











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
The estimated lifetime risk of developing herpes zos ter (HZ) is approximately 30% 1-4. In North America, Asia and Europe, the annual incidence rates of HZ in the overall population are 3-6/1,000 person-years (PYs) 5,6, increasing to 6-11/1,000 PYs in those over the age of 60 3,5,6 and 8-13/1,000 PYs in those over 80 5-7. Latin American estimates of HZ, however, are scarce. A Brazilian study by Castro et al. evaluated visits to an emergency dermatology clinic over 27 months, reporting an incidence rate of approximately 5.6/1,000 PYs 8. In Colombia, 9 the estimated incidence of HZ is limited to the results of a case-control study carried out at an oncology clinic, which found HZ in 0.65% of the check-ups of 11,560 patients without malignant disease 9.
Although the clinical picture varies, the onset of HZ is generally characterized by a prodrome of pain, followed by the appearance of a unilateral dermatomal rash several days later 10,11. It takes two to three weeks for the rash to clear, and the pain during this acute phase is moderate to intense in most patients 10-12. In a subgroup of patients, the pain persists even after the rash has cleared, which is known as postherpetic neuralgia (PHN). It has been deter mined that both acute and chronic HZ pain, the incidence and intensity of which are positively correlated with age 4, negatively affect the quality of life (QL) 12,13. The prompt administration of antiviral medications, which have been proven to mitigate the intensity and duration of HZ in the acute phase, has not been conclusively related to a reduced incidence of PHN 14, although it has been determined that prophylactic immunization against zoster reduces both the burden of the acute phase of the disease as well as the incidence of PHN 15. A study by Baxter et al. showed that the long-term efficacy of a prophylactic zoster vaccine is 67.5% one year after the vaccination, with a reduction to 47.2 and 31.8% after two and eight years, respectively, yielding a general vaccine efficacy of 49.1% 16.
At the moment, there are no available data on the clini cal presentation of HZ, its impact on patients' wellbeing, and its real-life management in Colombia. The objectives of this study were to describe the real-life burden of HZ in Colombia, including HZ-related pain, the use of resources and its impact on quality of life.
Methods
Study design
This was a prospective, observational single cohort study carried out at 10 clinical centers in Colombia, five specializing in internal medicine (one in Bogotá, one in Cali, one in Manizales and two in Medellín), two in fam ily/general medicine (one in Bogotá, one in San Gil) and one in each of the following: neurology (in Bucaramanga), endocrinology (in Barranquilla) and dermatology (in Bogotá). The purpose of the study was to calculate the burden of disease attributed to HZ both in incident cases, defined as patients with an HZ episode lasting less than seven days before being included in the study, as well as prevalent cases, defined as patients who were included after this seven-day window but within 90 days of the onset of the rash.
The study involved minimal risk according to Resolu tion 8430 of 1993, was reviewed and approved by the appropriate local ethical review organisms, and was car ried out according to the Guidelines of the International Conference on Harmonization for Good Clinical Practice and the principles of the Declaration of Helsinki.
Study population
Patients with HZ were enrolled at the offices of their attending physicians over a period of 18 months. To be eligible to participate, patients had to: 1. have a medically confirmed diagnosis of acute phase HZ or postherpetic pain, with a main diagnosis within 90 days of the enroll ment visit; 2. be at least 50 years old at the onset of the HZ rash; 3. be able to understand and complete the study questionnaires, and 4. be able to give informed consent. Immunocompromised patients were excluded from the study, with immunocompromise defined as the following: 1. the presence of immunosuppressive diseases, 2. the use of corticosteroids (except for topical or intermittent inhaled steroids), 3. receiving immunosuppressant or cytotoxic therapy, or 4. the presence of any neoplastic disease, other than localized skin cancer or other stable, solid malignant tumors with no immunosuppressive or cytotoxic treatment.
Study schedule and assessments
Follow up was for six months, regardless of the HZ phase at the time of enrollment. In the case of eligible patients who provided informed consent, sociodemographic and baseline disease characteristics were recorded at enrollment (day 0). The burden of disease was assessed using the evaluations described below.
