











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Chloroquine is an antimalarial drug, but due to its immunomodulating effect, it is also useful in autoimmune diseases. It has few side effects, but renal complications have been reported. We describe the case of a patient with impaired renal function in whom phospholipidosis with podocyte zebra bodies was found on kidney biopsy. This finding initially oriented the diagnosis toward Fabry disease, but she did not have clinical signs and symptoms or a family history of the disease. Since the patient was female, genetic studies were ordered, which did not show alpha-galactosidase A (GLA) gene mutations, and the serum levels of alpha-galactosidase enzyme were normal. Due to the length of time she had been on chloroquine, and in the absence of clinical findings which would indicate another disease, she was diagnosed with chloroquine-induced renal phospholipidosis, a finding which has already been reported by other authors.
Case presentation
A 73-year-old woman from a city in Colombia, South America, was being followed by nephrology for chronic kidney disease (CKD) secondary to hypertensive nephrosclerosis. She had a 10-year history of rheumatoid arthritis (RA), long-standing hypertension, dyslipidemia, and severe osteoporosis with L2-L4 compression fractures, and was being treated with chloroquine, methotrexate, losartan, hydrochlorothiazide and atorvastatin. On her first nephrology consult, her laboratory tests showed creatinine at 1.67 mg/dL, and a CKD-EPI estimated glomerular filtration rate (GFR) of 26 mL/min, with the expected GFR for her age being 70 mL/min. The urine tests showed no protein, acellular sediment, and a 24-hour urine protein of 79.5 mg.
Three months later, rheumatology requested a repeat nephrology evaluation, with the following findings on the follow up tests: elevated creatinine at 2.01 mg/dL, with normal calcium and phosphorus, and low PTH. Anti-HIV, hepatitis B and hepatitis C antibodies were negative, C3 and C4 were not consumed, and protein electrophoresis did not have a monoclonal peak. Renal ultrasound reported mildly shrunken kidneys (explainable due to her age) with no corticomedullary differentiation disorders, and a normal renal artery Doppler. Since the source of the renal impairment was unclear, a percutaneous kidney biopsy was ordered.
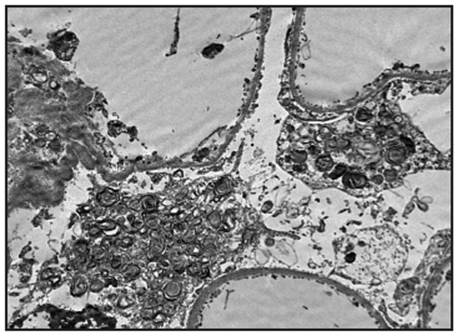
The biopsy report stated that 20 glomeruli were obtained; there was global sclerosis in five, with no mesangial or glomerular basement membrane abnormalities nor inflammatory changes in the glomeruli (Figures 1 and 2). There was 5% tubular atrophy, with no interstitial inflammation, myointimal thickening of the blood vessels and hyaline changes of the muscular wall with slight narrowing of the lumen (compatible with hypertensive nephrosclerosis). Immunofluorescence was negative for immune complex, complement (C3, C4, C1q), fibrin and light-chain immunoglobulin deposition. The main findings of electron microscopy or ultrastructural analysis were in the podocytes, with a loss of pedicels (their feet) in 70% of the capillary surface, and numerous zebra or lamellar bodies corresponding to lysosomal inclusions within them (Figures 3 and 4).
