English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
This paper aims to compute unjust health inequalities in Colombia based on a statistical association between health status through adulthood and socioeconomic characteristics during childhood. This relationship could be understood in the context of intergenerational health mobility analysis, i.e., the way in which childhood circumstances affect health through adulthood. In addition, this paper aims to show the implications of this association on health inequalities. It emphasizes on what the equality of opportunity theory calls an unjust inequality. Given that analyzing these inequalities implies normative judgements, this paper is a microjustice view of health inequalities (Kolm, 2002b). To do this, we use the Colombian Longitudinal Survey of the Universidad de Los Andes. We use information from 2010 because data related to self-reported health status (only available for that year) is needed. First, we use OLS as the estimation method. Using the estimates from this method, we apply the approach proposed in Fields (2003), which is based on Shorrocks (1983), to compute the participation of childhood circumstances in the inequalities in self-reported health status. These participations are known as unjust health inequalities.
Why equality is important for a society? Because it is desirable to have a society of quality, quality expressed in terms of the social relations that compose it. The term “quality” is associated with justice, and justice, rationally, leads to equality. If society gives X benefits to an individual because he/she has Y characteristics, another individual with similar Y characteristics should have access to the same benefits. Nevertheless, the above does not provide an answer to the question of equality of what? About this, there are answers that place emphasis on individual welfare (subjective welfare; for example, utility), resources, final outcomes, capacities and others (Dworkin, 1981a, 1981b; Fleurbaey & Maniquet, 2011; Fleurbaey, 1995; Sen, 1979, 1985).
Some philosophical theories propose a rationalization of the definition of “inequality” beyond those associated with individual preferences or physical resources. According to Arneson (1989) and Cohen (1989), final outcomes are conditioned by two broad characteristics: circumstances and efforts. The former are socioeconomic characteristics forming the individual, they are not under the individual’s decision process (i.e., the individual does not control them) and thus the individual should not take any responsibility for them. The latter are socioeconomic characteristics that are under the individual’s control (because he/she has the freedom and willingness to choose) and hence he/she should be responsible for them. This theory is called equality of opportunity and defines the inequalities caused from circumstances as unjust inequalities because the individual is subject to consequences from decisions he/she did not take. Inequalities caused by individual effort are considered legitimate (at least to some extent) because they are caused by the individual’s own decisions. In this case, what is relevant for evaluating a state of affairs are the unjust inequalities. Having said that, the individual must be compensated by final outcomes conditioned on circumstances, i.e., society should have the duty to alleviate the inequalities that prove to be unfair.
Health plays an instrumental role in the social development of individuals. Individuals have to be as healthy as possible to carry out daily activities that involve mental and physical efforts. Many of these activities are critical (e.g., to reason, to eat, to write, etc.). Health should be considered as a special good (Anand, 2002). For that reason, ideally, health should not be affected by any socioeconomic characteristics, as could be the case for other individual characteristics (e.g., earnings or monetary income). If a society is fair, that society guarantees all individuals the opportunity to achieve their life plans, assuming that they have the physical and mental capacities to desire a goal and to pursue it. Thus, a fair society is a society that guarantees opportunities for individuals to have a good health.
Under the principles of the theory of equality of opportunity, society must fight for the reduction of health inequalities that are unjust, i.e., health inequalities that are caused by circumstances. As it will be seen later, health inequalities in Colombia are usually measured from the use and access to health services. However, conclusions about health inequalities cannot be circumscribed only to an institutional perspective. Equality of opportunity offers a theoretical framework for a richer analysis because inequality is contextualized on normative judgments. Given the subcategorization that must be given to justice (Kolm, 2002b), this paper aims to apply the theory of equality of opportunity to health issues. Specifically, this paper studies the inequality of opportunities to have a good health in Colombia. To do this, the first objective is to find a statistical relation between individual circumstances as possible determinants of health. Health inequalities conditioned to this relation are considered as unjust inequalities.
I. Literature review
The theory of equality of opportunity
In the previous section we discussed equality of opportunity. Given this definition, there is a notion to make the individual responsible for the consequences of his/her decisions because we assume that these decisions are free and well informed. Ultimately, the most interested in getting the greatest welfare is the individual himself/herself.
The main objective of society is to give freedom of choice to the individual as long as equality plays an instrumental role, where everybody should have the same freedom to take decisions. Because inequalities may come from circumstances and individual effort, conjectures about justice arise. Inequalities caused by circumstances can be considered illegitimate and researchers can place special emphasis on these, instead of focusing on inequalities in general. With this new normative judgment, we are interested in measuring unjust inequalities rather than total inequalities. According to Fleurbaey and Schokkaert (2011), there are two principles that an unjust health inequality measure must meet:
(i) To give equal benefits to individuals equally responsible (Compensation).
(ii) To disregard legitimate inequalities (Reward).
