











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Intensive care units (ICUs) have changed the overall focus of various diseases, increasing the treatment pos sibilities and decreasing the associated mortality and comorbidity. One of the diseases with the greatest change over the last few years has been acute kidney injury (AKI) with the need for renal replacement therapy (RRT). It is estimated that up to 21.6% of patients admitted to the hospital have AKI, with 10% of these cases requiring RRT 1. Wald et al. reported an increased incidence of acute kidney injury with the need for RRT comparing the five-year periods of 1996-2000 and 2006-2010, at 0.8% and 3.0%, respectively, with the 90-day need for chronic RRT at 25% in ICU patients 2.
Anywhere from 13-78% of AKI cases in the ICU have medical causes, and surgical conditions account for 16 to 30% of the cases 3, with 5.6% of all of these requiring RRT. The 28, 90 and 365-day mortality in this context is 51, 60 and 64%, respectively 4, with wide variances between studies 5. Furthermore, kidney function and the need for chronic dialysis have been the focus of ongoing research. Wald et al. reported that, in 21,234 patients, 90-day RRT dependence was 27.2% 2.
Many factors are associated with the clinical outcomes and a predisposition to needing dialysis in the ICU. The most frequently reported factors are high blood pressure, diabetes, heart failure, chronic kidney disease 6,7, and the chronic use of medications such as acetylsalicylic acid (ASA), angiotensin-converting enzyme (ACE) inhibitors/angiotensin II receptor blockers (ARBs), diuretics, non-steroidal anti-inflammatory drugs (NSAIDs), and proton pump inhibitors (PPIs) 8,9. The type of RRT and timing of its initiation are also included, with a substantial dispar ity in the results of different studies in this regard 10.
Moreover, there are different definitions of kidney recovery, specifically in this type of patient, based on dif ferent creatinine or glomerular filtration rate (GFR) cut-off points 11. Pannu et al. showed that a greater than 25% deterioration in kidney function from the baseline GFR is the point at which the risk of other outcomes such as death and the need for chronic RRT increases 12, this being the starting point for evaluating the composite outcome of major adverse kidney events (MAKE) in patients with AKI13. The objective of the current study was to determine the clinical outcomes of patients needing acute dialysis using MAKE assessment in 90-day and one-year follow-up.
Materials and methods
Study design
A single-center, longitudinal, analytical study with a retrospective cohort was carried out at a tertiary care hos pital (Hospital Departamental Universitario Santa Sofía de Caldas) in the city of Manizales, Caldas, Colombia, including all patients requiring renal replacement therapy exclusively due to AKI, according to the Clinical Practice Guidelines for Acute Kidney Injury (KDIGO) criteria14, with 90-day and one-year follow up. This study was approved by the ethics committee of the health sciences department at Universidad de Caldas, and the ethics com mittee of Hospital Departamental Universitario Santa Sofía de Caldas.
The clinical charts of all patients who were admitted to the hospital's ICU and required RRT between 2006 and 2018 were reviewed. The clinical charts were selected using the institution's Hosvital® software, which allows selection by institutional units and, within the units, a key word search using terms like «dialysis,» «hemodialyis,» «renal replacement therapy,» and «hemodiafiltration,» to select patients who received RRT. The primary outcome was the occurrence of the MAKE compound outcome composed of death, partial kidney function recovery (un derstood as a creatinine level more than 25% higher than the baseline creatinine, with no RRT requirement) and the need for dialysis at 90 days and one year>s follow up. The secondary outcomes included the MAKE components analyzed separately during the same follow up periods.
Patients
The inclusion criteria were: patients over the age of 18 who were admitted to the ICU from 2006 to 2018, AKI with the need for RRT, and a creatinine report recorded in the institution's computerized clinical chart within the last year. For patients without a record of the last creatinine, the first creatinine taken on admission was used, as long as the RRT was not begun less than 48 hours after draw ing this lab. Exclusion criteria: need for RRT in the year prior to hospitalization, kidney transplants, prior GFR <30 mL/min/m2 BS by MDRD, and no reported creatinine at 90 days or one year.