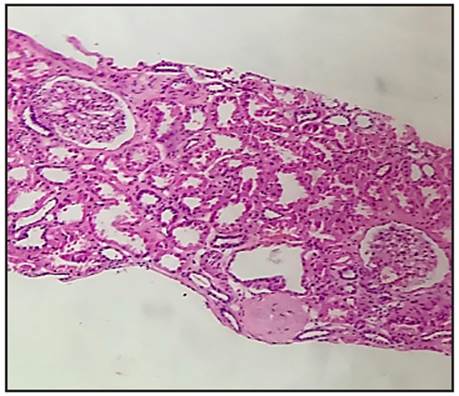
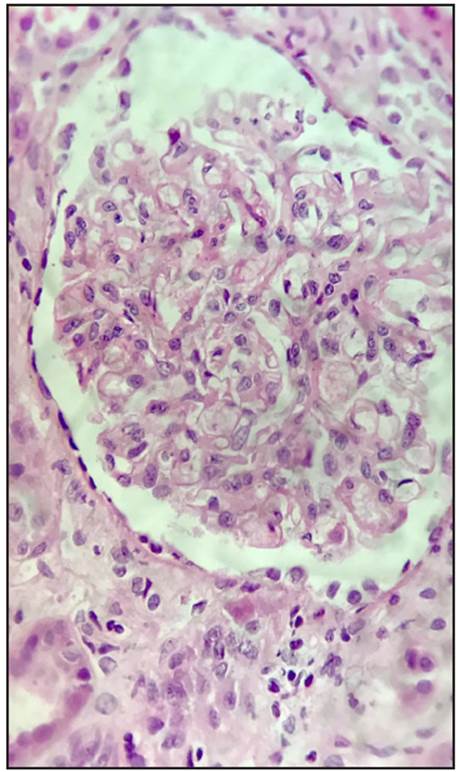
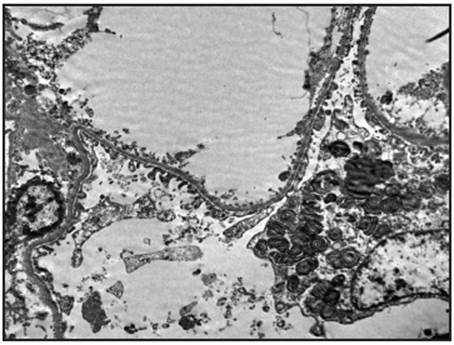
Figure 3 Electron or ultrastructure microscopy: Podocytes with multiple "Zebra Bodies" corresponding to cytoplasmic phospholipids.
In light of the histological findings, the first diagnostic possibility proposed was Fabry disease. Since she was female, sequence analysis was ordered for her and her daughters to determine if there were mutations of the gene coding for the alpha galactosidase (GLA) enzyme. No pathogenic findings suggestive of Fabry disease were found in the patient nor her daughters in this study. The serum alpha-galactosidase A levels reported were 7.5 nmol/mL/ hour (normal controls 2.0 to 21.8 nmol/mL/hour), concluding that she did not have Fabry disease. Since there were no clinical findings suggestive of other diseases which would explain the histological findings, it was concluded that this was drug-induced phospholipidosis and, of the medications the patient was taking, the only possibility was chloroquine, which she had been taking for many years, reaching a cumulative dose of 810 grams.
Three months after the biopsy, the patient was seen by rheumatology as an outpatient and showed general deterioration. She had lost four kilograms of weight and had hyporexia, dysphagia for solids and liquids, muscular atrophy, marked difficulty walking, herpes zoster-like lesions on the chest, leukopenia and further renal function impairment. She was hospitalized and another nephrology consult was requested.
On her new tests, the creatinine had risen to 8.18 mg/ dL, the CKD-EPI estimated GFR was 4 mL/min, 24-hour proteinuria was 390 mg, the urine test showed 75 mg/dL of protein, and the urine sediment included three eumorphic red blood cells per high-power field. Acute interstitial nephritis was suspected, but steroids or cytostatic agents were not begun due to her herpes zoster and the risk of viral systemic complications. Nephrology confirmed that she was still receiving 250 mg of chloroquine from Monday through Friday, which they discontinued along with the proton pump inhibitor (esomeprazole), adjusting the prescribed dose of acyclovir to her glomerular filtration rate. With these measures and hydration, her creatinine decreased to 5.0 mg/dL.
Due to her neuromuscular symptoms, a simple brain magnetic resonance was ordered which was reported as normal. Upper GI endoscopy showed a giant hiatal hernia. Chloroquine-induced myopathy was suspected, and electromyography plus nerve conduction was ordered. The patient developed marked dyspnea, requiring oxygen therapy due to desaturation, and an acute pulmonary thromboembolism was suspected. A transthoracic echocardiogram detected a slight decrease in the ejection fraction, which was still preserved (58%), and a slight increase in pulmonary systolic arterial pressure, but with no signs of right ventricular dysfunction. A chest CAT reported multiple segmental parenchymal opacities probably related to multilobar opportunistic pneumonia.
The patient deteriorated rapidly and neither she nor her family accepted a transfer to the intensive care unit or advanced measures like orotracheal intubation; she therefore remained on the general ward and died. The family also refused an autopsy.