The first principle is related to the compensation principle and the second one relates to the reward principle (Fleurbaey, 2008). The compensation principle disregards individual disadvantages arising from circumstances, while the reward principle allows individuals benefits associated with higher effort (Arnsperger, 1994; Kolm, 1995; Varian, 1974).
Nevertheless, these two principles are mutually exclusive. For example, if unjust inequality measures satisfy the reward principle, it does that because it does not consider individual effort. But the compensation principle considers individual effort. Thus, if the inequality measure satisfies the reward principle, it cannot fulfill the compensation principle (or vice versa). Legitimate inequalities are related to individual effort. Then, the research needs to choose one of these two principles as the basis principle of unjust inequality measures. Fleurbaey and Peragine (2013) show that, beyond having an excluding restriction between the compensation principle and the reward principle, there is an excluding restriction between an ex-ante and an ex-post unjust inequality measure.
The equality of opportunities approach has been applied in different fields of economics. For example, see Roemer et al. (2003), Brunello and Checchi (2007), Ferreira and Gignoux (2011), Lefranc, Pistolesi and Trannoy (2008, 2009), Pistolesi (2009) and Schütz, Ursprung and Wößmann (2008). The theory of equality of opportunity has been applied also to health issues. For example, see Fleurbaey and Schokkaert (2009), Jusot, Tubeuf and Trannoy (2010, 2013), Rosa Dias (2009), Rosa Dias and Jones (2007), Trannoy et al. (2010) and Jusot, Mage and Menendez (2014).
Jusot et al. (2010) find Gini coefficients for inequalities of opportunities in health ranging from 0.09 to 0.16. Sweden reports the smallest inequality, while Spain reports the greatest inequality. Europe as a whole reports a Gini coefficient of 0.10. Trannoy et al. (2010) confirm the presence of inequality of opportunities in health in France, with a Gini coefficient of 0.155. In addition, they find that parental socioeconomic status is the most important circumstance to explain health inequalities on descendants’ health through adulthood. Also, Rosa Dias (2009) finds inequality of opportunities in health in the United Kingdom of about 21.5%-26.3% of total health inequality using a pseudo-Gini coefficient as the inequality measure. There is little literature about this topic in developing economies. An exemption is a study about Indonesia. Jusot et al. (2014) show that parental health is the major transmission mechanism of inequality of opportunities in health. Circumstances account for a share of 10% in total health inequality.
It should be stressed that there is no clarity about which characteristics must be considered as circumstances. However, when it comes to health, socioeconomic characteristics through childhood are the first option because they accomplish the definition that theory gives to circumstances. An individual does not control or does not decide which socioeconomic characteristics should have when he/she is born. There is evidence that children from vulnerable households report the worst health status and this has a lasting impact throughout life. Likewise, children with the worst health status have lower educational attainment and hence lower social mobility through adulthood (Case, Lubotsky & Paxson, 2002; Case, Fertig & Paxson, 2005; Strauss & Thomas, 2008).
Felitti et al. (1998) find an association between childhood circumstances and the adoption of risk factors that affect health in adulthood (e.g., alcoholism and substance abuse). The childhood circumstances considered are those situations that reflect any household dysfunctionality or adverse situations (physical and sexual abuse or related events). Felitti et al. (1998) present evidence that individuals that have a difficult childhood have the worst health status and are more likely to get sick. For example, the probability to be a smoker is twice for individuals suffering an adverse circumstance. Something similar happens with the prevalence of heart disease, cancer, stroke, chronic bronchitis or emphysema, diabetes, bone fractures, hepatitis and self-reported health. However, Felitti et al. (1998) emphasize the need to substantiate more complex relations that could highlight a direct causality between childhood circumstances and health in adulthood beyond the instrumental role that risk factors have.
Health inequalities in Colombia
Bernal and Cárdenas (2005) study the existence of health inequalities attributable to race. They find that individuals belonging to ethnic minorities are less likely to have medical insurance, have worse perceptions about their health status and are more likely to get sick, although they use less hospital services. The authors conclude that there are not significant differences in health outcomes between ethnic groups. Access to health services and self-reported health do not have a statistically significant relation with race when they control for other socioeconomic characteristics such as labor force status, educational attainment, geographic location, and the like. This implies, according to the authors, that worse health perceptions by ethnic minorities are related to relative disadvantage over other socioeconomic characteristics.
Acosta (2014) analyses regional inequalities in self-reported health. She uses the methodology of Allison and Foster (2004) to get an approximation to health inequality indexes based on qualitative data. As could be expected, the most prosperous regions report better health status. The conclusion from Acosta (2014) is consistent with estimations of life expectancy at birth reported by the National Department of Statistics (Departamento Administrativo Nacional de Estadística, in Spanish) based on the census conducted in 2005. According to Naga-Yalcin indexes, regions with the highest health inequalities in 2010 are the East Central region and the West Central region. Between 2005 and 2010, health inequalities have increased. Women report higher use of medical services, according to the author, consistent with the fact that women report the worst health status.
