within 12 weeks of the onset of the symptoms 3. Here, the role of neuroimaging is essential, not only to prove the vasoconstriction, but also for alternative diagnoses and potential complications such as intracranial hemorrhage, vasogenic edema and ischemic stroke 3,10. Although conventional angiography has been the criterion standard for assessing cerebral vasoconstriction, non-invasive imaging modalities such as transcranial Doppler, tomography angiography (CT angiography) and magnetic resonance angiography (angioresonance) are being used more frequently 11.
We did not obtain a follow-up angiography on the patient in this case. The angioresonance performed is valid; it helped us in the diagnosis and does not detract from the validity of the case.
The differential diagnosis should include, mainly, aneurysmal subarachnoid hemorrhage, which the patient did not have, and primary central nervous system vasculitis, a less common entity predominantly presenting in males, whose headache is insidious and progressive, and whose angiographic findings are generally irreversible 10. In the described case, an association between the RVS and posterior reversible encephalopathy syndrome is probable, since they share many clinical and radiological characteristics, suggesting an overlap or similar pathophysiological mechanisms 1.
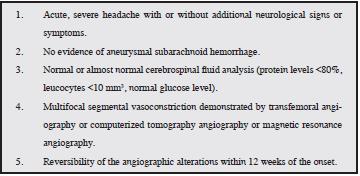
In 2007, Calabrese 2 proposed some diagnostic criteria that have proven useful for diagnosing RVS and improving medical knowledge but have not been validated in prospective studies 10. The patient in this case fulfills the described criteria (Table 3), as well as the headache attributed to RVS according to the Headache Classification Committee of the International Headache Society in its third edition 12.
Given the potentially serious nature of the possible underlying intracranial etiologies, "thunderclap" headaches should be considered and treated as a medical emergency. Therefore, we propose that all patients with a "thunderclap" headache, in addition to having a good clinical history and physical exam, should have a head CT without contrast as soon as possible to rule out subarachnoid hemorrhage. If the CT is normal, the next step is to perform a lumbar puncture to determine the opening pressure and analyze the cerebrospinal fluid. If the CT and lumbar puncture are not diagnostic, a simple brain MR should be carried out along with noninvasive neurovascular imaging through angioresonance or CT angiography. Conventional arteriography is reserved for cases in which there is doubt regarding vasoconstriction in the prior studies.
There is no established treatment for RVS 3. Verapamil, glucocorticoids, magnesium sulphate, triptanes, and dantrolene have been used, as well as balloon angioplasty and intra-arterial administration of nicardipine, papaverine, milrinone and nimodipine, with varying results 9. Glucocorticoids should not be used, as they have been associated with worse results 9. They are useful when the apparent RVS is caused by primary vasculitis of the CNS 6,9.
Given the lack of comparative clinical studies, the treatment of vasoconstriction has been directed by observational data and expert opinion 3.
We used nimodipine empirically to treat the vasoconstriction. However, there are data that show that nimodipine does not affect the evolution of cerebral vasoconstriction 3,10, but could alleviate the intensity of the headache, and an effect on the small vessel walls, not visible on conventional angiography, has been documented. Thus, imaging techniques must be improved, especially vessel wall imaging 11. Nonetheless, since clinical and angiographic resolution occur without any medical intervention in approximately 90% of patients 9, we propose to only provide symptomatic pain management, bed rest, elimination of the triggers and avoidance of the Valsalva maneuver as adequate measures while awaiting the natural resolution of the headache and the vasoconstriction. Likewise, we believe that these patients should not necessarily go to the ICU, unless they are unstable and/or have a worsening neurological state.
In conclusion, despite the strong growing interest in RVS, complete understanding has still not been reached. Since it is a clinical entity characterized by a sudden "thunderclap", intense headache, it must be considered within the differential diagnosis in emergency rooms when patients with this type of headache present, in order to guide the necessary tests; especially in patients with a history of headaches, migraines and medication or drug abuse, which are common in our environment.


