











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Hypoglycemia in nondiabetic patients is defined as a blood glucose level lower than 55 mg/dL 1. It is con sidered to be a medical emergency, and has a variety of symptoms which basically depend on its severity, generally being classified as neuroglycopenic symptoms (changes in behavior, drowsiness, confusion, seizures and coma), autonomic adrenergic symptoms (trembling, palpitations, anxiety), and autonomic cholinergic symptoms (hunger, diaphoresis, paresthesias) 2. The described causes of hy poglycemia in nondiabetic patients include those classified as pharmacological, such as those caused by sulfonylureas, cibenzoline, antibiotics like pentamidine, quinine and al cohol. Other causes include a deficit of hormones such as glucagon, cortisol and epinephrine; lack of glucose due to starvation or malnutrition; critical patients with liver, heart or kidney failure; and endogenous hyperinsulinism due to nesidioblastosis, following gastric bypass surgery, or due to functional pancreatic neuroendocrine tumors like insu linomas. Likewise, non-hyperinsulinemic hypoglycemia is caused by nonpancreatic neoplasms such as fibrosarcoma, liposarcoma, rhabdomyosarcoma, leukemia, lymphoma, teratoma, fibrous tumors (solitary or multiple) and mesothelioma 3,4.
A solitary fibrous tumor of the pleura is a rare neoplasm. This tumor is mostly benign, representing 8% of the benign chest tumors and 10% of the pleural tumors. It is located, in 30% of cases, in the visceral or parietal pleura, and extra thoracically, predominantly in the peritoneum, pericardium and mediastinum 5,6. This tumor has other names such as localized mesothelioma, benign fibrous mesothelioma or benign localized fibroma 5. Since most of them are benign and slow-growing, they may be asymptomatic and undetected for an extended period of time. However, 10% of these fibrous tumors may be malignant with local or metastatic recurrence, with malignancy variables including high cellularity, mitotic activity of four or more mitoses/10 high-power fields, and necrosis 7-9. In 2013, a risk factor scoring system was described to predict aggressive behavior with a significant degree of recurrence if at least three of the following six criteria are present: located in the parietal pleura, size equal to or greater than 10 cm, hypercellularity, nuclear atypia, four or more mitoses/10 high-power fields and necrosis 10,11.
In patients with a solitary fibrous tumor of the pleura, hypoglycemia occurs in fewer than 5% 5. Refractory hypoglycemia has been related more frequently to tumors originating in the peritoneum or those which reach a "giant" size in the pleura (greater than 10 cm) 6. Hypoglycemia associated with a solitary tumor of the pleura is a paraneoplastic syndrome referred to in the literature as Doege Potter syndrome.
Doege Potter syndrome was described in 1930 as a syndrome characterized by severe, sustained and refrac tory hypoglycemia associated with nonpancreatic tumors, more specifically, to fibrous tumors originating most frequently in the pleura 12. In general, it is a syndrome with a nonspecific clinical presentation, with symptoms related to lung involvement: cough, dyspnea, chest pain and pleural effusion 6. At a metabolic level, it presents with hypoglycemia, this being the main diagnostic criterion 12, and which, in its pathophysiological mechanism is characterized by low insulin levels, undetectable C-peptide, and normal IGF-I levels 12. Treatment is based mainly on curative tumor resection, with consequent improvement in symptoms.
We present the case of a patient with initial respiratory signs and symptoms, a documented pleural mass with a histological diagnosis by biopsy of a solitary fibrous tumor of the pleura, and the subsequent appearance of symptoms associated with severe hypoglycemia with Whipple's triad: symptoms or signs of hypoglycemia, low blood sugar and symptom resolution after its correction 1. She also underwent a 72-hour fasting test which was positive for non-hyperinsulinemic hypoglycemia a few hours after its initiation, and was thus diagnosed with Doege Potter syndrome.