Camacho and Flórez (2012) analyze equity in maternal and child health services conditioned by geographic area and wealth quintiles. The implementation of the subsidized regime encourages the use of health services, thus contributing to reduce health inequalities by region and socioeconomic characteristics. However, quality has not improved given its focalization and financing. Indicators of maternal and child health exhibit improvements with increases in coverage of maternal and child health services. In addition, they observe a drop in child morbidity without implications for inequality. The authors suggest the possibility that other social characteristics determine these results.
Fresneda (2010) performs a retrospective analysis on the dynamics of health inequalities in Colombia between 2000 and 2007. He relies on self-reported health status, perceived disability and risk of communicable diseases, external injuries, morbidity and demand for health services. He finds that self-reported health is better in urban areas relative to the reports of rural areas. Likewise, men report better health compared to what women report. Regarding the health regime in which an individual is affiliated, those who are affiliated to a special regime and the contributive regime report better health status compared to those who are affiliated to the subsidized regime. Something similar happens when individuals live in higher socio-economic strata and have more years of education.
Finally, Flórez and Soto (2007) identify inequalities at the geographical and gender levels and in the use of services in 1990, 1995, 2000 and 2005 using information available from the Demographic and Health Survey. Regarding insurance, there were significant gains in universal enrollment, particularly between 1995 and 2000. The authors associate this fact with the inclusion of relatives in the contributive regime. Also, the largest affiliations occur across richer regions. Between 2000 and 2005, inequalities in the use of medical services increase by region, gender and wealth quintile. Nevertheless, prenatal care inequalities are reduced between 1990 and 2005 for all socioeconomic characteristics. As for child mortality, inequalities are reduced between 1995 and 2005; however, individuals in rural areas and poor regions and boys still report higher mortality rates. Inequalities in chronic undernourishment increase, except when the authors control for gender.
Considering all the previous results, insurance coverage and health service availability have increased remarkably since enactment of the health bill currently in place (Ley 100 de 1993). These improvements were focused on the vulnerable population through the subsidized regime. Even so, quality of services depends on regime affiliation, where better regimes (i.e., contributive and especial) report better health indicators. In addition, it can be observed a higher use of medical services associated with the increased availability of services, but inequalities in the use of services by wealth quintiles or region (rural vs. urban) are still evident. Richer regions report better distributions of health states, always favoring the central regions. There is no evidence of health inequalities between ethnic groups, but inequalities conditioned to other socioeconomic characteristics (education, occupation, wealth quintile, region, and the like) are often found.
All the previously cited literature has been focused on total health inequalities. Nevertheless, Fajardo-Gonzalez (2016) conducts an analysis of equality of health opportunities from a normative perspective related to the analysis attempted herein. Using data from the 2010 Living Standards and Social Mobility Survey, she calculates dissimilarity and Gini-opportunity indexes to provide different measures of inequality of opportunity in adult health. Additionally, she applies Shapley-value decompositions to estimate the contribution of circumstances on the dissimilarity index. Her findings suggest that about 10 percent of circumstance-driven opportunities enjoyed by those who are healthier should be redistributed among those less healthy and thereby attain equality of opportunities. The most important circumstances of inequality of opportunity in adult health are household socioeconomic status during childhood and parental education.
Often, health inequalities in Colombia have been analyzed from an institutional perspective, i.e., studies place emphasis on access to health services and how much individuals use them. Nevertheless, health cannot be measured only as use of health services and access to them. This paper uses data from the Colombian Longitudinal Survey under the framework of the equality of opportunity theory and, rather than emphasizing on total health inequality (of self-reported health), it focuses on unjust health inequalities under a normative framework of social justice. It could be said that this is the first analysis of this kind in Colombia, and therefore this paper contributes to the literature on unjust health inequalities.
II. Data
The empirical analysis is based on available data from the Colombian Longitudinal Survey (ELCA, for its acronym in Spanish) in 2010. This survey interviews 10,164 households, of which 5,446 are urban households distributed over five regions (Atlántica, Pacífica, Central, Oriental and Bogotá) and 4,718 are rural households from four microregions (Atlántica Media, Eje Cafetero, Cundiboyacence and Centro Oriente). See Bernal et al. (2014).
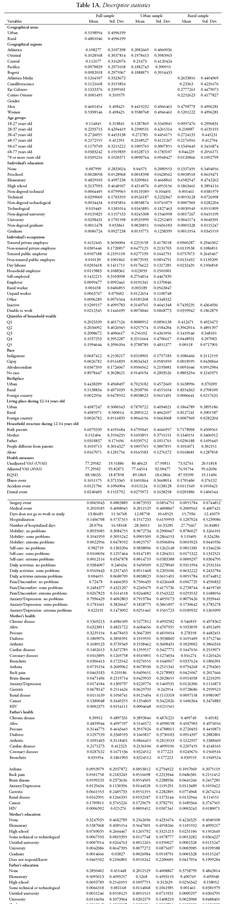
ELCA has data from households, communities and individuals. In this paper, we use data from individuals. These data are divided into four categories: demographic characteristics, childhood circumstances, effort and (present) socioeconomic status. Given that we are interested in measuring health inequalities, health is measured as self-reported health status, and thus the sample is reduced to individuals for which data on health status are available. In the ELCA, data on health status are only available from the household head and his/her spouse. Additionally, the sample is restricted to individuals older than 17 years and for which there is information regarding parental education.1 The final sample has 15,682 observations (see Table 1A in the annex on descriptive statistics).