Variables
Sociodemographic and anthropometric variables, as well as medical history, prior use of medications associ ated with AKI (ACE inhibitors, ARBs, ASA, diuretics, PPIs, and NSAIDs), the etiology of the AKI and need for RRT (hypovolemic shock, cardiogenic shock, septic shock, obstructive uropathy, cardiovascular surgery or other etiologies), type of therapy (continuous/intermittent therapy), and timing of treatment initiation (early initia tion understood to be RRT in a patient with KDIGO 3 AKI without emergency dialysis criteria: hypercalcemia greater than 6.5 mEq/L with abnormal electrocardiographic find ings, diuretic-resistant fluid overload/anasarca or pulmo nary edema, metabolic acidosis, uremic encephalopathy, persistent anuria and uremia; or late initiation understood as KDIGO 3 AKI with any of the previously mentioned criteria for emergency dialysis) were analyzed. The severity of the patient's clinical condition was also considered using the APACHE II score, delirium and days of hospital stay. For renal function, baseline creatinine and GFR estimated by the MDRD formula were used. In addition, a creatinine sample was taken and the GFR was estimated at 90 days and one year, recorded in the institution's medical chart and verifying the presence or absence of chronic RRT or a record of death in the mentioned periods.
Statistical analysis
The analysis of the collected data was performed using SPSS version 21 statistical software. Categorical variables were described using absolute and relative frequencies. The Kolmogorov-Smirnov test was used to determine the normal or asymmetric distribution of quantitative variables. Measures of central tendency and dispersion were used, such as mean and standard deviation (SD) for variables with a normal distribution, and median and interquartile range (IQR) for variables with asymmetric distribution. Chi-square was used to evaluate the association between qualitative variables, and then a comparison of means of the dichotomous quantitative variables was conducted using the Mann Whitney U test for asymmetric variables and Student's t-test for those with a normal distribution. P values <0.05 were considered to be significant. Survival was assessed by the Kaplan-Meier method, using log rank to detect significant differences between the groups of interest evaluated. A logistic regression model was run, calculating the OR to evaluate predictors of MAKE (at 90 days and one year) and individual mortality.
Results
Patient selection and general characteristics
A total of 252 clinical charts of patients who received RRT from 2006 to 2018 were found. Eighty-six patients were excluded due to having begun RRT prior to being admitted to the ICU, 39 due to being admitted to the institution needing emergency dialysis without a prior creatinine report, and five due to not having GFR follow up at one year. A total of 122 patients were included in the study. Table 1 summarizes the patients' characteristics.
Table 1 General patient characteristics.
| Variable | n=122 |
|---|---|
| Sex | |
| Male | 81 (66.3) |
| Female | 41 (33.6) |
| Age, median (IQR) | 60 (42-71) |
| Weight, median (IQR) | 60 (55-70) |
| Baseline creatinine, mean in mg/dL (SD) | 1.1 (0.4) |
| Baseline GFR, median mL/min/m2 (IQR) | 75.7 (51-101.8) |
| History of diabetes, n (%) | 19 (15.5) |
| History of heart failure, n (%) | 23 (18.8) |
| History of HTN, n (%) | 52 (42.6) |
| Prior use of ASA, n (%) | 23 (18.8) |
| Prior use of ACE inhibitors/ARBs, n (%) | 38 (31.1) |
| Prior use of diuretics, n (%) | 28 (22.9) |
| Prior use of NSAIDs, n (%) | 7 (5.7) |
| Prior use of PPIs, n (%) | 16(13.1) |
| Delirium, n (%) | 47 (38.5) |
| APACHE II score on admission, median (IQR) | 22 (17-27) |
| Days of hospital stay, median (IQR) | 28.5 (10-54) |
| Etiology | |
| Septic shock n (%) | 79 (64.7) |
| Carcinogenic shock n (%) | 34 (27.8) |