Case report
This is a case of a 67-year-old woman who consulted due to a four to six-week history of episodes of altered consciousness with hallucinations, disorientation, abnormal behavior, and disconnection from her environment, with subsequent recovery and amnesia regarding the event. Six months prior to this episode, the patient had consulted due to a cough with bloody sputum, for which a chest computerized tomography (CT) with contrast had been performed, finding a 17 x 12 x 9 cm pleural mass suggestive of a fibrous tumor. A pleural trucut biopsy was performed, reporting a fibrous tumor with diffuse immunoreactivity of the tumor cells to vimentin, CD99, BCL2 and CD34, and a 5% Ki67 cell proliferative index. The P53, NSE, S100, AML and desmin markers were negative. Two months after this biopsy, a follow-up trucut biopsy was performed which confirmed a fibrous tumor of the pleura as a fusocellular tumor without atypia, necrosis or mitotic activity, which was considered to be benign. The patient began the procedures to be seen and treated by thoracic surgery.
Due to her symptoms on admission, a cerebrovascular accident or neurogenic/cardiogenic syncope was ruled out with a brain CT, Doppler test of the neck vessels, electro encephalogram and brain magnetic resonance, with no rel evant findings. She also had a transthoracic echocardiogram showing a preserved LVEF. Given the clinical picture with an unknown etiology, she was seen by psychiatry and neuropsychology, ruling out a psychosomatic disorder.
Due to the desaturations during the described episodes, another chest x-ray was taken, reporting left basal opacity with a well-defined upper border (Figure 1). A new chest CT with contrast was also performed, reporting an image compatible with a fibrous tumor of the left pleura, which had increased significantly in size compared to the previous test (April 2018), and a residual calcified granuloma in the right upper lobe (Figure 2).
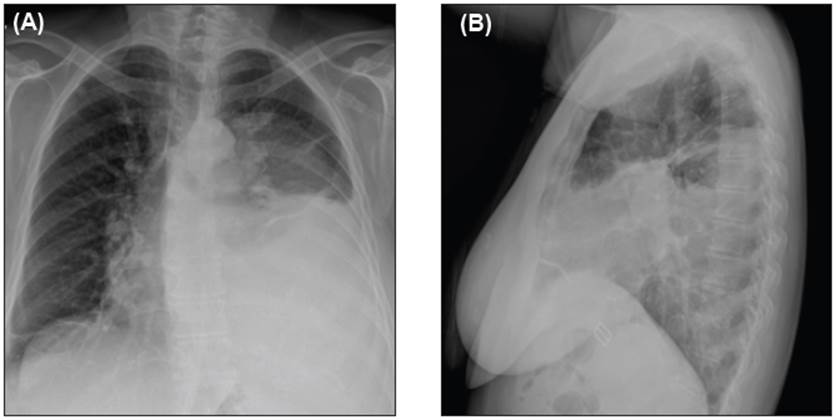
Figure 1 Chest x-ray: a mass occupying the base of the left lung. A: anterior-posterior. B: lateral.
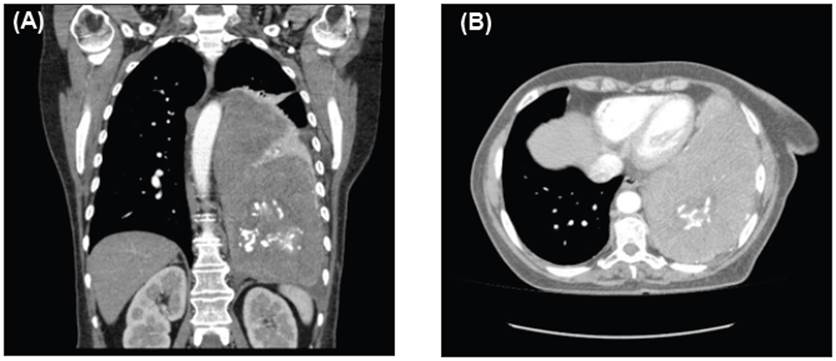
Figure 2 Tomography of the chest with contrast: Extrapulmonary solid mass with internal calcifications. A: coronal view. B: cross-sectional view in the lung window.
During the preparation for the imaging study, and after approximately six hours of fasting, she experienced an altered state of consciousness and diaphoresis; therefore, a blood sugar test was performed with a reported level of 41 mg/dL. Twenty grams of dextrose were administered, and the follow-up blood sugar was 62 mg/dL. During the following 24 hours, she had symptomatic refractory hypoglycemia despite dextrose boluses, and thus she was placed on a continuous infusion, with improvement in her state of consciousness as well as her blood sugar levels. Due to the refractory hypoglycemia of unclear etiology, other en docrine disorders were ruled out, such as diabetes mellitus (glycosylated hemoglobin at 5.2%), thyroid disease (TSH 1.8 IU/L) and adrenal insufficiency (basal cortisol at 8 AM of 221 nnmol/L).