Discussion
The renal complications which accompany rheumatoid arthritis may be triggered by poor disease control or be related to its pharmacological treatment 1. In our case report, the kidney biopsy mainly reported podocyte involvement with pedicel loss in 70% of the capillary surface, and numerous zebra or lamellar bodies corresponding to lysosomal inclusions. The diagnosis was renal lipidosis, a group of diseases characterized by abnormal lipid storage in the kidney. They are classified as primary when there are specific hereditary enzyme deficits, or secondary to other disorders such as liver cirrhosis, nephrotic syndrome, Alport syndrome, Alagille syndrome, or even toxic agents or medications, the latter being known as drug-induced phospholipidosis (DIP) 2-5.
Drug-induced phospholipidosis due to antimalarial medications like chloroquine or hydroxychloroquine (HCQ) has been rarely described, always in the context of autoimmune diseases like Sjögren syndrome, systemic lupus erythematosus (SLE), RA and connective tissue disease, rather than in malaria treatment, possibly due its short treatment course in which the cumulative dose is small. To date, 12 cases of chloroquine and HCQ-induced phospholipidosis have been reported (Table 1), as well as one case in a renal transplant patient with underlying SLE, in whom graft rejection was suspected due to kidney function impairment, but phospholipidosis was found on the kidney biopsy, requiring hydroxychloroquine withdrawal, with resulting improvement 3-4,6-16.
Table 1 Case reports to date of chloroquine and hydroxychloroquine-induced renal phospholipidosis.
| Case | Medical history | Medication Dose | Renal manifestation and general symptoms | Creatinine GFR | Biopsy result | Genetic/ Enzymatic analysis | Treatment | Effect of treatment Efecto del tratamiento |
|---|---|---|---|---|---|---|---|---|
| 13 Female 56 years | Polyarthritis | NSAIDs, steroids, gold salts, methotrexate, HCQ | Proteinuria 3,384 mg/ day; Arthralgias of the knee, ankles, hands | GFR 73.1 mL/ min Creatinine 1.3 mg/dL | Acute tubular lesion. Electron microscopy shows electrondense bodies bound to the membrane with the characteristic multilamellar appearance of zebra bodies in the glomerular epithelial cells, mesangial cells, glomerular endothelial cells, interstitial cells, tubular epithelial cells, and vascular endothelium. | Normal levels of galactosidase, with no GLA gene mutation | HCQ discontinued, ACE inhibitors begun | Decreased proteinuria and creatinine. |
| 24 Female 28 years | SLE | Captopril, HCTZ, prednisone HCQ 400 mg/ day. 14 months 168 gr | Proteinuria (600 mg/ day), fever, erythema, photosensitivity, asthenia | CKD-EPI GFR 116 mL/min/1.73 m2 | Elecgtron microscopy: osmiophilic lamellar intralysosomal inclusions in the podo-cytes resembling "zebra bodies." | Neither galactosidase nor genetics were measured | HCQ was discontinued in favor of thalidomide | No proteinuria. A second kidney biopsy showed cytoplasmic edema in the podocytes, with no lipid deposits. |
| 36 Female 56 years | Rheumatoid arthritis | Celecoxib, Chloroquine minimum of 75 cumulative grams | Increased creatinine, proteinuria, hematuria. Edemas, muscle weakness. | Cr 2.2 mg/dL GFR 23 mL/min/1.73 m2 | Visceral epithelial cells showing spiral lipid inclusions, some capillaries with vacuolated cytoplasm and some small granular deposits | Normal levels with no genetic mutations | Chloroquine discontinued | After one year, she returned to her baseline kidney function, proteinuria and hematuria ceased, and she had no edemas or muscular symptoms. |
| 47 Female 51 years | Sjogren syndrome | Prednisone, Methotrexate HCQ 300 mg/ day 1.8 cumulative g | Increased creatinine, neck and lumbosacral pain | Cr 1.45 mg/dL | Granular and vacuolar degeneration and formation of protein cylinders in the tubular epithelial cells. Interstitial fibrosis and infiltration with numerous inflammatory cells. Electron Microscopy: lamellar bodies in some podocytes. | No GLA gene mutation. | HCQ discontinued | Restored kidney function |
| 58 Female 41 years | Undifferentiated connective tissue disease | HCQ 400 mg/ day 288 cumulative g | Proteinuria 1,120 mg/day, hematuria, weight loss, weakness | GFR 119 mL/min/1.73 m2 Creatinine 0.66 mg/dL | Granular degeneration of tubular epithelial cells without evident atrophy, edematous glomerular epithelial cells vacuoles in the podocytes with dense lamellar structures | No genetic mutations | HCQ discontinued | Decreased proteinuria and hematuria |