| Obstructive uropathy n (%) | 3 (2.4) |
| Cardiovascular surgery n (%) | 15 (12.2) |
| Hypovolemic shock n (%) | 10 (8.1) |
| Other etiology | 12 (9.8) |
| Therapy modality | |
| Continuous therapy, n (%) | 85 (69.6) |
| Intermittent therapy, n (%) | 38 (31.1) |
| Timing of RRT | |
| Early initiation, n (%) | 34 (27.8) |
| Late initiation, n (%) | 88 (72.1) |
| Criteria for initiating late therapy | |
| Anuria n (%) | 34 (27.8) |
| Metabolic acidosis n (%) | 57 (46.7) |
| Oliguria n (%) | 9 (7.3) |
| Hypercalcemia n (%) | 13 (10.6) |
| Uremia n (%) | 14 (11.4) |
| Fluid overload n (%) | 26 (21.3) |
| Uremic encephalopathy n (%) | 1 (0.8) |
| HTN: Hypertension, ACE inhibitors: Angiotensin converting enzyme inhibitors, ARBs: angiotensin II receptor blockers, NSAIDs: non-steroidal anti-inflammatory drugs, PPIs: proton pump inhibitors, GFR: glomerular filtration rate. RRT: renal replacement therapy. APACHE II: Acute Physiology And Chronic Health Evaluation IQR: interquartile range, SD: standard deviation. | |
Primary outcome
An evaluation of MAKE at 90 days showed that it was associated with a history of diabetes, a higher APACHE II score, anuria, acidosis, and the timing of RRT initiation (a greater percentage of patients in the late initiation group developed MAKE). In the one-year analysis, the therapy modality was added to the mentioned variables (a greater percentage of patients in the continuous therapy group), as shown in Table 2. No associations were found with the kidney stage on admission or other variables.
Table 2 MAKE compound outcome at 90 days and one year and associated variables.
| Variable | MAKE 90 DAYS | MAKE 1 YEAR | ||||
|---|---|---|---|---|---|---|
| Absent, n=28 | Present, n=94 | P value | Absent, n=29 | Present, n=93 | P value | |
| Hisory of diabetes, n (%) | 3.6 | 19.1 | 0.046* | 0 | 20.4 | 0.008* |
| APACHE, median (IQR) | 19.5 (15-23) | 23 (17-28) | 0.036* | 19 (15-23) | 23 (17-28) | 0.036* |
| Days of hospital stay, median (IQR) | 63 (49-80.5) | 19.5 (9-39) | 0.000* | 62 (48-81) | 19 (9-36) | 0.000* |
| Baseline creatinine, mean (SD) | 1.0 (0.4) | 1.1 (0.4) | 0.468 | 1.0 (0.4) | 1.1 (0.4) | 0.734 |
| Baseline eGFR, median (IQR) | 86.9 (64 101.8) | 74 (48.7 101.4) | 0.178 | 86.6 (62.8 98.5) | 74.6 (48.8 102.5) | 0.322 |
| Type of therapy | ||||||
| Continuous therapy, n (%) | 18.8 | 81.2 | 0.1 | 17.6 | 82.4 | 0.016* |
| Intermittent therapy, n (%) | 31.6 | 68.4 | 0.127 | 36.8 | 63.2 | 0.23* |
| Timing of initiation | ||||||
| Early initiation, n (%) | 38.2 | 61.8 | 0.013* | 38.2 | 61.8 | 0.020* |
| Late initiation n (%) | 17 | 83 | 0.013* | 18.2 | 81.8 | 0.020* |
| Criteria for initiation | ||||||
| Anuria, n (%) | 7.1 | 34 | 0.005* | 6.9 | 34.4 | 0.004* |
| Acidosis, n (%) | 21.4 | 54.3 | 0.002* | 24.1 | 53.8 | 0.005* |
| APACHE II: Acute Physiology And Chronic Health Evaluation. HTN: Hypertension. MAKE: major adverse kidney events. eGFR: estimated glomerular filtration rate. IQR: interquartile range, SD: standard deviation. | ||||||
Secondary outcomes
At the 90-day follow up, an association was found between dialysis dependence and a history of high blood pressure, obstructive uropathy, NSAIDs, metabolic acidosis, hypercalcemia, anuria and uremic encephalopathy, with a persistent association at one year with NSAIDs, metabolic acidosis, anuria and uremic encephalopathy (Table 3). At 12 months, an analysis of renal outcomes according to the chronic kidney disease stage on admission showed that 65.6% of the patients were in stage 2 or better, 18.9% in 3a and 15.6% in 3b. Altogether, 64.2% of the cases fully recovered kidney function, 45.2% of whom were in stage 2 on admission. An association was found between the kidney stage on admission and the renal outcomes after 12 months (p=0.000), mainly showing a greater dependence on dialysis for patients with GFR in stage.
