











 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkIntroduction
Infectious endocarditis (IE) is a multisystemic disease resulting from an infection, generally bacterial, of the en docardial surface of the heart. Currently, this disease entity is classified according to its diagnostic situation (definite or possible), anatomical site (left/right), type of valve affected (native or prosthetic) and the microorganism involved (bac terium, fungus) 1. Its incidence is three to nine cases per 100,000 people with risk factors 2,3.
Within its pathophysiology, it has been understood that for this disease to develop, several independent factors must appear simultaneously: alteration of the heart valve surface to produce an appropriate site for bacterial insertion and colonization; bacteremia with an organism capable of adhering to and colonizing valve tissue; and the creation of the infected mass or "vegetation" as the proliferating organism is "buried" within a protective molecular ma trix, such as fibrin and platelets. Infectious endocarditis rarely results from intravenous injections of bacteria unless the valvular surface is first disturbed. In human beings, equivalent damage to the valvular surface may be due to a variety of factors, including turbulent blood flow related to primary valve damage, specific systemic disease states such as rheumatic carditis, and mechanical injuries caused by catheters or electrodes. This endothelial injury triggers the formation of fibrin-platelet deposits on the interstitial edema, a pathophysiological entity first named "non-bacterial thrombotic endocarditis" 3.
This causes characteristic pathological changes in mul tiple target organs. Portions of the vegetation's platelet and fibrin matrix may break off the infected heart valve and travel with the arterial blood until they lodge in a vascular bed. Such septic emboli may involve almost any organ system in the body and may manifest clinically in various ways. This is the pathogenic process of embolic cerebrovascular accidents and myocardial, kidney, spleen, mesenteric and skin infarctions 3,4.
The objective of the following paper is to characterize the patients seen at the Hospital Universitario San Rafael de Tunja with a diagnosis of IE.
Materials and methods
This was an observational, descriptive, retrospective cross-sectional study. The study universe was patients seen at the Hospital Universitario San Rafael de Tunja between January 1, 2010 and January 1, 2019 with a diagnosis of IE. Patients with related ICD-10 codes (I33.0, I33.9, I38.0, I39.0) and who were over the age of 18 were included, and patients with incomplete data, those who were referred to another institution for treatment and those who did not meet the previously mentioned inclusion criteria were excluded.
The following variables were reviewed in the clinical charts: sociodemographic (age, sex and comorbidities), clinical (signs and symptoms) paraclinical (complete blood count, acute phase reactants, electrolytes, liver and kidney function), microbiological (blood cultures), imaging (echocardiogram, LVEF and vegetation measurements), treatment (antibiotic and surgical treatment) and outcome (complica tions and sequelae) variables.
The univariate analysis was performed using descriptive statistics of the selected population, determining absolute and relative frequencies of the categorical variables (with their respective 95% confidence intervals [95% CI]). For quantitative variables, central tendency measures were cal culated (mean, median) along with measures of dispersion (standard deviation and interquartile range). The database was recorded on Excel, version 2013, and was analyzed using the SPSS version 22 statistical package, Copyright IBM Corporation (License IBM Z125-3301-14). Based on Resolution 8430 of 1993, this was considered to be a no risk study. Permission was obtained from the ethics and research committee of the Hospital Universitario San Rafael de Tunja to review the clinical charts.
