











 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkIntroduction
Estimated glomerular filtration (GF) is an important tool for the clinician, routinely used to identify chronic kidney disease (CKD), monitor kidney function changes and adjust pharmacological treatment in some patients 1-5. There are more precise methods which show real glomerular filtration values, such as clearance of inulin and various isotopes 6,7. Due to the complexity and cost of these techniques, they have been replaced in clinical practice by equations for estimating the GF rate (GFR).
At this time, it has become necessary to determine which of the equations for estimating GFR have the greatest precision for classifying kidney patients. Worldwide, the concordance between the Cockroft-Gault (CG), four-variable Modification of Diet in Renal Disease (MDRD-4) and Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formulas has been established, comparing them with direct measurement based on iothalamate 8. Ever since the CKD-EPI formula was published, the performance of the equations has been compared in various types of populations, finding that the CKD-EPI formula is the most accurate 9-11. Thus, in the KDIGO 2012 guidelines, this formula is used as the basis for classifying patients with CKD 12.
The Colombian 2016 CKD guidelines 13, an adoption of the KDIGO guidelines, have taken CKD-EPI as the formula for estimating glomerular filtration. However, since 2008, when the High Cost Account (CAC in Spanish) was established in Colombia, the equation that has been used to date for defining patients with CKD is CG-SC 14. The reason for using the CG formula is the fact that it is easy to run manually and does not require internet availability, which is needed for the MDRD-4 or CKD-EPI formulas.
The clinicians' feeling is that, in following the CAC guidelines, patients with CKD are being mistakenly classified, since the CG-SC formula is used for all patients without considering that it cannot be used in patients at the extremes of age and weight, those with muscle disease, amputees and/or vegetarians 15,16. The objective of our study is to determine the concordance of GFR measured according to the CG, CG-BSA, MDRD-4 and CKD-EPI formulas in patients with Stage 3a (G3a) to Stage 5 non-dialysis (G5ND) CKD.
Materials and methods
Study population
This was an observational study of individuals seen as outpatients in the nephrology department of a healthcare institution in Cartagena, Colombia, during 2016 and 2017.
The inclusion criteria were: 1) Adult patients over the age of 18 being followed for G3a-G5ND CKD; and 2) Patients with glomerular filtration calculated using the CG (CGeGF), body surface area-adjusted CG (CG-BSAeGF), MDRD-4 and CKD-EPI formulas. 2
The following patients were excluded: pregnant women, lower-limb amputees, vegetarians, and those with active cancer, or primary or secondary muscle disease. Data was gathered on type of health insurance, age, sex, weight, height, body mass index (BMI), etiology of CKD and al buminuria and/or proteinuria.
Glomerular filtration rate estimation
The GFR was calculated in all cases using the CG (mL/ min), CG-BSA, MDRD-4 and CKD-EPI (mL/min/1.73 m2) equations, as described below:
• GF estimated by Cockcroft-Gault (CGeGF) 15:
- Creatinine clearance in men= (140 - age) x (weight) / serum creatinine x 72).
- Creatinine clearance in women= (140-age) x (weight) x 0.85/serum creatinine x 72.
• GF estimated by body surface area-adjusted Cockcroft-Gault (CG-BSAeGF) 15:
- Men= (140 - age) x (weight) x (1.73 m2 / body surface area)/(serum creatinine x 72).
- Women= (140 - age) x (weight) x (1.73 m2 / body surface area) x 0.85 / (serum creatinine x 72).
Body surface area was calculated using the DuBois formula (17): body surface area (m2) = 0.20247 x height (1) 0.725 x weight (kg) 0.425
• GF estimated by four-variable MDRD (MeGF) 18:
- 175 x (serum creatinine / 0.95)-1.154 x (age) -0.2030 x (0.742 if female) x (1.210 if black race).
• GF estimated by CDK-EPI (CKD-EPIeGF) 19:
- 141 x min {creatinine / k, 1} α x max {creatinine / k, 1} -1.209 x 0.993 age [years] x 1.018 [if female], where k is 0.7 for women and 0.9 for men, α is -0.329 for women and -0.411 for men.
The units used in the equations were age in years, weight in kilograms (kg), serum creatinine (Cr) concentration in mg/dL and body surface area (BSA) in m2.