Table 3 Renal results of surviving patients at 90 days and one year.
| Variable | 90-day survivors | One-year survivors | ||||||
|---|---|---|---|---|---|---|---|---|
| Full recovery (n=21) | Partial recovery (n=7) | Dialysis (n=4) | P value | Full recover (n=21) | Partial recover (n=7) | Dialysis (n=3) | P value | |
| History of HTN, n (%) | 38.1 | 14.3 | 100 | 0.049* | 33.3 | 42.9 | 100 | 0.188 |
| Use of NSAIDs, n (%) | 0 | 0 | 50 | 0.001* | 0 | 0 | 66.7 | 0.000* |
| Obstructive uropathy, n (%) | 0 | 0 | 25 | 0.027* | 0 | 14.3 | 0 | 0.194 |
| Baseline eGFR, median, (IQR) | 75.6 (38.6 12.8) | 128.3 (87 174.5) | 53.7(31.6 -98.5) | 0.001* | 85.3 (55.9 93.3) | 98.5 (86.2 134.8) | 40.4 (31.6 44.2) | 0.010* |
| Type of therapy | ||||||||
| Continuous therapy, n (%) | 81.3 | 18.8 | 0 | 0.069 | 80 | 20 | 0 | 0.170 |
| Intermittent therapy, n (%) | 50 | 25 | 25 | 0.069 | 56.30 | 25 | 18.8 | 0.170 |
| Timing of RRT initiation | ||||||||
| Early initiation, n (%) | 69.2 | 30.8 | 0 | 0.168 | 62.9 | 30.8 | 0 | 0.242 |
| Late initiation, n (%) | 63.2 | 15.8 | 21.1 | 0.168 | 66.7 | 16.7 | 16.7 | 0.242 |
| Criterion for initiation | ||||||||
| Anuria, n (%) | 9.5 | 0 | 0 | 0.015* | 9.5 | 0 | 0 | 0.020* |
| Acidosis, n (%) | 28.6 | 0 | 100 | 0.002* | 23.8 | 28.6 | 100 | 0.022* |
| Hypercalcemia, n (%) | 4.8 | 28.6 | 50 | 0.019* | 9.5 | 14.3 | 33.3 | 0.615 |
| Uremic encephalopathy, n (%) | 0 | 0 | 25 | 0.000* | 0 | 0 | 33.3 | 0.000* |
| NSAIDs: non-steroidal anti-inflammatory drugs. APACHEII: Acute Physiology And Chronic Health Evaluation. ARBs: angtiotensin II receptor blockers. HTN: Hypertension, ACE inhibi tors: Angiotensin converting enzyme inhibitors. eGFR: estimated glomerular filtration rate. IQR: interquartile range, SD: standard deviation. | ||||||||
Inpatient mortality was 73.7% (90 patients). Thirty-two patients had survived at 90 days, and 31 at 12 months. An as sociation was found between one-year mortality and a higher APACHE II score, diabetes, and the type and timing of RRT initiation, with a greater percentage of deaths in continuous and late-initiating therapy, and in the presence of anuria. A Kaplan-Meier analysis was performed comparing mortality according to timing of initiation and type of therapy, with statistically significant differences found (Figures 1 and 2).