For the econometric models below, demographics, childhood circumstances, effort and socioeconomic status are all considered independent variables. The demographical variables are region of living and age cohort. Childhood circumstances are identified by race, birthplace, living place, household structure, parental health and parental education. Individual effort refers to preventive use of health services. Finally, the variables pertaining to socioeconomic status are occupation, education and wealth quintile.
It should be noted how parental health is measured. Mother’s health (father’s health) is an interaction term between the fact that the mother (father) is still alive at the moment of the interview and the fact that she (he) does not suffer from any chronic disease. Chronic diseases considered in the ELCA are high blood pressure, diabetes, arthritis or joint pain, heart disease, coronary disease, chronic bronchitis, asthma, back pain, stroke, depression or anxiety, gastritis, kidney disease, cancer and HIV.
The health status of an individual is measured with the Visual Analogue State (VAS) and EQ5D (Brazier et al., 2007). The VAS is a cardinal measure of self-reported health status. Individuals qualify their health with values between 1 and 100, where 1 represents the worst health status and 100 represents the best. Given its characteristics, the VAS is a subjective measure. The other measure, EQ5D, is a standard health measure developed by the EuroQol Group (Szende, Oppe & Devlin, 2007). This measure generates a specific health value based on information from individuals about mobility, self-care, daily activities, pain or discomfort and depression or anxiety. Specifically, each of these variables is ranked with three levels: no problems, some problems and serious problems. What the measure aims to capture is the capacity with which an individual can perform regarding these aspects. It should be noted that health state is a combination of three possible rankings from the five variables mentioned above. For example, perfect health is present when an individual has no problems in regard to the five mentioned aspects. The worst health, in contrast, is present when an individual has serious problems regarding these. With all possible combination of rankings and variables, EQ5D covers 253 health statuses. As VAS, the EQ5D is a cardinal continuous measure.
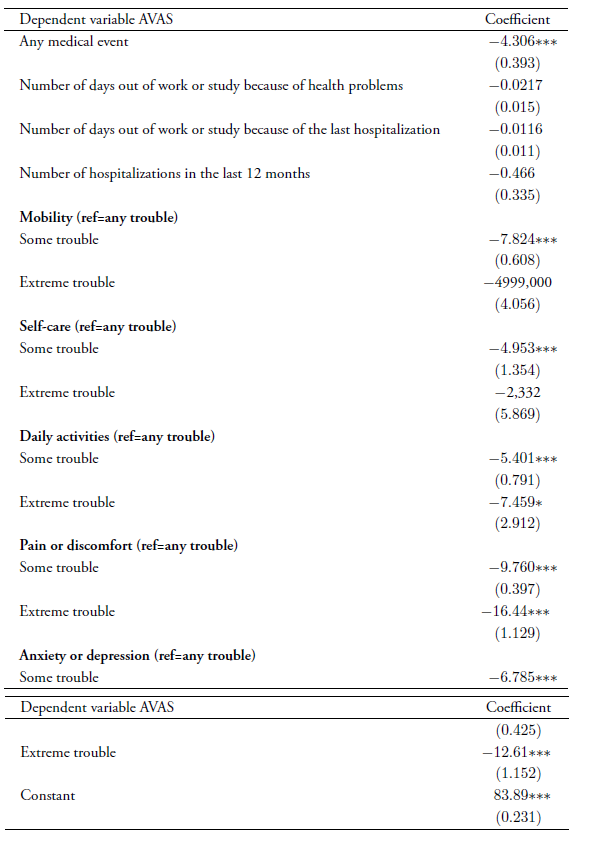
There is some controversy on the convenience of using subjective health indicators.2 Some authors say that self-reported health can be a good predictor of mortality rates and medical service use rates (Idler & Benyamini, 1997; Nielsen, 2015). However, others are concerned about the reliability of these health indicators (Clarke & Ryan, 2006; Crossley & Kennedy, 2002; Sen, 2002). For this reason, we construct an alternative health measure that reflects a VAS more associated with medical characteristics. Considering VAS as the dependent variable, we specify a linear regression model as follows:
 ()1
()1
Where eventi is the fact that the individual i had a medical event in the last 30 days. We consider as a medical event whether the individual has had an illness or pain, an accident or physical injury, an ambulatory surgery or any event involving hospitalization. daysi is the number of days that the individual has not been at work or study due to the above mentioned medical events, timesi is the number of times that the individual has been hospitalized in the last 12 months, and lasti is the number of days the individual did not go to work or study because of the last hospitalization in the last 12 months. All other controls ( level2i and level3i ) represent how problematic the individuals find the aspects considered in the EQ5D measure because they capture the individuals’ attitudes toward their health. The alternative health measure is represented by adjusted values of the model. Finally, we have three health measures: unadjusted VAS (UVAS), adjusted VAS (AVAS) and EQ5D. Table 1 shows the results from the OLS estimation of Equation (1).
