











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkA 66-year-old man with a history of heart failure (HF), hypertension and chronic kidney disease was admitted to the emergency room with symptoms of acute decompensated HF. A transthoracic echocardiogram showed severe aortic regurgitation. Coronary angiography showed dilation of the ascending aorta (43 mm) and the aortic root. A computed tomography with contrast showed multiple > 5 mm cystic lesions in the liver and kidneys (Figure 1A and B); there was a single cyst in the head of the pancreas (Figure 1C). The patient had normal liver enzymes and elevated CA 19-9. He was diagnosed with autosomal dominant polycystic kidney disease (ADPKD). Brain aneurysms were ruled out with angiography. The patient underwent ascending aorta and aortic root replacement and was discharged with improved symptoms. Autosomal dominant polycystic kidney disease can affect the liver and pancreas, and may be associated with aortic or cerebral artery aneurysms 1,2.
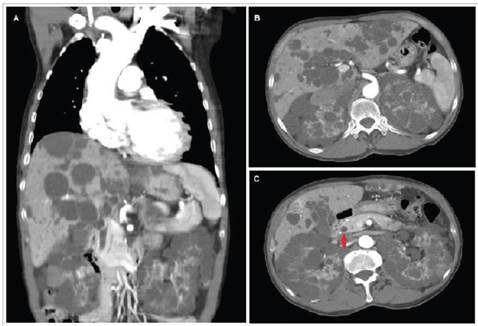
Figure 1 Abdominal tomography with and without contrast A. Coronal section showing dilation of the aortic root and ascending aorta, and cysts in the liver and kidneys. B. Transverse section showing multiple cystic lesions in the parenchyma of the liver and both kidneys. C. Transverse section showing cysts in the head of the pancreas marked by the red arrow and multiple cystic lesions in the liver and kidney parenchyma.

