











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Cerebrovascular disease (CVD) entails a significant burden of morbidity and mortality today 1-3. According to data from the 2013 global burden of disease study 1, cerebrovascular accidents (CVAs) were the second cause of mortality worldwide (11.8% of deaths) after acute myocardial infarction, and the third cause of disability (4.5% of disability-adjusted life years for all causes). Cerebrovascular disease is also the second cause of death in Colombia 2, with a 2016 mortality rate of 31.99 per 100,000 inhabitants 3.
A CVA is defined by the American Heart Association (AHA) as a demonstrable neurological deficit attributed to focal damage of the central nervous system and due to a vascular cause 4. Within the treatment of acute ischemic CVA, reperfusion therapies play a key role as the most effective alternatives for rapidly re-establishing oxygen supply to the tissues, thus seeking the patient's functional recovery 5,6.
The need to shorten the time between the onset of symptoms and reperfusion therapy has led to the design of thrombolysis networks, programs and protocols in the in stitutions which care for patients with acute ischemic CVA. In this context, some parameters have been established to measure the proper functioning of these programs, including door-to-needle time and door-to-imaging time 6.
The E.S.E. Hospital San Rafael de Tunja is a public ter tiary care institution which is a reference center for Boyacá Department and neighboring departments, thus covering a broad geographic area. The institution has a cerebral throm bolysis program which began to function in 2012.
This paper describes the sociodemographic and clinical characteristics, inpatient outcomes and rate of complications of the population of patients who have received intravenous thrombolysis due to ischemic CVA at the E.S.E. Hospital San Rafael de Tunja in the last six years. In addition, the door-to-needle and door-to-imaging times are reported, as some of the care quality indicators listed for thrombolysis programs.
Materials and methods
This is a retrospective observational study carried out in a population of patients who received intravenous thrombolysis due to a diagnosis of ischemic CVA at E.S.E. Hospital San Rafael de Tunja, Boyacá between January 1, 2014 and June 30, 2019.
First, the physical thrombolysis register in the institu tion's resuscitation room was reviewed to identify the total number of patients. With the approval of the institutional research and bioethics committee, the clinical charts were reviewed, and a database constructed based on this review. This study is aligned with the ethical principles for human research stated in the Declaration of Helsinki 7. Due to its retrospective nature, informed consent was not required.
The inclusion criteria were: patients over the age of 18, a diagnosis of ischemic CVA as proposed by AHA in 2013 4, and intravenous thrombolysis using recombinant tissue plasminogen activator performed at the E.S.E Hospital San Rafael de Tunja. The exclusion criteria were: telemedicine-directed thrombolysis, hemorrhagic CVA and incomplete clinical charts or those that were not found in the institution's statistics and archive office.
The population's main sociodemographic characteristics were taken, along with the prevalence of premorbid cardio vascular risk factors, clinical variables associated with the CVA event [vascular territory of the CVA, length of hospital stay, time elapsed from the onset of symptoms-arrival at the hospital, time elapsed to assessment by physical therapy, National Institutes of Health Stroke Scale (NIHSS) 8 score on admission[, inpatient outcomes (inpatient mortality and NIHSS score at discharge), most relevant inpatient complica tions (hemorrhagic transformation, aspiration pneumonia, and pressure sores) and quality indicators of the thrombolysis program (door-to-needle and door-to-imaging times).
The NIHSS score was determined by the neurologist on duty both at patient admission as well as discharge. This was further categorized according to Muchada et al.'s proposal in 2014 9 as follows: mild ≤8 points, moderate 9-15 points and severe ≥16 points. For hemorrhagic transformation, the Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST) was used, which conceptualizes it as a parenchymal space-occupying hemorrhage which covers more than 30% of the infarcted area, as seen on imaging 22 36 hours after thrombolytic treatment 10. We also analyzed whether the hemorrhagic transformation was associated with neurological deterioration quantified using the NIHSS score. For the pressure sores variable, the diagnosis was tracked in the clinical charts, and an active search was performed comparing this study's database with the institution's healthy skin service and wound clinic databases.
The statistical analysis was performed using Microsoft® Excel®, Mac Version 14.4.3 -140616-, 2011. Frequency distributions and proportions were calculated for categori cal variables, and measures of central tendency with their respective measures of dispersion were calculated for con tinuous variables.
Various biases could be present in this study, includ ing selection bias. To avoid this, inclusion and exclusion criteria were specified. Another possible bias is informa tion bias, which was controlled for by specifying a list of variables to be analyzed from the beginning; in addition, those in charge of collecting data were aware of how to complete the database.
Results
A total of 166 patients were identified in the physical register as having received thrombolysis due to a diagno sis of ischemic CVA at the E.S.E. Hospital San Rafael de Tunja between January 1, 2014 and June 30, 2019. Three patients were excluded due to having been thrombolyzed by telemedicine, two due to incomplete medical charts, and five because their clinical charts were not available in the institution's office of statistics and archives. The final included population was 156 patients: 24 from 2014, 30 from 2015, 35 from 2016, 29 from 2017, 22 from 2018 and 16 from 2019.