III. Empirical methods
Estimations
According to the theory of equality of opportunity, inequality of final outcomes is attributable to both circumstances and effort. Because the dataset has more information related to childhood circumstances, our measure of inequality of opportunities in health conforms to this fact. For this reason, the measure as presented here is an ex ante measure of health inequality (see section I).
The theoretical basis for measures of unjust inequalities is Roemer (1998). According to this author, the general case is that in which the final outcome is affected by circumstances and effort; and equality of opportunities requires that individuals be compensated for any difference in circumstances that could affect the final outcome, but not for any difference in effort. For Roemer (1998), a “type” is a group of individuals with similar circumstances. Clearly, individuals of the same “type” could have different final outcomes. For this reason, each “type” has a distribution of individuals based on their final outcomes. Roemer (1998) assumes a monotonic relation between final outcomes and individual effort. This means that within a “type” an individual makes more effort if he is in the top percentile relative to other individual of the same “type”. Then, for Roemer (1998), the effort to be considered is the effort that does not depend on circumstances. Two individuals of different “types” make the same effort if both are on the same percentile of their respective “type”.
Having said that, there is a discussion regarding the correlation between circumstances and effort. Barry (2005) argues about the need to ignore the conditionality imposed by individual circumstances on future effort, that is, individual effort (taking care of his/her health) must be considered independently of the influence of past circumstances. Jusot et al. (2013) show the empirical implications of different normative conjectures. They rely on three premises and measure the inequality of opportunities that different assumptions involve. At the end, their results suggest that the relative participation of circumstances and effort on health inequalities are very similar regarding their three premises. See also Balia and Jones (2011).
According to the above, we specify two linear models regarding inequality of opportunities in health:3 one considering Roemer’s normative principle and the other considering Barry’s one. We get
 () 2
() 2
In this model, we assume a linear relation between self-reported health S (UVAS, AVAS or EQ5D) and socioeconomic characteristics(demographics (Demog), circumstances (Circums), effort (E f f o) and economic status (Stat)(at an individual level, hence the subscript i. Equation (2) identifies Barry’s normative principle, in which only direct effects of circumstances on health are considered. Now, given the conditionality of circumstances on effort, we get
 3
3
 . ()4
. ()4
Replacing from Equation (2), we get
 ()5
()5
 ()6
()6
 ()7
()7
where
 ()8
()8
 ()9
()9
 ()10
()10
 (8) ()11
(8) ()11
Equation (7) identifies Roemer’s normative principle. Equations (2) and (7) are estimated in the next section. Ramos and van de Gaer (2015) carry out a meta-analysis about the different ways of measuring inequality of opportunities. They find that the literature distinguishes between direct and indirect measures, ex ante and ex post measures and parametric and nonparametric measures. Using their terminology, the measure that we present below is a parametric, direct and ex ante measure of inequality of opportunities in health in Colombia for 2010.
Measuring inequality of opportunities in health
There is no consensus on the best way to measure inequality of opportunities. According to Ramos and van de Gaer (2015), on many occasions measures of inequality of opportunities do not have any theoretical basis and are ad hoc choices by researchers. Under these conditions, we apply the methodology proposed by Shorrocks (1982) to establish the contribution that every income source (earnings, capital income, transfers, etc.) has on total income inequality. Shorrocks (1982) poses the principles that must be met by any decomposable index, resulting in the following decomposition rule:
 ()12
()12
where Sj is the share of total inequality associated to Xj source. This decomposition rule is well behaved (Shorrocks, 1983). However, in this paper, rather than having different components that generate a final health status, there is a data generating process (an OLS estimation) that aims to approximate the performance of individual health status. Therefore, we need to adapt Shorrocks's (1982) methodology to an analysis of inequality based on regressions. This is what Fields (2003) precisely does, showing that the new decomposition rule is
 ()13
()13
where aj is the estimated parameter in the regression of Y on Xj and Sj is the share of total inequality associated with factor j (Xj) . This decomposition rule is characterized by
 ()14
()14
that is, all shares from the linear regression model (including participations from intercept and residuals) must sum 100%. When we exclude the share of residuals, we get
 ()15
()15
The participations from the explanatory variables are equivalent to the goodness of fit of the model. Then, we can establish that the percentage of total inequality explained by factor j is
 ()16
()16
The methodology adopted by Fields (2003) allows us to compute the participation of unjust inequalities on total health inequalities.