Categories according to GFR
Reduced GF, defined as eGFR <60 mL/min/1.73 m2 was classified in four groups according to the 2012 KDIGO guidelines 12: 45-59 mL/min/1.73 m2 (G3a), 30-44 mL/ min/1.73 m2 (G3b), 15-29 mL/min/1.73 m2 (G4) and <15 mL/min/1.73 m2 (G5). Patients in category G5 under conservative management without dialysis were classified as stage G5ND. Prevalence for each category was described according to the study equations.
Statistical analysis
Descriptive statistics were applied for categorical and quantitative variables, expressing them as frequencies, percentages, mean and median according to the nature of each variable.
The concordance correlation coefficient (CCC) 20 was calculated for all patients between the GFR estimated by CKD-EPI and the GFR estimated by other formulas: MDRD-4, CGeGF and CG-BSAeGF. Concordance was classified according to the CCC as follows: 1=perfect; >0.99=almost perfect; 0.95 to 0.99=substantial; 0.900 to 0.949=moderate; and <0.900=poor.
Glomerular filtration estimated by the CKD-EPI formula was taken as the gold standard (eGFGS) for this study. The eGFGS was compared with MeGF, CGeGF and CG-BSAeGF using the Bland-Altman analysis (21) (a graphical representation of the regression line produced by using the difference in means of the formulas being compared as the dependent variable and the average of the means as the independent variable). Two standard deviations around the mean difference were taken as the limits of agreement between both measurements, as they include 95% of the observed differences. A maximum limit of agreement of ±5 was established between the estimation formulas and the eGFGS (CKD-EPI), considering the definition of ac celerated CKD progression to be a sustained decline in GF greater than 5 mL/min/year.
Bias, precision and accuracy were evaluated among the compared formulas. Bias was assessed as the mean difference in means between the eGFGS and the MeGF, CGeGF and CG-BSAeGF. Precision was defined as the range of the limits of agreement of the mean difference in means (bias) between the eGFGS and the MeGF, CGeGF and CG-BSAeGF estimates. Accuracy was measured as the percentage of results estimated with the different formulas within 15% (P15) and 30% (P30) of the measurements using the eGFGS. A P30 >90% qualifies a formula as satisfactory for clinical interpretation 22. The best formula was defined as the one with the least bias, smallest range of limits of agreement (or best precision) and highest P30. Stata 14 and XLSTAT Premium statistical software were used for analysis.
Ethical aspects
The ethical principles were in accordance with Colombia's Resolution 8430 of 1993. As it was a non-intervention study, with minimal risk, written informed consent was not requested, only verbal consent. The study was approved by the healthcare institution. Data confidentiality, integrity and transparency were respected.
Results
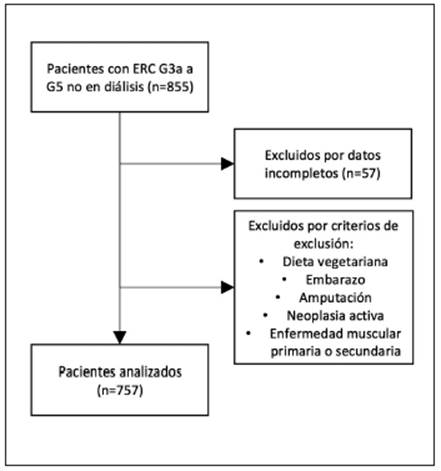
Data were collected from 855 patients, of whom 757 were eligible for the final analysis, having met the inclusion criteria (Figure 1).
Of the subjects analyzed, 61.96% were men and 38% were women; 50.53% had contributory health insurance and 48.68% subsidized. Arterial hypertension was the main cause of CKD (61.43%), followed by diabetes mellitus (31.04%); primary glomerulopathies and other causes made up the remaining 7.53%. The main characteristics of the included individuals are shown in Table 1.