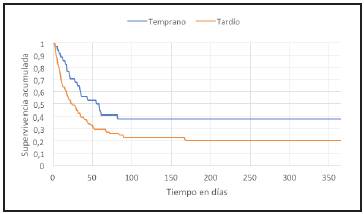
Figure 1 Graph of 12-month survival using the Kaplan-Meier method by treatment modality (p=0.000 by log rank).
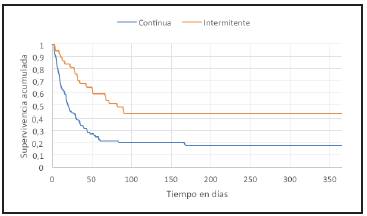
Figure 2 Graph of 12-month survival using the Kaplan-Meier method by timing of treatment (p=0.027 by log rank).
A logistic regression analysis was performed with the variables associated with MAKE outcomes at 90 days and one year, and mortality at one year, finding that patients who developed MAKE at 90 days were more likely to have initiated therapy late, and to have had anuria and metabolic acidosis. There were similar results in the one-year follow up of MAKE and the mortality analysis, where continuous therapy was added (Table 4). The severity of the clinical condition on admission was evaluated according to the APACHE II score between therapy modalities and the timing of initiation variables, with no differences found for either comparison (p=0.836 between intermittent vs. continuous RRT, and p=0.808 between early vs. late RRT).
Table 4 Multivariate analysis using logistic regression.
| Variable | OR | 95% CI |
|---|---|---|
| 90-day MAKE | ||
| Early initiation | 0.332 | 0.137-0.806* |
| Late initiation | 3.013 | 1.241-7.316* |
| Anuria | 6.71 | 1.497-30.076* |
| Metabolic acidosis | 4.349 | 1.616-11.7* |
| Diabetes | 6.39 | 0.814-50.222 |
| One-year MAKE | ||
| Early initiation | 0.359 | 0.149-0.864* |
| Late initiation | 2.786 | 1.157-6.706* |
| Continuous therapy | 2.841 | 1.193-6.763* |
| Intermittent therapy | 0.373 | 0.157-0.884* |
| Anuria | 7.082 | 1.582-31.697* |
| Metabolic acidosis | 3.654 | 1.423-9.385* |
| Death at one year | ||
| Early initiation | 0.415 | 0.175-0.986* |
| Late initiation | 2.407 | 1.015-5.713* |
| Continuous therapy | 3.556 | 1.509-8.375* |
| Intermittent therapy | 0.299 | 0.127-0.701* |
| Anuria | 7.86 | 1.76-35.10* |
| MAKE: major adverse kidney events | ||
Discussion
This study found a relationship between the compound outcome of MAKE and diabetes, APACHE II, timing of RRT initiation and anuria at 90 days and one year, when the modality of RRT was added, with similar results on the logistic regression. In addition, arterial hypertension, NSAIDs, obstructive uropathy, anuria, metabolic acidosis, hypercalcemia and uremic encephalopathy were associated with chronic RRT therapy at 90 days, with an association with NSAIDs, anuria, metabolic acidosis and uremic en cephalopathy persisting at one year.
The results evidence the complexity and worse prognosis of patients who require RRT due to AKI in the ICU. Inpatient mortality was 73.77% at 90 days and 74.5% at one year. Compared with other studies reporting mortality between 41 and 65%, ours had greater inpatient mortality. However, we had a lower mortality between the follow up periods 15-19, also associated with the severity of the clinical condition. Other authors described an association with a positive fluid balance, metabolic acidosis, late initiation of therapy and continuous therapy, similar to the findings of this study, although they did not maintain these findings in the multivariate analysis 15. There are likely to be differences in mortality, mainly related to sociodemographic variables, given the origin of the patients admitted to our institution, compared with international studies.