Results
Demographic characteristics of the population
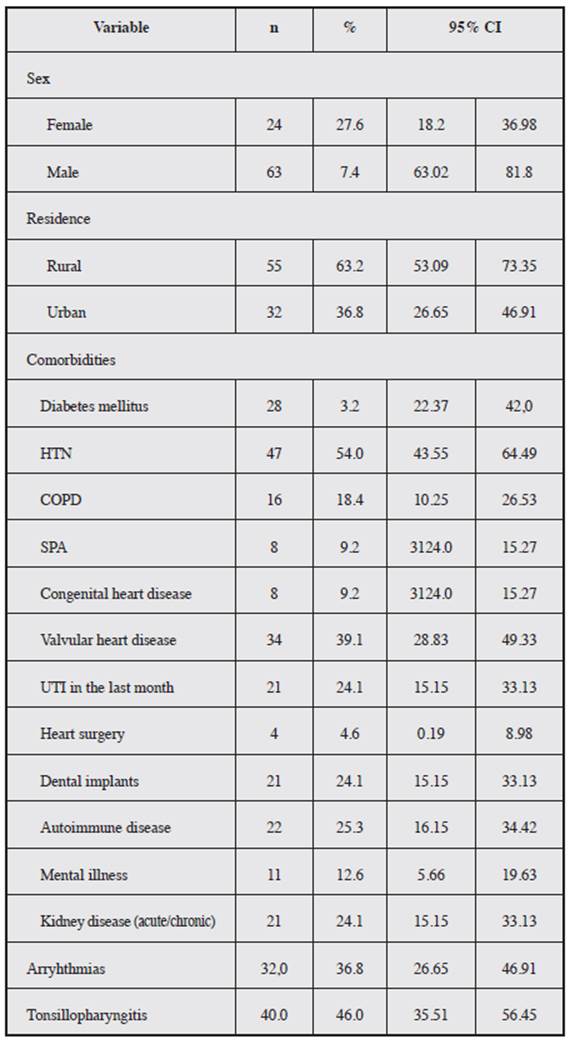
A total of 87 people were seen with a confirmed diagnosis of infectious endocarditis. The average age was 38.77 years, with an SD ± 13.32 years; 72% were males, rural residents, and had certain comorbidities which are shown in Table 1.
Clinical and paraclinical characteristics
The duration of the clinical picture ranged from one to 30 days, with an average of 9.28 days (SD± 7.56 days), with fever and systemic infectious vasculitis signs being the most frequent manifestations (Table 2).
Table 2 Clinical and paraclinical characteristics of patients diagnosed with infectious endocarditis. Etiopathogenic microorganisms isolated.
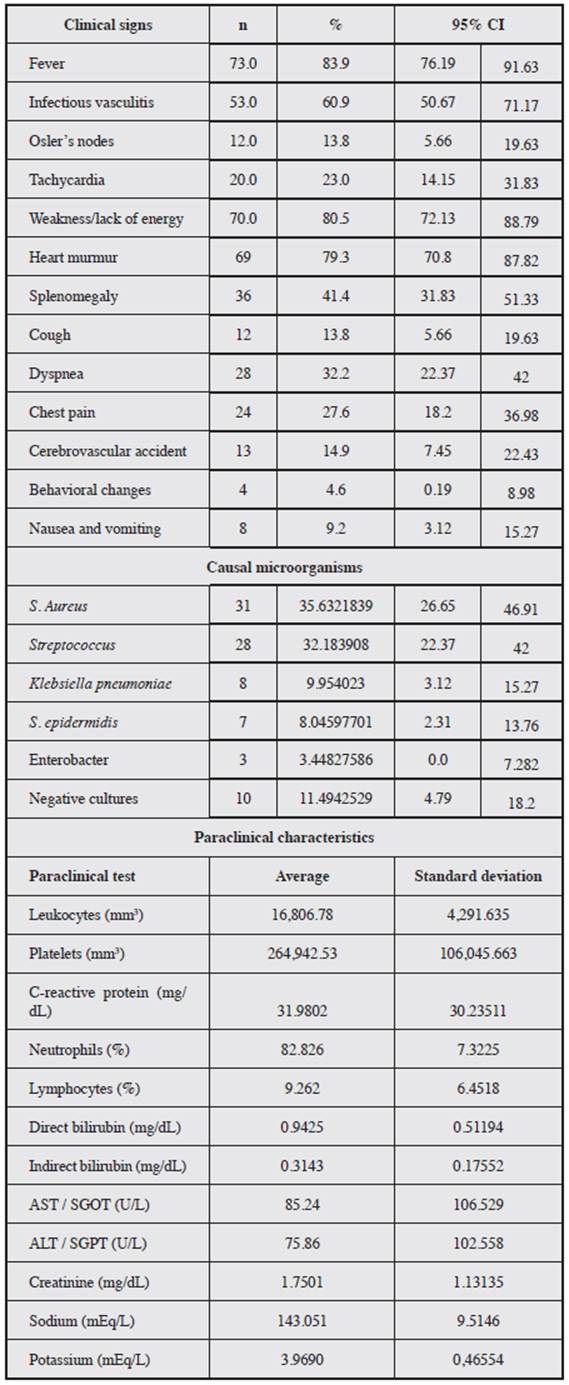
Gram positive microorganisms were the most frequently found in the blood cultures (Table 2). Leukocytosis was found in 90%, neutrophilia in 85%, lymphocytosis in 3%, thrombocytopenia in 4%, increased serum CRP in 85%, transaminitis in 45%, hyponatremia in 2% and hypernatremia in 4% of cases (Table 2).