At enrollment, quality of life (QL) prior to the HZ episode was evaluated using Euro-QoL (EQ-5D) 15, a consolidated QL tool designed to be completed automatically. The EQ-5D index score is calculated by evaluating five dimensions, specifically mobility, self-care, usual activities, pain/discom fort and anxiety/depression. These dimensions grade the patient's health status at five different levels: no problems, slight problems, moderate problems, serious problems and extreme problems. The overall health perception was also graded using the 100 mm visual analog scale (VAS) attached to the EQ-5D, on which higher scores indicate a better QL. Although its aim was prospective data collection, a previous study by Wilson et al. concluded that, despite the risk of a small upward bias, the retrospective use of EQ-5D is more appropriate than the use of population norms for evaluating quality of life before the onset of an acute injury/disease 18.
The Initial Zoster Impact Questionnaire (IZIQ) 19 was also administered to gather information related to the burden of prodromal pain on a scale of 0-10, where 0 is "no pain" and 10 is "the worst possible pain." A pain score of 7 to 10 or more was considered to be intense.
Follow up consisted of telephone interviews on days 30, 60, 120 and 150. Office interviews were also scheduled for day 90 and day 180 (the end of study visit). At all visits, including enrollment (day 0), the patients completed the following questionnaires, either self-administered or admin istered by the interviewer: the Zoster Brief Pain Inventory (ZBPI) 19, scored according to the previously described IZIQ, and, to assess current QL, information related to acute phase pain (current and worse/less/average in the last 24 hours) and the EQ-5D and VAS indices.
The use of healthcare resources (UHCR) was also evalu ated with a simple questionnaire which asked patients if they had sought additional medical care due to HZ since the last study visit/telephone interview. In addition, concomitant HZ treatment and the incidence of PHN (defined as a ZBPI score of HZ-related "pain in the last 24 hours" >3 lasting 90 days after the onset of HZ symptoms) were evaluated at all visits.
Only in incident HZ cases, patients were also requested to complete the ZBPI, EQ-5D and UHCR questionnaires on days 7, 14 and 21 and submit them by mail or take them to the following office study visit on day 90.
Statistical analyses
Analyses were performed on the general study cohort. Descriptive statistics were developed for all the study vari ables, which included the mean, median and 95% confidence interval (CI) of the mean for continuous variables, as well as distribution frequencies for categorical variables. The EQ-5D index score was calculated according to the Latin American preference weights 20.
The burden of pain due to HZ was estimated from the area under the curve (AUC) of the ZBPI measure of "worse pain in the last 24 hours" against the time since the onset of symptoms, where symptom onset refers to rash or pain, whichever came first. The burden of pain predictors were identified using mixed multivariate models with repeated measures, adjusted by the duration of the onset of HZ symp toms reported at enrollment and considering the following covariables according to what was reported at enrollment: the age at the onset of HZ symptoms; educational level; employment status; medications for HZ; number of lesions at enrollment; incident vs. prevalent HZ and the worst prodro mal and general pain scores. Retroactive variable selection was used to derive the parsimonious model.
All analyses were performed using SAS version 9.4 software (SAS Institute Inc., Cary, NC).
Results
Sociodemographic characteristics
Table 1 presents the study cohort's sociodemographic characteristics at enrollment. The overall mean age (SD) was 64.6 (9.6) years, 35.7% of the patients were between 50 and 59 years old, 38.3% were 60 to 69 years old, and 26.0% were over 70. Most of the patients were female (62.3%; n = 96) and Hispanic (65.6%; n = 101). Regarding education, a little over 55% (n=87) of the patients reported a primary or secondary level of education. Altogether, 20.8% (n=32) of the patients reported working full time, 7.8% (n=12) reported working part time, and 35.7% (n=55) were retired.