One of the important points in this study is the evalu ation of the MAKE compound outcome, which in recent years has been proposed as the best way to characterize the results in patients with AKI. Few studies have evaluated this outcome in the ICU. De Corte et al. 15 analyzed MAKE in 1,292 patients, 86 and 87.5% of whom developed this outcome at 90 days and one year of follow up, respectively, these being higher results than those of our study (77.04% for MAKE at 90 days and 76.22% for MAKE at one year). The most significant associations included kidney stage 3 on ICU admission, oligo/anuria, and the severity of the clinical condition on admission 15, similar to our study. M. Meersch et al. followed the patients who participated in the ELAIN study, with MAKE analysis at the 12 month follow up, finding that 64.9% of the patients who received early therapy developed MAKE at one year compared with 89.1% of the patients who began therapy late 20. Although there is some concordance with our findings, the differences in the definition of the timing of therapy should be noted. The STARRT-AKI study evaluated the results of early vs. late implementation of RRT, with secondary analysis of the MAKE components at 90 days, finding no differences 21. As can be seen, a large proportion of the compound outcome is due to inpatient mortality, as found in the studies men tioned as well as our own. It is clear that MAKE evaluation provides important information regarding these patients' outcomes; however, looking at its individual components also supplies other relevant data, as done in our study.
Within the renal outcomes, 65.62% had full recovery of renal function, 21.87% had partial recovery and 12.5% were dialysis-dependent at 90 days, with similar results after one year. Compared with similar studies, there was a lower per centage of RRT requirement compared with the FINNAKI study 22 (18.9%) and a greater percentage compared with the RENAL 23 and IVOIRE 24 studies (5.6% and 1.4%, respectively). At one-year follow up, there was a similar need for RRT in the studies by Meersch et al. 20 and Conroy et al. 19, coinciding in the association of this outcome with oligo/anuria and worse kidney function on admission 15. An association was found between worse kidney function on admission (kidney stage 3b) and the need for chronic dialysis, just as in studies by other authors 15,25-27.
The bivariate analysis showed an association between the type of therapy and timing of initiation, and MAKE and mortality. Regarding the continuous therapy outcomes, these could be explained by the implementation of this therapy in patients with greater hemodynamic instability, reflecting a worse clinical condition at a given time. Most randomized studies have not shown any differences when evaluating the therapy modality, mentioning the great equality between the various study arms compared with ours 28,29. Further more, an association has not been found between dialysis dependence and the modality of treatment, a situation which some authors have presented in their papers, noting that the vast majority of these are observational studies 30-32. In Schneider et al.'s systematic review 33, this hetero geneity is mainly found in observational studies, in which differences are found in clinical outcomes, as opposed to randomized studies.
Regarding the timing of initiation, we found worse results in MAKE and mortality in the group with late initiation, with no effect found on kidney outcomes. These findings differ partially from the randomized studies of recent years. We share findings with the ELAIN study 34 with, however, a clear difference in the definition of early initiation, which makes comparison difficult. On the other hand, in other randomized studies with 28 and 90-day follow up and a similar initiation criterion to ours, there is no similarity in the findings, which could be partially explained by the dif ference in the number of patients in the treatment initiation groups compared with these papers 21,35-37. While there are differences in the findings with regard to mortality, there is consistency in the kidney outcomes, corroborated by vari ous meta-analyses 38-40.
The strengths include: a broad analysis of the condi tions associated with clinical outcomes not included in other publications, as well as 90-day and one-year follow up. The MAKE evaluation is a more comprehensive way of analyzing the effects of treatment in this type of patient. The limitations include retrospective data collection, a sample from a single institution, the different number of patients according to the type and timing of RRT, the low number of patients in follow up, and not including other sociodemographic and nutritional variables which could be determining factors in mortality.
In conclusion, the APACHE II score, high blood pressure, NSAIDs, obstructive uropathy, metabolic acidosis, anuria, hypercalcemia and uremic encephalopathy were associated with the need for RRT at 90 days. Mortality was greater in patients with late-starting or continuous RRT. Anuria, a higher APACHE II score, and continuous or late-starting RRT are more frequent in patients who develop MAKE.