Table 1 General characteristics of the population.
| Characteristic | Mean (N=757) | Standard deviation | 95% CI | |
|---|---|---|---|---|
| Age (years) | 75.36 | 12.16 | 65.3 | 79.4 |
| Weight (kg) | 67.3 | 12.42 | 66.7 | 77.8 |
| Height (cm) | 163.53 | 8.2 | 160.5 | 170.2 |
| BMI (kg/m2) | 25.11 | 4.14 | 24.3 | 28.5 |
| Creatinine | 1.86 | 0.97 | 1.35 | 3.1 |
| GFR by CG (mL/min) | 35.08 | 12.59 | 27.69 | 42.97 |
| GFR by BSA-corrected CG (mL/ min/1.73 m2) | 34.52 | 11.34 | 26.66 | 41.17 |
| GFR by MDRD-4 (mL/min/1.73 m2) | 39.81 | 13.20 | 26.99 | 47.34 |
| GFR by CKD-EPI (mL/min/1.73 m2) | 37.31 | 12.71 | 25.72 | 45.11 |
| Serum albumin (g/dL) | 4.03 | 0.52 | 3.29 | 4.39 |
| Creatinine clearance (mL/min) | 44.57 | 19.85 | 36.14 | 63.52 |
| BMI: body mass index; GFR: glomerular filtration rate; CG: Cockroft-Gault; MDRD-4: four-variable Modification of Diet in Renal Disease; CKD-EPI: Chronic Kidney Disease Epidemiol ogy Collaboration formula. | ||||
Overweight was found in 37.12% of cases, and obesity in 11.2%. The frequency of the CKD stages was different for each of the formulas used (Figure 2). The CG-BSA formula classified a greater percentage of cases as G3b CKD than the MDRD-4 and CKD-EPI formulas. In turn, there was a greater proportion of patients in G4 CKD with CG and CG-BSA: 32.23 and 30.65%, respectively.
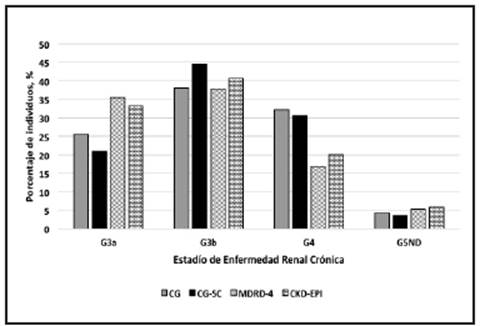
Figure 2 Stages of Chronic Kidney Disease according to the different formulas for calculat ing glomerular filtration rate. CG: Cockroft-Gault; CG-BSA: Cockroft-Gault corrected for body surface area; MDRD-4: four-variable Modification of Diet in Renal Disease; CKD-EPI: Chronic Kidney Disease Epidemiology Collaboration formula; ND: not on dialysis.
Serum albumin was measured in 508 patients (mean 4.0±0.5 g/dL); 90.55% had normal levels and the remaining 9.48% had hypoalbuminemia. The average albuminuria was 481.58±305.73 mg/gr (range: 1-5,009 mg/gr); 53.77% of the albuminuria measurements were in category A1 (<30 mg/ gr), 32.43% in category A2 (30-300 mg/gr), and 13.8% in category A3 (>300 mg/gr).
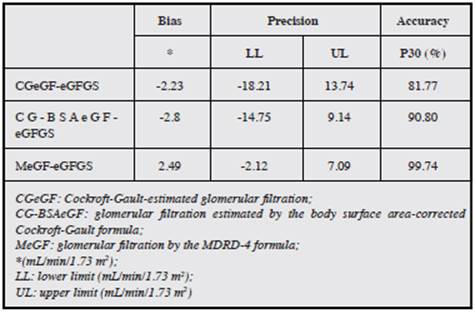
The performance of the various formulas in estimating GFR is shown in Table 2. All the formulas had a small bias with respect to GF by CKD-EPI. The bias was negative for CGeGF and CG-BSAeGF (-2.23 [-2.82 to -1.65] and -2.8 [-3.24 to -2.37] mL/min/1.73m2, respectively) and positive for MeGF (2.49 [2.32 to 2.65] mL/min/1.73m2). Precision was similar between CGeGF and CG-BSAeGF (-18.2 to 13.7 and -14.7 to 9.1 mL/min/1.73m2, respectively); the most precise was MeGF (-2.1 to 7.1 mL/min/1.73m2). The most accurate formula was MeGF, with a proportion of measurements within 15 and 30% of 97.1 and 99.74%, respectively, and the least accurate was CGeGF with 59.7 and 81.77% of the measurements within 15 and 30%, respectively. The con cordance correlation coefficient between eGFGS and MeGF was 0.97, with 0.78 for CGeGF and 0.85 for CG-BSAeGF.