| 69 Female 36 years | SLE Class V lupus nephritis | HCQ 400 mg/ day (1,412 cumulative grams over 9 years) Steroid, ritux-imab | Non-nephrotic proteinuria, without hematuria or kidney function abnormalities | Not reported | Unusual cytoplasmic vacuolization of the podocytes, extramembranous granular deposits containing IgG, C3, kappa and lambda, osmiophilic lamellar and concentric inclusions in the podocytes corresponding to "Zebra bodies" | No GLA gene mutation, Normal galactosidase levels | HCQ discontinued | The patient developed nephrotic syndrome associated with SLE membranous nephropathy; she received rituximab |
| 710 Female 14 years | SLE; Hashimoto's thyroiditis | Prednisolone, azathioprine HCQ 500 mg/day | Non-nephrotic proteinuria, low-grade fever, cheek rash, proximal muscle weakness, atrophy, bilateral knee and ankle edema | Not reported | Electron Microscopy: numerous zebra bodies, mainly located in the podocyte cytoplasm, associated with mesangial dense deposits | No GLA gene mutation, normal galactosidase levels | HCQ discontinued | Proteinuria resolved, muscle function improved |
| 811 Female 27 years | SLE | HCQ, azathioprine, prednisone | Proteinuria/creatinuria ratio 0.4-3.8 g/g, pyuria | GFR 119 mL/min/1.73 m2 | Mesangial proliferative lupus nephropathy and membranous nephropathy (Class II/V). Electron Microscopy: subepithelial dense deposits and "zebra body" lamellar inclusions in the podocytes. | No genetic mutation | Not mentioned | Not mentioned |
| 912 Female 31 years | SLE | HCQ 150 mg/day 219 cumulative g | Proteinuria 600 mg/ day, increased skin lesions, corneal lesions | Cr 0.9 mg/dL | Visceral epithelial cells with vacuolated cytoplasm, dense bodies with a multilamel-lar appearance and characteristic myelin figure or zebra body changes, also found in smaller amounts in the glomerular endothelium and vascular smooth muscle. Expansion of the mesangial matrix and IgA, IgM, IgG, and C3 mesangial and focal subendothelial immune dense deposits (class II lupus nephritis) | Normal levels, with no genetic mutations | Chloroquine discontinued | Six months later the skin lesions had decreased, the kidney function was unchanged, proteinuria had decreased and the subepithelial corneal lesions had disappeared |
| 1013 Female 70 years | SLE, HTN, DVTTVO | Steroid, methotrexate, HCQ | Impaired kidney function, proteinuria, small left kidney. Corneal deposits | Cr 1.28 mg/dL GFR 64 mL/min 2 gr proteinuria | Arterionephrosclerosis and arteriolar hyalinosis compatible with hypertensive kidney disease without signs of lupus nephritis. Foamy inlusions within the podocytes and tubular epithelial cells. Intracellular osmio-philic myelin body ("zebra body") deposits | Normal levels, with no genetic mutations | HCQ discontinued | The creatinine clearance remained stable, proteinuria was maintained at 1.5-5 gr |
| 1114 Female 30 years | SLE | Steroid HCQ 340 g | Nephrotic syndrome, hematuria, leukocyturia, kidney function impairment, increased arthralgias, cardiomyopathy | Cr 1.05 mg/dL 3.5 gr in 24 hours | Mesangial proliferation, irregular endothelial cell proliferation, neutrophilic cells, focal fibrosis in the interstitium, mesangial IgG, IgA, and C3 deposits, class III lupus nephritis. Endothelial cells from the glomeruli and the vessels showed myelin-like figures, identical to lamellar bodies (zebra bodies) | Normal galactosidase levels, a genetic study was not performed as it was not available | HCQ discontinued | Normal echocardiogram, urinalysis showing trace proteins |
| 1215 Female 46 years | Sjögren syndrome, osteoporosis, HTN | Steroids, hydroxychloroquine 51 cumulative grams | Increased creatinine, non-nephrotic proteinuria | Initial GFR 23 mL/min 11-month GFR 8 mL/min Cr 5.0 | Electron microscopy: showed a large quantity of osmiophilic lamellar bodies, especially in the podocytes. Small quantities of curvilinear elements. A smaller quantity of these lamellar bodies were found in vascular smooth muscle, endothelial cells and the tubular system | Normal galactosidase levels | HCQ discontinued | Restored kidney function (9 months) |
In the reported studies, all the cases occurred in women with ages ranging from 14-70 years, 10 of whom were on HCQ, with the most common disease being SLE. The cumulative doses of the two patients who were on chloroquine were 75 and 51 grams, while in our case it was close to 810 grams 3,4,6-15.