Table 1 Patients' sociodemographic characteristics.
| Parameter | Total cohort N = 154 |
|---|---|
| Age at onset of symptoms, years, mean (SD) | 64.6 (9.6) |
| Range of age at onset of symptoms, years, n (%) | |
| 50-59 | 55 (35.7) |
| 60-69 | 59 (38.3) |
| >70 | 40 (26.0) |
| Sex, female, n (%) | 96 (62.3) |
| Race, n (%) | |
| Caucasian | 24 (15.6) |
| Black | 1 (0.6) |
| Hispanic | 101 (65.6) |
| Other | 28 (18.2) |
| Highest level of education, n (%) | |
| Primary | 56 (36.4) |
| Secondary | 31 (20.1) |
| Associate degree | 23 (14.9) |
| University | 25 (16.2) |
| Graduate studies | 19 (12.3) |
| Current employment status, n (%) | |
| Full-time | 32 (20.8) |
| Part-time | 12 (7.8) |
| Retired | 55 (35.7) |
| Unemployed | 9 (5.8) |
| Not working due to disability | 2 (1.3) |
| Full-time homemaker | 30 (19.5) |
| Other | 14 (9.1) |
| Immunity status, n (%) | |
| Normal | 107 (69.5) |
| Compromised1 | 47 (30.5) |
| 1 Compromised includes the following: vitamin/mineral insufficiency (n = 1); stressful/exhausting lifestyle (n = 18); excessive cigarette smoking (n = 8); alcohol abuse (n = 3); intermittent use of topical/inhaled corticosteroids (n = 2); autoimmune disorder (n = 8); allergic disorder (n = 20); stable malignant tumor (n = 1). Patients may have reported more than one immunological condition. | |
Herpes zoster characteristics
The characteristics of the HZ disease are summarized in Table 2. The mean length (SD) of HZ symptoms prior to the enrollment visit was 35.9 (24.0) days, and 93.5% (n = 144) of the HZ cases were classified as prevalent. The mean time elapsed (SD) from the onset of the rash at enrollment was 21.3 (17.6) days. Among the patients who reported a rash at enrollment (n = 87; 56.5%), the most commonly affected main dermatome was the thoracic dermatome (n = 40; 26.0%), and the number of lesions present on the main dermatomes and adjacent to them were divided mainly between 1-20 lesions (n = 34; 22.1%), 11-20 lesions (n = 24; 15.6%) and 21-50 lesions (n = 22; 14.3%).
Table 2 Disease characteristics.
| Parameter | Total cohort N = 154 |
|---|---|
| Time elapsed since the onset of HZ symptoms, days, mean (SD) | 35.9 (24.0) |
| HZ case group, n (%) | |
| Incident | 10 (6.5) |
| Prevalent | 144 (93.5) |
| Time elapsed since the onset of the rash, days, mean (SD) | 21.3 (17.6) |
| HZ rash present at enrollment, yes, n (%) | 87 (56.5) |
| Principal dermatome area affected, n (%) | |
| Trigeminal nerve | 17 (11.0) |
| Cervical | 16 (10.4) |
| Thoracic | 40 (26.0) |
| Sacral | 4 (2.6) |
| Lumbar | 10 (6.5) |
| Not applicable | 67 (43.5) |
| Number of lesions on the principal and adjacent dermatomes, n (%) | |
| None | 2 (1.3) |
| 1-20 | 34 (22.1) |
| 11-20 | 24 (15.6) |
| 21-50 | 22 (14.3) |
| 51-100 | 5 (3.2) |
| Not applicable | 67 (43.5) |
| Prodromal pain, yes, n (%) | 109 (70.8) |
| Duration of the pain prior to the onset of the rash, days, mean (SD) | 5.2 (8.8) |
| Worst pain, mean (SD)1 | 7.2 (2.7) |
| Average pain, mean (SD) 1 | 5.8 (2.6) |
| HZ pain since the onset of HZ rash, yes, n (%) | 147 (95.5) |
| Duration of pain, days, mean (SD) | 17.6 (15.0) |
| Worst pain, mean (SD)1 | 8.2 (2.1) |
| Average pain, mean (SD) 1 | 6.0 (2.0) |
| HZ treatment begun, yes, n (%) | 150 (98.7%) |
| Medication for HZ, n (%)2 | |
| Acyclovir | 131 (85.1) |
| Acyclovir (dermatological use) | 86 (55.8) |
| Carbamazepine | 32 (20.8) |