The population's average age was 66.1 years, with a range from 30 to 92 years. The sociodemographic characteristics are shown in Table 1. The clinical variables, outcomes, complications and inpatient mortality are shown in Table 2.
Table 1 Sociodemographic characteristics of the population.
| Variable | colspan="2">Frequency (N) (%) | ||
|---|---|---|---|
| Age group (n= 156) | Under 65 years | 37.2 (58) | |
| Between 65 and 79 years | 51.9 (81) | ||
| 80 years or older | 10.9 (17) | ||
| Sex (n= 156) | Male | 49.4 (77) | |
| Female | 50.6 (79) | ||
| Place of origin (n= 156) | Boyacá | 91.7 (143) | |
| Tunja 31.5 (45) | Other towns 68.5 (98) | ||
| Santander | 6.41 (10) | ||
| Others | 1.9 (3) | ||
| Zone of origin (n= 156) | Urban/county seat | 62.8 (98) | |
| Rural | 37.2 (58) | ||
| Type of health insurance (N= 156) | Contributory | 37.8 (59) | |
| Subsidized | 57.7 (90) | ||
| Special | 4.5 (7) | ||
| Source: Authors. | |||
Table 2 Clinical variables, outcomes and inpatient complications associated with the CVA event.
| Variable | Frequency (N) % | |
|---|---|---|
| Vascular territory of the CVA (n= 156) | Left middle cerebral artery | 46.2 (72) |
| Right middle cerebral artery | 44.9 (70) | |
| Posterior circulation | 3.9 (6) | |
| Lacunar | 2.6 (4) | |
| Multitopographic | 1.9 (3) | |
| Anterior cerebral artery | 0.6 (1) | |
| Pre-morbid risk factors associated with CVA (n= 156) | Arterial hypertension | 66 (103) |
| Diabetes mellitus | 16.7 (26) | |
| History of prior CVA | 14.7 (23) | |
| Smoking | 10.9 (17) | |
| Atrial fibrillation | 10.3 (16) | |
| Coronary diseasea | 10.3 (16) | |
| Dyslipidemia | 2.6 (4) | |
| Inpatient mortality (n= 156) | Total | 14.7 (23) |
| Due to hemorrhagic transformation after thrombolysis | 2.6 (4) | |
| Due to edema associated with ischemic CVA | 7.1 (11) | |
| Due to aspiration pneumonia | 2.6 (4) | |
| Due to other causes | 2.6 (4) | |
| Hemorrhagic transformation after thrombolysis (n= 156) | Total | 10.9 (17) |
| With neurological deterioration | 3.2 (5) | |
| Without neurological deterioration | 7.7(12) | |
| Aspiration pneumonia during hospitalization (n= 156) | 5.1 (8) | |
| Pressure sores during hospitalization (n= 156) | 0.6 (1) | |
| Source: Authors. | ||
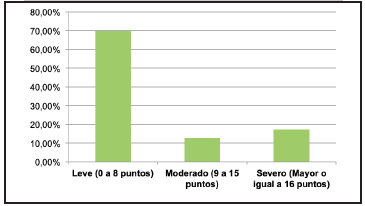
Altogether, 48.72% of the patients were admitted with a moderate NIHSS score (between 9 and 15 points), while 69.9% of the patients were discharged with a mild score or with no deficit (between 0 and 8 points). Of the patients who survived, 92.5% improved their NIHSS score during hospitalization, with an average 6.9 point decrease (SD 4.9). The rate of hemorrhagic transformation after thrombolysis was 10.9%, and only five patients (3.2% of the total) had neurological deterioration related to the hemorrhagic trans formation. The admission and discharge NIHSS scores are found in Table 3 and are diagrammed by severity category in Figures 1 and 2.
Table 3 Admission and discharge NIHSS scores.
| Variable | Mean | Standard deviation (SD) | Median | Interquartile range (IQR) |
|---|---|---|---|---|
| Admission NIHSS score (N= 156) | 12.4 | 5 | 12 | 7 |
| Discharge NIHSS score (N= 133) | 4.8 | 4.48 | 4 | 7 |
| Source: Authors. | ||||

The key times for programs caring for patients with acute ischemic CVA are shown in Table 4. In 59% of the cases, the door-to-needle time was less than 60 minutes and in 43.6% it was less than 45 minutes. Furthermore, in 63.7% of the patients, the door-to-imaging time was less than 20 minutes.
Table 4 Key times for acute ischemic CVA care programs.
| Variable | Mean | Standard deviation (SD) | Median | Interqnartile range(IQR) |
|---|---|---|---|---|
| Length of hospital stay (days) | 8 | 7.7 | 6 | 5 |
| Time elapsed from onset of sym¡Xoms to arrival al the hospital (hours) | 2.7 | 1.29 | 3 | 1.5 |
| Door-to-imaging time ( minutes) | 23.5 | 27.42 | 16 | 25.5 |
| Door-to-needle time (minutes) | 62.8 | 42.95 | 50 | 52.5 |
| Time elapsed to assessment by physical therapy (hours) | 47.5 | 51.6 | 24 | 48 |
| Source: Authors. | ||||
Discussion
Worldwide, only 2-10% of patients with ischemic CVA are thrombolyzed 10. This study describes the largest population of patients receiving thrombolysis for ischemic CVA to date in Colombia (156), compared to studies from the Hospital Universitario San Ignacio (24 patients) 12, Hospital Universitario Fundación Santa Fe de Bogotá (70 patients) 13 and Fundación Hospital Universidad del Norte (27 patients) 14.