Imaging characteristics
Most patients (94.3 %) were diagnosed using transthoracic echocardiograms (TTE); only 5.7% required a transesophageal echocardiogram (TEE) to confirm the diagnosis. The most commonly affected heart valves were the mitral and aortic valves; most had moderate regurgitation, and only 4.6% were prosthetic valves (Table 3).
Table 3 Imaging characteristics, with evidence of myocardial valve involvement; most had moderate regurgitation, and only 4.6% were prosthetic valves
The average left ventricular ejection fraction (LVEF) was 60.67% (SD±16.85%). The vegetations had an average width of 1.10 cm (SD±0.49 cm) and an average height of 0.85 cm (SD±0.23 cm).
Treatment, complications and sequelae
All the patients received six weeks of antibiotic treatment, following the institutional protocol, and only 23% required surgical treatment, including three who ultimately required pacemaker implantation due to the severity of the disease (they had high-grade AV block).
The most frequently seen complications were arrhythmias and heart failure, with the latter being a significant sequela for many patients (Table 4).
Discussion
Infectious endocarditis is a potentially fatal systemic infection 4. Despite being a rare disease, its incidence has increased in developed countries, and there are few available studies in developing countries 4,5. Endocarditis is the fourth most important infectious syndrome after urosepsis, pneumonia and intraabdominal sepsis, in the medical depart ments of developed countries 6.
The study population was noted to have a greater preva lence of IE in males, with 72.4%, similar to reports in Latin American and global studies 7,8. The average age was 38.77 years, with an SD ± 13.32, and the majority were rural residents. In this study, the main etiological agents found in the blood cultures were S. Aureus (35.6%), Streptococ cus (32.1%), and Klebsiella pneumoniae (9%). This differs from some studies where agents such as Enterococcus spp were reported, along with a prevalence of those already mentioned 9.
Fever was the main clinical sign followed by weakness and lack of energy. Likewise, there was a high prevalence of heart murmurs and infectious vasculitis, coinciding with the picture reported in other studies 10-12. The less frequent symptoms included cough, Osler's nodes and be havior changes. The most affected myocardial valves were the mitral and aortic valves, in which most had moderate regurgitation, and only 4.6% were prosthetic valves, similar to what has been reported by other authors 13,14. The diagnostic precision of the transthoracic echocardiogram for detecting echocardiographic signs of IE is high, but its effectiveness increases in patients with heart murmurs 15.
The initial treatment for all patients was antibiotics. If heart failure develops or worsens, the patient should be im mediately evaluated for heart surgery, just like the treatment reported in other cases 16. In this study, only 23% needed surgical treatment, including three patients who ultimately required pacemaker placement due to the disease severity (high-grade AV block). The main complications are cardiac and neurological, with heart failure being the main hub, along with hemorrhagic and thrombotic processes 17-19.
The main limitation of the study is the small sample; however, this is due to the low prevalence of this disease, and it could be reproduced, increasing the sample size. Furthermore, the retrospective character of the study is considered to be another limitation, as it allows informa tion bias. However, it was controlled through objective data measurement.
Conclusions
In this case series, similar clinical and microbiological characteristics to those reported in other national and inter national studies were found. Males were affected more than females, with the main causal agent being Staphylococcus aureus Fever and infectious vasculitis signs were the main clinical manifestation, with the mitral valve being the most frequently affected.