| Diclofenac | 25 (16.2) |
| Acetaminophen | 71 (46.1) |
| Pregabalin | 66 (42.9) |
| Tramadol | 44 (28.6) |
| Valacyclovir | 25 (16.2) |
| Patients with PHN, n (%)3 | 54 (36.5) |
| SD: standard deviation, HZ: herpes zoster, PHN: postherpetic neuralgia. 1 Classified on a scale of 1 (no pain) to 10 (the worst pain imaginable); determined at the enrollment visit. 2 The medications for HZ presented are those reported by >15% of the patients. 3 Six prevalent cases with <90 days of follow up from the onset of symptoms were not evaluated; the percentage is based on n = 148. | |
A total of 70.8% of the patients reported prodromal pain; the mean duration (SD) was 5.2 (8.8) days before the onset of the rash, and the mean worst pain (SD) was 7.2 (2.7). Altogether, 95.5% of the patients had acute HZ pain (n=147), with mean scores for average pain and the worst pain of 6.0 (2.0) and 8.2 (2.1), respectively. The mean duration (SD) of acute pain was 17.6 (15.0) days. A total of 36.5% of the patients (n = 54/148) reported PHN, evaluated in patients with data available for up to at least 90 days following the onset of HZ symptoms. A total of 150 patients (98.7%) received a prescription for medications to control their HZ episode (Table 2) and acyclovir was the most common (n = 131; 85.1%).
Use of healthcare resources
Table 3 summarizes the UHCR reported by patients on follow up. Visits to a general practitioner (GP) were the most frequently used resource; 79.2% of the patients (n=122) re ported a mean (SD) of 2.6 (2.8) visits each. The proportion of patients who reported >1 visits to the emergency room or to a specialist was also high: 38.3% (n = 59; mean [SD]: 1.6 [1.0] visits) and 29.2% (n = 45; mean [SD]: 2.6 [3.1] visits), respectively. Overall, 14.3% (n=22) of the patients were hospitalized for their HZ episode, with a mean length of stay (SD) of 5.0 (4.7) days. Although the use of nursing services (n = 10; 6.5%) and psychotherapy/rehabilitation (n = 4; 2.6%) was infrequent, the mean (SD) number of services per user was high: 13.1 (27.5) and 21.0 (27.8), respectively.
Table 3 Use of healthcare resources related to HZ.
| Type of UHCR | Total cohort N = 154 | |
|---|---|---|
| N (%) | Mean (SD)1 | |
| General practitioner (GP) | 122 (79.2) | 2.6 (2.8) |
| Emergency room (ER) | 59 (38.3) | 1.6 (1.0) |
| Hospitalization | 22 (14.3) | 5.0 (4.7)2 |
| Nursing services | 10 (6.5) | 13.1 (27.5) |
| Physical therapist/rehabilitation | 6 (3.9) | 21.0 (27.8) |
| Psychiatry/psychologist/counselor | 4 (2.6) | 1.5 (0.6) |
| Specialist | 45 (29.2) | 2.6 (3.1) |
|
1 Number of healthcare contacts among users of the respective healthcare resources. 2 Number of inpatient days. | ||
Pain over time
Figure 1A shows HZ-related pain over time, evaluated us ing the ZBPI questions which assess "average pain" and the "worst pain in the last 24 hours" in patients with a pain score of 1 or more (0 represented no pain). The mean (SD) ZBPI average pain score peaked on day 7, 5.2 (2.2), and gradually decreased over time to 2.6 (1.7) on day 120. A slight increase was seen towards day 150 and day 180, which returned to an average score of 3.1 on both visits. A similar trend was seen for the ZBPI worst pain score, with an elevated score of 6.4 (2.4) reported on day 7, which decreased to 4.1 (2.3) on day 180, and increased slightly to 4.6 (2.4) and 5.0 (2.6) on days 150 and 180, respectively.
