English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
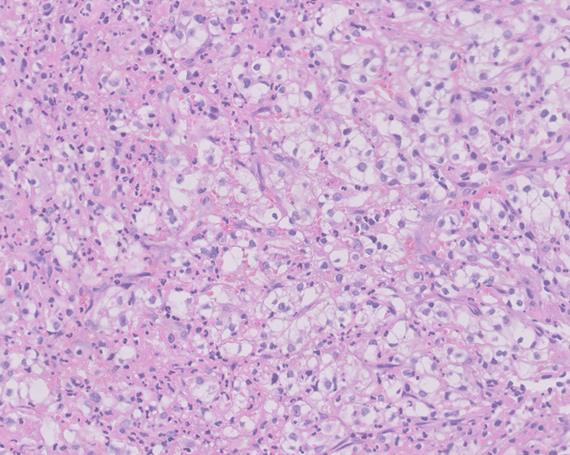
PermalinkA 68-year-old woman, with no relevant medical history, was undergoing outpatient studies due to a small amount of painless gross hematuria and a kidney mass detected on ultrasound. She presented to the emergency room with a complaint of three months of asthenia, weight loss and dyspnea. Laboratory tests showed iron deficiency anemia (hemoglobin of 4.6 g/dL and ferritin of 11 ug/L). She underwent an upper GI endoscopy which revealed an eroded ampullary lesion suggestive of malignancy (Figure 1). Abdominal ultrasound confirmed the presence of an 8 cm kidney mass compatible with a kidney neoplasm (Figure 2) and a periampullary duodenal lesion with endoluminal infiltration. The histopathological study of the duodenal lesion showed ulcerated tissue infiltrated with renal carcinoma (Figure 3). In this case, the appropriate work up for iron deficiency anemia was able to adduce the duodenal lesion, which was compatible with metastasis. The ampulla of Vater is an unusual site for renal cell carcinoma metastasis and may present as GI bleeding, obstructive jaundice or iron deficiency anemia without obvious bleeding 1. The current treatment for renal carcinoma has improved its prognosis; it includes radical or partial nephrectomy with a curative intent, immunotherapy, and targeted therapy. Metastasis resection is available in some cases in which there are inoperable conditions 2,3.