Table 2 Performance of the formulas in calculating glomerular filtration rate compared with CKD-EPI.
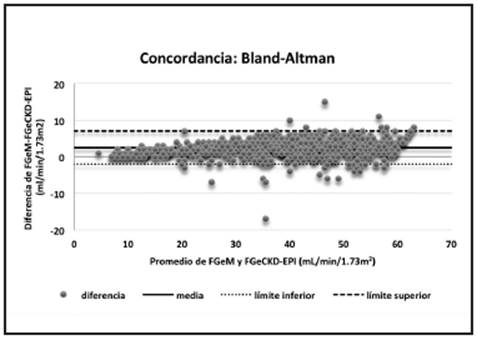
Figures 3-5 show the dispersion graphs for each equation and the differences between MeGF, CGeGF, CG-BSAeGF and eGFGS. The CGeGF Bland-Altman graph has a wide limit of agreement, with predominantly underestimated measurements, but predominantly overestimated G4 and G5 CKD measurements, which is more evident in the CG-BSAeGF graph. Conversely, the MeGF Bland-Altman graph has a narrow limit of agreement with predominantly overestimated measurements, but with measurements around zero (0) in G4 and G5 CKD.
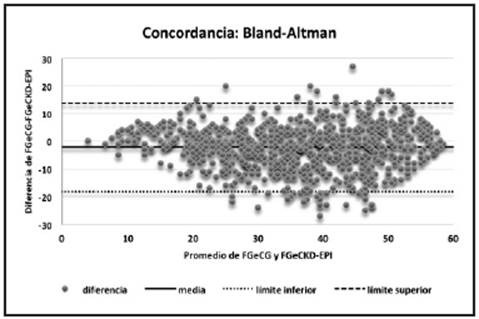
Figure 3 Bland-Altman concordance between CGeGF and CKD-EPIeGF. CG: Cockroft-Gault; CKD-EPI: Chronic Kidney Disease Epidemiology Collaboration formula; CGeGF: CG-estimated glomerular filtration; CKD-EPIeGF: glomerular filtration by CKD-EPI.
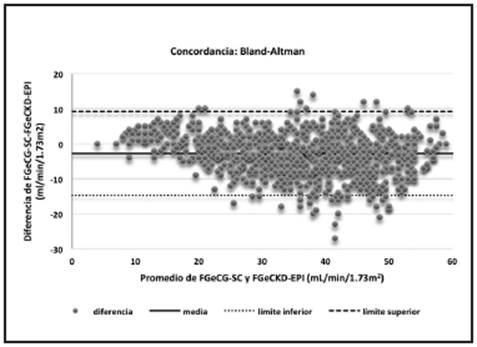
Figure 4 Bland-Altman concordance between CG-BSAeGF and CKD-EPIeGF. CG-BSA: Cockroft-Gault corrected for body surface area; CKD-EPI: Chronic Kidney Disease Epidemiology Collaboration formula; CG-BSAeGF: glomerular filtration estimated by CG-BSA; CKD-EPIeGF: glomerular filtration estimated by CKD-EPI.
Discussion
All GFR estimation formulas should be validated in the population in which they are to be used. The current study is the first to attempt to validate the bias, precision, accuracy and concordance between each of the formulas for measuring GFR in the Colombian population, using GFR estimated with the CKD-EPI formula as the gold standard.
In our study, we found that the MDRD-4 formula had the best performance with respect to precision, accuracy and concordance relative to the CKD-EPI formula. The precision did not exceed the established limit of a range of 10 for limits of agreement (from -5 to +5), with precision being better at the eGFGS underestimation limit. The accuracy is almost perfect, and concordance is in the substantial range. On the other hand, GFR estimates using the CG and CG-BSA equations were widely dispersed with respect to the eGFGS, both with a range of limits of agreement over the established limit, with borderline accuracy for CG-BSAeGF alone, but poor concordance for both.