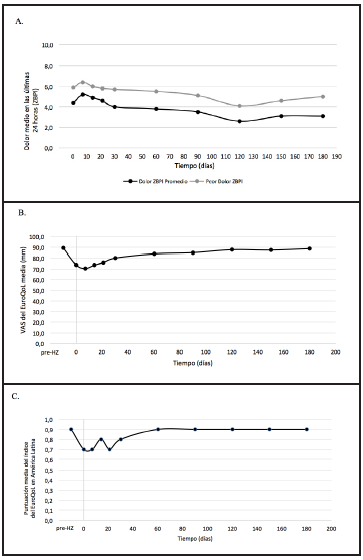
A. Average and worst HZ pain scores in the last 24 hours, over time. B. EuroQoL-5D VAS scores over time. C. EuroQoL-5D index score (Latin American weights) over time.
Burden of pain predictors were identified, calculated from the area under the curve of the "worst pain in the time since the onset of the HZ rash," based on the multivariate mixed model analyses (Table 4). In a reduced model, older age was found to be a significant positive predictor of the burden of pain (p<0.05) (Table 4); a "worst ZBPI pain since the onset of the HZ rash" score >7, assessed at enrollment, was also significantly related to a greater burden of pain than scores of 0-6 (p<0.001).
Table 4 Mixed model of repeated measures*: predictors of cumulative burden of pain.
| Predictor | Estimate | SD | 95% CI | P value |
|---|---|---|---|---|
| Age at onset of HZ symptoms, years | 3.85 | 1.93 | 0.03; 7.67 | 0.048 |
| Worst ZBPI pain score since the onset of the HZ rash: intense (>7) vs. mild/moderate (0-6) | 251.29 | 44.01 | 164.3; 338.2 | <0.001 |
| SD: standard deviation; CI: confidence interval; ZBPI: Zoster Brief Pain Inventory; HZ: herpes zoster. * Reduced model after retroactive selection of variables and adjustment for the time elapsed from the onset of symptoms at enrollment. The following variables were considered: time elapsed since the onset of HZ symptoms and age at that time: educational level; employment status; medications for HZ; number of lesions at enrollment; incident vs. prevalent HZ; time elapsed since the onset of symptoms at enrollment; worst prodromal and general pain scores. | ||||
Quality of life over time
Quality of life over time is presented in Figure 1B (EQ-5D VAS) and Figure 1C (EQ-5D index; Latin American weights). Regarding the first, the mean (SD) self-scored QL prior to HZ among the patients who answered was 89.3 (13.1), and it decreased to 73.7 (21.1) at the initial visit and to 70.5 (19.9) on day 7. Subsequently, constant increases were seen over time up to day 180, when a QL practically the same as that prior to HZ was reported: 88.6 (14.4) mm. The EQ-5D index score among patients who answered had a mean (SD) of 0.9 (0.2) prior to HZ, and decreased to 0.7 (0.2) both at the enrollment visit as well as on day 7. The QL index score prior to HZ of 0.9 (0.2) was once again reached on day 60 and remained constant to the end of the study.
Discussion
The clinical and economic burden of HZ has been pre viously studied in other Latin American regions 21-25; however, as far as we know, this is the first report on the burden of HZ in a Colombian context. In general, the find ings of this prospective, observational study indicate that the burden of HZ in Colombia is high, affects the quality of life, promotes the use of resources, and results in elevated rates of postherpetic, prodromal and acute pain. Given that 16.6% of the Colombian population is age 55 or older 26, this burden will continue to increase over time, unless adequate treatment strategies are implemented.
Although patients were recruited in different stages of their current HZ episodes, the UHCR during follow up was high; approximately 80% of the patients were seen by a general practitioner, and an additional 38 and 30% reported visiting the emergency room and specialists, respectively. This was seen despite the fact that treatment for the HZ episodes was prescribed for more than 98% of the patients, and coincides with the observed rates and intensity of HZ-related pain which are analyzed below. An interesting finding of this study was the use of topical acyclovir reported by more than 50% of the patients; since topical antiviral medications are not currently recommended for HZ treatment 2, this result reflects the actual treatment of HZ in Colombia, and may alert us to an unmet need in medical training and the understanding of treatment modalities aligned with best practices.