The patient had a history of a fibrous tumor of the pleura (histopathological diagnosis) associated with severe symptomatic hypoglycemia with Whipple's triad, which was difficult to manage; thus, a presumptive diagnosis of paraneoplastic syndrome was made. She underwent a 72 hour fast, with confirmed hypoglycemia within the first few hours of the test, a reported C-peptide level less than 33.1 pmol/L and a reported insulin level less than 4.2 pmol/L. Thus, this was a patient with a fibrous tumor of the pleura and severe, symptomatic non-hyperinsulinemic hypoglycemia, with Doege Potter syndrome being the most likely diagnosis. Complementary treatment was provided with 15 mg of prednisolone every 12 hours, which temporar ily resolved the hypoglycemias while she was evaluated by thoracic surgery and taken to surgery for resection of the fibrous tumor of the pleura. Intraoperative findings showed a 15 x 10 x 10 cm diameter solid tumor touching the diaphragm at the left lower lobe.
Postoperatively, the patient showed clinical improvement with no new hypoglycemic episodes or altered states of consciousness, and no need for additional glucose after discontinuing the prednisolone. The pathology report showed a 17 x 15 x 9 cm fibrous tumor of the pleura, with tumor-free resection margins. On outpatient follow up in the subsequent months, the patient remained asymptomatic with no new episodes of hypoglycemia.
Discussion
Doege Potter syndrome is mainly caused by hypoglycemia-inducing intrathoracic tumors 12, generally by a solitary fibrous tumor, although some cases report multiple tumors 12. It has been described as a rare paraneoplastic syndrome 13 with an incidence of 2.8 per 100,000 popula tion 11, and a mean age at diagnosis between the sixth and eighth decade of life 13.
The tumors may grow very large before they are symp tomatic. When symptoms are present, they include intra thoracic symptoms such as cough, dyspnea, and pleural effusion; or extrathoracic symptoms such as hypertrophic osteoarthropathy or severe, sustained hypoglycemia 13. In our case, the patient was within the usual age group for presentation and had a solitary fibrous tumor of the pleura. The clinical picture produced by severe, symptomatic hypoglycemia secondary to greater glucose consumption by the tumor 5,6 and/or insulin-like growth factor II (IGF-II) secretion causing lowered insulin levels and somatomedin-C (IGF-I) displacement from its carrier protein 6 is taken as a diagnostic criterion. In the presented case, non-hyperin sulinemic hypoglycemia was documented during the fasting test, within the context of severe, persistent hypoglycemia. However, no serum IGF-II measurement was performed since it is not available in our setting.
Considering that the syndrome's main symptom is hypoglycemia, which causes most of these patients' compli cations, the "curative" treatment is surgical removal of the tumor 13. Symptom management mostly consists of intra venous dextrose boluses or infusion, according to the clinical response. However, there are complementary treatments in the literature using glucagon, somatostatin analogues, recombinant growth hormone and, of course, glucocorticoids. Glucocorticoids were what allowed us to control the hypoglycemia, as a bridge therapy, until the tumor could be surgically removed. Glucocorticoids and growth hormone, combined or as monotherapy, are the most frequently used agents for symptom management, and are even an alternative when the tumor is inoperable. Glucocorticoids are preferred due to their low cost and effectiveness, since they directly lower IGF II levels 14. Other additional treatments de scribed when the tumor is unresectable include combination chemotherapy with temozolomide and bevacizumab 13.
Within the histopathological diagnosis, these solitary, benign tumors of the pleura tend to be positive for markers like vimentin and other less specific marker such as CD34, bcl-2 or CD99, and negative for cytokeratin 13.
Despite having a low mortality rate (since most of these tumors are benign), it may behave like a malignant tumor, causing more aggressive growth or developing paraneoplastic syndromes.
It is vitally important to consider this syndrome when faced with a solitary fibrous tumor, since hypoglycemia is what may have the most serious effect on these patients.