IV. Results
Estimations
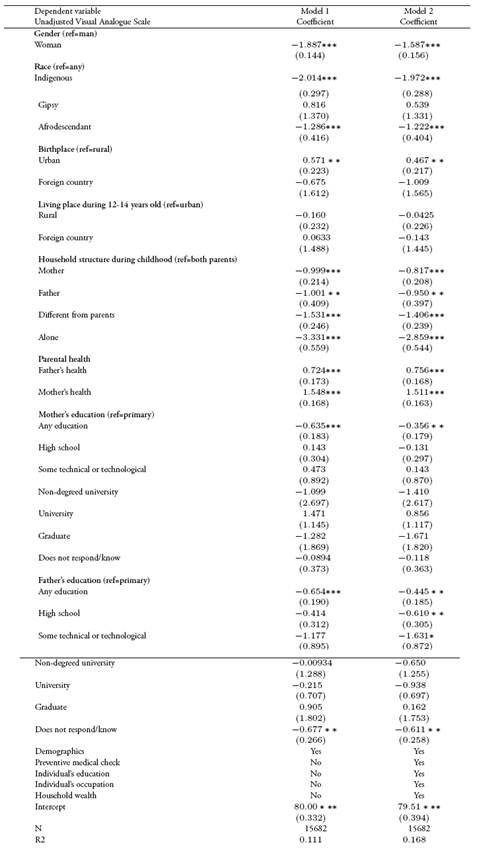
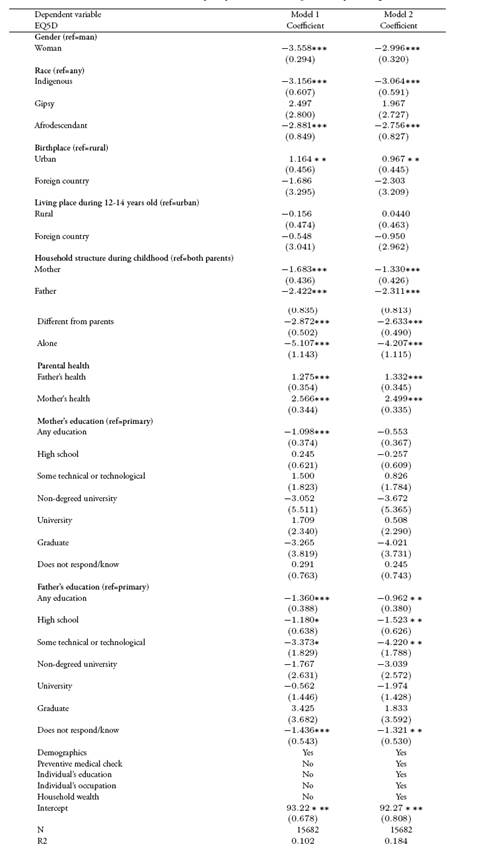
We present the OLS estimations of Equation (2) through Equation (7). Given that we have three dependent variables (UVAS, AVAS and EQ5D) and two normative principles, we estimate six regression models. Nevertheless, we present the estimates concerning UVAS only (see Table 2). Results for AVAS and EQ5D are similar, both qualitatively and quantitatively (see Table 2A and Table 3A, respectively, in the annexes). In Table 2, Model 1 identifies Roemer’s normative principle (Equation (7)), while Model 2 identifies Barry’s one (Equation (2)). Women report worse health states in comparison with men. This relation is statistically significant. Having been born in urban areas is associated with positive changes in self-reported health relative to rural areas. Regarding household composition, it is ideal to have lived with both parents. People that lived with one parent only, lived with individuals different from their parents or lived alone during childhood have the worst self-reported health status. This relation is statistically significant. As for parental health, having parents alive and without any chronic illness at the time of the survey is important for descendant’s health, a relation that is positive and statistically significant. Finally, that parents have no education shows a negative relation with a descendant’s self-reported health.
Table 2 OLS estimations of unjust health inequalities for UVAS
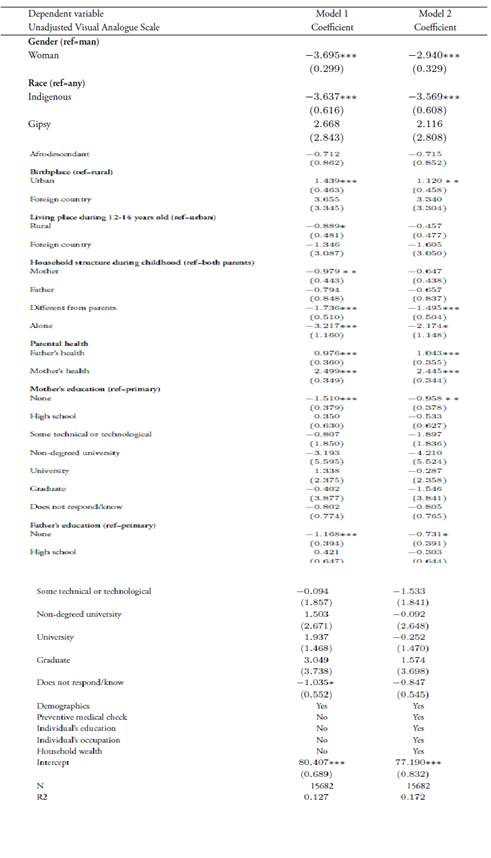
Note: standard error in parenthesis; ***p<0.01. **p<0.05. *p<0.1.