Overall, approximately 71% of the patients reported prodromal pain at enrollment, with reports of "pain since the onset of the rash" in more than 95% of the cases. In the worst cases, the pain was considered to be intense (aver age score ≥7), for both the prodromal as well as acute pain phases. Likewise, more than 36% of the patients reported PHN. This estimated PHN is in line with the 38.6% reported previously by Rampakakis et al. in a grouped analysis of Argentine, Mexican and Brazilian patients with HZ 23, although it is higher than the Mexican and Argentinian estimates of approximately 11% 24,25. The difference in observed rates of PHN may be attributed to the following: 1) for this study, more than 90% of the patients had preva lent HZ, which provided a longer time frame during which PHN could be captured, while the Argentinian estimate is for a sample which includes 40% incident cases; and 2) the Mexican incidence rate is based on data reported to the national health data system which provides epidemiological data only for hospital discharges.
Regarding the burden of pain (worst pain in the time elapsed since the onset of the HZ rash), the positive predic tors of increased burden found were advanced age and higher scores of the "worst pain on the ZBPI" since the onset of the HZ rash. These findings coincide with previous reports by Tsai et al. 27 and Drolet et al. 28 who evaluated the predictors of "seriousness of the disease" (equivalent to the burden of pain) in patients with HZ. Both studies reported a positive relationship between the seriousness of the disease, the oldest age group and higher worst pain scores on the ZBPI.
Likewise, and in line with the trend identified in the previous studies on HZ burden 22,25,27-30, increases in pain were accompanied by reductions in QL, measured by the EQ-5D. The average and worst "pain on the ZBPI in the last 24 hours" scores peaked on day 7, at 5.2 and 6.4, respectively, and the lowest EQ-5D VAS scores, of 70.5 mm, were seen at the same assessment time. The gradual improvement in pain scores over time showed concurrent increases in EQ-5D VAS scores on day 180, on which QL essentially reached the pre-HZ levels.
For the EQ-5D index scores, a negative impact on qual ity of life was also found, with a reduction from 0.9 in the period prior to HZ to 0.7 at the enrollment visit and on day 14, returning to the initial values by day 60. Slightly differ ent from this, a recent calculation in Costa Rica reported a reduction in EQ-5D index scores from 0.8 (prior to HZ) to 0.4 initially, without recovery of the pre-HZ QL at the end of the study (0.7 at day 180) 22. In contrast, while the EQ-5D index scores reported by the Argentine population with HZ were initially lower than those of the current study (0.6), they did reach the pre-HZ index scores by day 21, and exceeded them on day 120 25. These QL variations over time may be attributed to differences in pain scores between the studies: for Costa Rica, patients reported higher initial average and worst pain ZBPI scores of 6.6 and 7.7, respectively, with a reduction to 5.9 and 4.0 on day 180. However, the worst initial pain in Argentina was 5.5, it increased to 0.9 on day 60, and was 0.2 on day 180. This interpretation also supports the relationship between HZ pain and reduced QL.
This study has several limitations that should be con sidered. First, the study population only included patients 50 years old or older; given that the seriousness of the disease is known to increase with age, the exclusion of younger patients with HZ may have resulted in a selection bias favoring the recruitment of patients with slightly more advanced HZ. This selection bias is further aggravated by the fact that this study included patients who sought medical care for HZ, which may have resulted in an over-representation of more serious HZ cases than in the general population. Also, since laboratory confirmation of HZ was not required for patient inclusion, HZ classification errors may have occurred. In addition, the inclusion of prevalent cases may have led to a recall bias in the pain and QL evaluation before and after the onset of the rash. However, given that the mean (SD) of the time elapsed from the onset of the rash to being admitted to the study was only 21.3 (17.55) days, it may be supposed that the patients prob ably reported the HZ-related information accurately and, therefore, the risk of recall bias was reduced.
Despite these limitations, this study provides information on the burden of disease from HZ in a Colombian clinical context. The results not only indicate that the pain, UHCR and impact on QL of HZ are high, but also that advanced age and the time elapsed since the onset of symptoms are predictors of the burden of pain. As Colombian populations age, it is more important than ever to consider strategies for preventing HZ reactivation, such as the implementation of universal vaccination, or increased knowledge of HZ symptom recognition as well as pharmacological treatment options. The results of this study can be used to evaluate the economic burden of HZ in Colombia.