The predominant site of lipid accumulation can guide the clinician in the differential diagnosis of the diseases which cause it. Deposition mainly in the podocytes, with lysosomal inclusions, is found in Fabry disease, nephrosialidosis, GM1 gangliosidosis, type 2 mucolipidosis, Hurler syndrome, Niemann-Pick disease and Farber disease. Renal tubular cell involvement occurs in metachromatic leukodystrophy, adult Refsum disease, and Sandhoff disease. Accumulations in mesangial and glomerular endothelial cells are found in lecithin cholesterol acyltransferase deficiency, Gaucher disease and Niemann Pick disease 2,3,4. Zebra or myeloid bodies in the podocytes are more characteristic of Fabry disease. They have occasionally been described in Niemann Pick; however, this disease also has glomerular and mesangial endothelial damage and large vacuolated cells known as Niemann Pick cells 2-4.
In Fabry disease, despite being an X-linked disorder, heterozygous women may develop systemic organ involvement. In our patient, the lack of other clinical findings, normal enzyme levels and lack of genetic mutations ruled out this diagnosis, with the most probable diagnosis being drug-induced phospholipidosis, in this case caused be chloroquine 17-19.
Drug-induced phospholipidosis is a condition in which some cationic drugs with lysosomal affinity can easily enter this organelle and form a drug-phospholipid complex with subsequent accumulation, aided by lysosomal enzyme activity inhibition and resistance to digestion due to increased lysosomal pH. The reversible inhibition of lysosomal phospholipases A and C is thought to be dose dependent 20. Some drugs with a documented ability to cause DIP include chloroquine, hydroxychloroquine, amiodarone, azithromycin, gentamicin, fluoxetine, sertraline and clozapine 21.
Histopathological findings have been used to try to distinguish Fabry disease from DIP. The presence of curvilinear bodies (microtubular structures in vascular smooth muscle cells and podocytes) and small, round granular inclusions in the mitochondria of mesangial, tubular, and endothelial cells may favor DIP. Meanwhile, a greater number of intra-lysosomal inclusions are found in Fabry disease. 5.
During the patient's final hospitalization, when she was still receiving chloroquine, important developments included neurological and muscular involvement, worsening kidney function and the onset of proteinuria without significant urine sediment findings. The cumulative dose of chloroquine was greater, and the fact that her kidney function improved when it was discontinued suggests exacerbated chronic kidney disease, and worsening podocytopathy evidenced by proteinuria, events which could be explained by chloroquine toxicity 22. Several case reports have described a similar behavior 3,8.
The patient also exhibited dysphagia and symmetrical proximal muscle weakness symptoms, with marked difficulty in walking. Chloroquine toxicity has been reported to cause neuromyopathy and myopathy, as it can accumulate in these tissues; thus, in this case, the patient may have developed chloroquine-induced myopathy 6,20,23,24,25. These findings have been reported to improve when the medication is discontinued 26, and with a prevalence of 6.7% and incidence of 1.2%, it is not such a rare condition 27.
Conclusion
We report a patient being treated with chloroquine for an approximately 10-year history of rheumatoid arthritis, with a significant cumulative dose, who developed progressive deterioration of her kidney function, non-nephrotic-range proteinuria and proximal muscle weakness in the extremities. The kidney biopsy showed zebra bodies in the podocytes. Fabry disease was ruled out. The final diagnosis was drug-induced phospholipidosis, in this case caused by chloroquine. This case report reminds us of the importance of being aware of the possible side effects of medications.