Source: own calculations based on ELCA 2010.
Three situations arise that should be noted. First, the coefficient of mother’s health is higher than the coefficient of father’s health (and, as will be seen later, this is true independently of the health measure). Second, coefficients estimated for Model 1 are higher than coefficients of Model 2. This is so because Roemer’s principle (Model 1) accounts for total effects (direct and indirect) of circumstances on health, while Barry’s principle (Model 2) takes account of direct effects only. This enables us to confirm, in addition, an association between individual circumstances and present socioeconomic status. Finally, the use of health services for preventive reasons shows a negative relation with self-reported health. A possible explanation for this is related to the endogeneity of variables; that is, individuals that report the worst health use health services more often.
Estimations for Model 1 could be biased due to endogeneity issues. Given that we do not control for effort and because of the correlation between circumstances and effort, we could be violating the assumption of exogeneity for OLS estimation (i.e, E(u|X) ≠ 0). In this case, the coefficients of circumstances are biased because they capture both direct and indirect effects (absorbed from effort). However, we are fulfilling Roemer’s principle. Thus, we do not correct for endogeneity in Model 1 for any of the health measures.
Inequality of health opportunities in Colombia
Table 3 shows the participations associated with Equation (16) for UVAS, AVAS and EQ5D applying the two normative principles. Inequality of opportunities in health represents almost 30% of total inequality in self-reported health if we consider Barry’s principle. Roemer’s normative principle exhibits a higher degree of inequality of opportunities against Barry’s principle because the former takes into consideration both direct and indirect effects of circumstances on the final outcome (i.e., self-reported health status), while the latter principle only takes direct effects into account.
Table 3 Inequality of opportunities in health in Colombia

Source: own calculations based on ELCA 2010.
Contextualizing results from the first and second columns of Table 3 on an inequality measure, the third and fourth columns of the same table reports Gini coefficients associated with inequality of opportunities in health for all three self-reported health measures. According to these Gini measures, total self-reported health inequalities are around 0.1214, 0.0521, and 0.0799 for UVAS, AVAS and EQ5D, respectively. Considering the proportions reported, those Gini coefficients of inequality of opportunities in health are 0.0538, 0.0244 and 0.0344 for Roemer’s principle and 0.0268, 0.0153 and 0.0178 for Barry’s principle.
These reported participations in Table 3 are conditioned on observable information related to individual circumstances, therefore the values that are shown should be considered as a lower bound for the true inequality of opportunities in health. Table 4 shows the participations of observable individual circumstances in unjust health inequalities for the three health measures.
Table 4 Circumstances and unjust health inequalities in Colombia
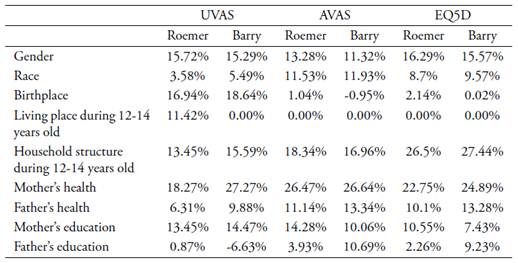
Source: own calculations based on ELCA 2010.
For the three health measures, the most important circumstance for total inequality of opportunities in health is mother’s health. Birthplace and gender have considerable participations for UVAS only. Their participations in inequality of opportunities in health range between 15% and 18%. Also, household structure during childhood has a significant participation (after mother’s health) for AVAS and EQ5D. The normative approaches of Roemer and Barry have some implications for measuring inequality of opportunities when health status is measured by AVAS. For Roemer’s principle, the third most important circumstance affecting unjust inequalities is mother’s education (14.28%); in contrast, the third most relevant circumstance applying Barry’s principle is father’s health. There is a particular result with respect to UVAS using Barry’s principle. The participation of father’s education is negative, meaning that inequality of opportunities in health is reduced for higher levels of father’s education by a factor of -6.63%.
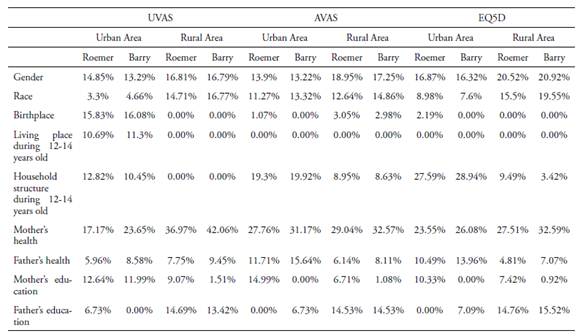
Based on a geographical approach, inequality of opportunities in health is higher in rural areas than in urban areas.4 Table 5 shows the participations of circumstances on total health inequalities in rural and urban areas.