The benefit of intravenous thrombolysis in terms of mortality and dependence for patients with ischemic CVA is widely recognized in the literature (OR 0.85 three to six months after the event, according to a recent meta-analysis) 15, especially with the implementation of multidimen sional programs which extend the intervention's reach 6,16-18. The results of our program show an improvement in the NIHSS score in most thrombolyzed patients, with a mean decrease of more than 4 points, which favors the clinical effectiveness of this treatment. The average dis charge NIHSS score found 4.8 is lower than that reported in the Colombian studies from the Hospital Universitario Fundación Santa Fe de Bogotá 7,13 and the Fundación Hospital Universidad del Norte 9,14.
The main adverse event related to thrombolysis in ischemic CVA is symptomatic intracranial hemorrhage 15. The total hemorrhagic transformation rate at our institu tion (10.9%) is higher than that reported in the Colombian Hospital Universitario Fundación Santa Fe de Bogotá study (4%) 13, and Tosta et al.'s study in Brazil (6%) 19. The rate of hemorrhagic transformation with neurological deterioration (3.2%) is lower than reported in Khan et al's study in Dubai (6.8%) 20, but slightly higher than that of the Hospital Universitario Fundación Santa Fe de Bogotá (2.8%) 13 and the SITS-MOST study (1.7%) 21. The inpatient mortality rate (14.7%) is higher than that reported in the Hospital Universitario San Ignacio (12.5%) 12 and the Hospital Universitario Fundación Santa Fe de Bogotá (9%) 13 studies, and very similar to the rate reported in the Chilean study by Guevara et al. (14.8%) 22, also car ried out in a public hospital. Altogether, 2.6% of the study patients died from hemorrhagic transformation related to the thrombolytic procedure.
With regard to inpatient complications, the rate of aspi ration pneumonia found (5.1%) is lower than what was re ported in Licona et al.'s study in 2009 (12.5%) 23, Wilson'sstudy in 2012 (8.1%) 24, and the rate of chest infections reported by Langhorne in 2000 (22%) 25. Moreover, the rate of pressure sores (0.6%) is lower than that reported by Amir et al. in 2013 (22%) 26 and by Langhorne (21%) 25, but higher than that reported by Bilir in 2019 (0%) 27. The data supplied by the other Colombian studies 12-14 do not allow a comparison with the rate of complications found in our institution.
The average length of hospital stay found in this study (eight days) is lower than that reported in the other Co lombian studies (10.8 days and 10.4 days) 12,13 and in Canada (34-47 days), but higher than what is reported in the United States (six days) 28. The time elapsed from the onset of symptoms to arrival at the hospital was greater than that reported in national and international studies 13,14,19,20-31, which could be related to the broad geographical area from which our population was derived, together with the delays in the region's ambulance system, a problem which has already been discussed in other Co lombian departments 32.
On the other hand, the door-to-needle and door-to-im aging times were lower than those in the other Colombian studies 13,14 and most of the international studies 19,22,30,33. Although some of these studies included data from before 2014, these lower times could be related to continuous communication of the thrombolysis program in our area of influence, which leads to early activation of the CVA code by the referral site and expedites care at the receiving center. In 2018, AHA established a primary objective for the door-to-needle time of 60 minutes in ≥50% of thrombolyzed patients and a secondary objective of less than 45 minutes in ≥50% of thrombolyzed patients 6. With regard to door-to-imaging time, a goal was set of less than 20 minutes in at least 50% of the patients who may be candidates for reperfusion therapy 6. The data confirm that E.S.E. Hospital San Rafael de Tunja meets the primary door-to-needle time objective and the door-to-imaging time objective proposed by the AHA 6.
In this study, it is noteworthy that most of the population came from towns other than Tunja, the city in which the insti tution is located. This supports the usefulness of establishing regional networks for managing CVA, as has been proposed in the recent evidence 6,16-18. In addition, it should be highlighted that the Boyacá thrombolysis network has been complemented since 2019 with telemedicine, as a recognized strategy for optimizing reperfusion therapy times and thus improving patient outcomes 34,35. E.S.E. Hospital San Rafael de Tunja implemented the first telethrombolysis ex perience in Colombia together with E.S.E. Hospital Regional de Duitama, and will soon do so with four more institutions in four other cities in the department of Boyacá.
Conclusion
Cerebrovascular disease incurs a significant burden of morbidity, mortality and disability 1-3. Reperfusion strate gies are recognized as the fundamental pillar of treatment, and therefore should be improved through the implementa tion of programs, construction of care networks and use of tools such as telemedicine 5,6,17,18,34,35. The results obtained contribute to strengthening the epidemiological data on ischemic CVA and thrombolysis programs in Co lombia and Latin America.