In Colombia, the CKD-EPI formula has not been validated, but it has been validated internationally, including the Latin American population. In 2014, a study of healthy Mexicans with an average age of 35 took direct GFR measurements obtained by an isotope or radiopharmaceutical (Tc-DTPA: Tc99m-DTPA [diethylenetriaminepentaacetic acid]) as a reference and subsequently compared them with GFR values estimated by CKD-EPI and MDRD-4. The GFR calculated by CKD-EPI was found to have a greater concordance with the direct measurement reference values23. Similar results were obtained by Veronese FV, et al.24 in a study including healthy, diabetic and CKD patients. Despite having different population characteristics, the two studies demonstrated that CKD-EPI is a better predictor of GFR. However, in Colombia, the CAC categorizes GFR by CGeGF 14. Nevertheless, CGeGF's results cannot be generalized, given their high heterogeneity as BMI increases 25,26, and its performance is inferior to GFR estimated by MDRD-4 and CKD-EPI formulas, as has been reported in the previously mentioned studies and others in various population groups 27,28. These findings are consistent with our results.
Kuo CF et al., in a study of 32,542 healthy individuals undergoing routine studies, compared GFR estimated by six-variable MDRD (MDRD-6), MDRD adjusted to the Chinese population and CG. The estimation of GFR, CKD risk factor assignment and stratification differed significantly between the three equations, especially with the CG equation. The CG formula produced a lower GFR and, paradoxically, higher measurements in patients with hyperuricemia, hypertension, and metabolic syndrome than in those without these risk factors. In this study, as well as in ours, the use of the CG formula for CKD screening is discouraged, and the MDRD formula adjusted to the Chinese population is recommended for that population 29.
On the other hand, the previous data contrast with results obtained by Liu X et al. who reported that the CG formula was the most precise for estimating GFR at different stages of chronic kidney disease in older adults 30. Hence the importance of our study to validate the CG and MDRD-4 formulas in the Colombian population, using the globally recommended CKD-EPI formula as reference, which has also been accepted in our country, according to the guidelines adopted in 2016. In the study population, we found that the performance of MDRD-4 was statistically better in all the study variables with respect to CGeGF and CG-BSAeGF; it was also more accurate in estimating GFR. Similar to our results, the data obtained by Schwandt A, et al. 31 concur in that the MDRD-4 formula performed better globally, and had greater precision and less bias. In this last study, the parameter used as the gold standard was GFR estimated by 24-hour urine creatinine clearance.
Chudek J, et al. 32 also compared the performance of the MDRD-4, MDRD-6 and CG equations specifically in patients 65 years old and older. The MDRD-6 formula was found to have the best concordance, precision and accuracy, compared to CG, for all CKD groups. Related results in favor of the precision of MDRD in elderly patients were demonstrated in another study performed by Aras S et al. 33.
Finally, Zaman SB 34, in a study of 4,042 type 2 dia betic patients, reported a correlation coefficient between GFRs estimated by CKD-EPI and MDRD-4 of 0.90 (95% CI 0.83 - 0.97, p < 0.001). However, this study found that the correlation coefficient between the CKD-EPI equation and CG was 0.56 (95% CI: 0.44 - 0.67, p <0.0001), even lower than what was found in our caseload.
The current study has the strength of having been performed on a significant number of CKD patients not on dialysis, and comparing for the first time the eGFGS (CKD-EPI), globally recommended and adopted in Colombia in the 2016 CKD guidelines, with alternative estimation formulas used in Colombia: MDRD-4, and the one used by the CAC, CG-BSAeGF. Despite the fact that the data are solid and have clinical significance, reporting a global analysis of the data of patients in Cartagena, its weaknesses lie in not considering a stratified analysis according to CKD stage and patient subgroups of ages and average and extreme weights that can show similar findings.
Conclusion
Our findings suggest that the classification of CKD categories in Colombia should be based on the CKD-EPI formula, as is recommended internationally based on direct measurements with inulin and radiopharmaceuticals. Using the alternate CG-BSA formula is not advisable, despite its easy manual use, as this study has shown that it has low precision and accuracy, which could lead to a greater classification of elderly patients in this population in early stages, such as G3a CKD, with the corresponding consequences for the patient and the healthcare system.
Thus, the most precise, accurate and concordant alternate formula for estimating glomerular filtration in this Colombian population is MDRD-4, although online methods would be required for its calculation, just like CKD-EPI. The Cockroft-Gault formula has low precision, borderline accuracy and poor concordance with the CKD-EPI formula. It is recommended that the CG-BSA formula for GFR estimation not be used to classify CKD in Colombia.