Table 5 Circumstances and unjust health inequalities in Colombia: rural and urban areas
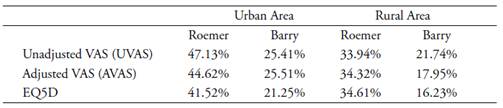
Source: own calculations based on ELCA 2010.
Table 9 shows the participations of observable circumstances in unjust health inequalities in rural and urban areas. Unlike our findings at the national level, household structure during childhood does not have a relevant share in unjust health inequalities. For all the health measures considered, gender and mother’s health are circumstances that account for a significant proportion of inequality of opportunities in health. For instance, according to Roemer’s principle, gender has a share of 20.52% and mother’s health has a participation of about 27.51% in EQ5D. The relative significance of father’s education and race depends on the normative principle that is used. For Roemer’s principle, father’s education is the third circumstance with the highest participation, whereas race is the third most influential circumstance for Barry’s principle. This is the case for UVAS and AVAS. For EQ5D, the third most important circumstance is race regardless of the normative principle considered.
Table 6 Circumstances and unjust health inequalities in Colombia
Source: own calculations based on ELCA 2010.
As mentioned above, mother’s health represents the highest share of unjust inequalities independently of the health measure. Gender has the second highest proportion. The trade-off between circumstances conditional on a normative principle is between father’s health and race for health measures UVAS and AVAS in rural areas. For EQ5D, the third circumstance with the highest participation in unjust inequalities is race.
Observed patterns in urban areas are very similar to what is evidenced at the national level (Table 3). In all cases, mother’s health has the highest participation in inequality of opportunities in health. This circumstance is followed by gender and household structure during childhood. This is conditional on the health measure. For AVAS, normative principles condition the significance of the shares of mother’s education and father’s health. Finally, in both rural and urban areas, inequality of opportunities in health applying Roemer’s principle is higher than with Barry’s principle. Moreover, mother’s health is the circumstance with the highest participation in unjust health inequalities in rural areas, as opposed to urban areas.
In general, mother’s health is the circumstance with the highest participation in inequality of opportunities in health regardless of the health measure, geographical area and normative principle. The opposite occurs with the rest of the circumstances. Their participations depend on the geographical area and the health measure. While household structure is the second most important circumstance in urban areas, in rural areas gender is the second most influential circumstance. Observable circumstances explain between 30% and 40% of total self-reported inequalities in health status conditional on the normative principle considered.
Concluding remarks
This paper aims to calculate inequality of opportunities in health in Colombia using available data from the ELCA for 2010. It is suggested that Colombia presents evidence of unjust health inequalities that explain between 30% and 40% of total inequality in self-reported health status. Based on our estimations, we intend to ascertain what individual characteristics and childhood circumstances affect health status through adulthood in greater proportion. Being indigenous or a woman and to have lived with people different from parents are circumstances that have a negative correlation with health. These relations are statistically significant. Also, having parents alive without any illness has a positive correlation with descendants’ health. For the three health measures considered herein, the incidence of inequality of opportunities in health depends on the normative principle considered. For example, considering total effects from circumstances on health (Roemer’s principle) means greater unjust inequalities as opposed to considering only direct effects (Barry’s principle). In addition, we show that unjust inequalities are more relevant in urban areas. Mother’s health is the most important circumstance in accounting for unjust health inequalities. This is true for all health measures, geographical areas and the two normative principles. At the national level, other circumstances such as gender and household structure during childhood are important in these kinds of inequalities. Differences between areas are evident in circumstances such as race and birthplace.
It is difficult to compare the results found herein with other studies. For example, Fajardo-Gonzalez (2016) uses a different methodology and dataset to estimate equality of opportunity in health. This is also true for all the documents cited. As expressed by Ramos and van de Gaer (2015), a unified methodology to estimate equality of opportunities does not exist and everything depends on the available data.
This study has several limitations. First, the estimations presented herein are limited by the data available; that is, a cross-section. The relevance of the analysis would be higher if we could see the dynamics of inequality of opportunities in health over time. Second, the reliability of self-reported health status (Clarke & Ryan, 2006; Crossley & Kennedy, 2002; Sen, 2002). We use self-reported information because of lacking data regarding objective health measures in the ELCA (at least in 2010). Finally, another limitation is the use of retrospective questions about childhood circumstances. The reason is that this information could not be accurate and generate biased estimations. As for recommendations for future research, the results presented herein could be disaggregated by age cohorts, gender, educational level and health regime, which would allow us to conduct a broader analysis and enrich the normative approach.
This paper offers an integral perspective to understand the dynamics of individual health status from a social justice judgment for a developing country such as Colombia. Beyond considering medical factors that can affect health status, we offer preliminary evidence that other factors, such as educational and social ones, can affect individual health. This should be kept in mind when formulating public health policies and motivate a more enlightening debate about this topic from a normative perspective