










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkColombian Journal of Anestesiology
versão impressa ISSN 0120-3347
Rev. colomb. anestesiol. vol.41 no.4 Bogotá out/dez. 2013
https://doi.org/10.1016/j.rca.2013.06.007
Scientific and Technological Research
Variables associated with the risk of suicide in patients with chronic pain seen in a hospital outpatient clinic in Bogotá
Variables asociadas a riesgo de suicidio en pacientes con dolor crónico atendidos por consulta externa en un hospital de Bogotá
Ana Carolina Amaya Ariasa'*, Angie Bruceb, Deisy Herránc, Angie Martín Arangoc, Katherine Munozd, Patricia Abellae
a Psychologist, Specialist in Social Research, MSc (c) Clinical Epidemiology, Educational Researcher, Universidad Manuela Beltran until 2011, Associate Researcher, Instituto de Investigaciones Clínicas, Faculty of Medicine, Universidad Nacional de Colombia, Bogotá, Colombia
b Last Year Student of Psychology, Universidad Manuela Beltran, Bogotá, Colombia
c Psychologist, Universidad Manuela Beltrán, Bogotá, Colombia
d Estudiante, Psychologist, Universidad Manuela Beltrán, Bogotá, Colombia
e Anesthesiologist, pain, Clínica de dolor Coordinator, ACED member, Bogotá, Colombia
* Please cite this article as: Amaya Arias AC, Bruce A, Arango AM, Abella A. Variables asociadas a riesgo de suicidio en pacientes con dolor crónico atendidos por consulta externa en un hospital de Bogotá. Rev Colomb Anestesiol. 2013;41:267-273.
* Corresponding author at: Instituto de Investigaciones Clínicas, Facultad de Medicina, Universidad Nacional de Colombia, Oficina 215, Edificio 471, Carrera 30 No. 45-03, Bogotá, Colombia.
E-mail addresses: acamayaa@unal.edu.co, anaamaya@hotmail.com (A.C. Amaya Arias).
ARTICLE INFO
Article history: Received 8 November 2012 Accepted 27 June 2013 Available online 5 October 2013
ABSTRACT
Introduction: The primary objective of this research is to determine the relationship between anxiety, depression, quality of life and the risk of suicide in patients with chronic pain. Method:Cross-sectional descriptive-correlational study of a consecutive sample taken from a census of the total population seen between December 2011 and January 2012. The sample included 49 patients of the El Tunal Hospital Pain Clinic in Bogotá. The following measurement tools were used: Health-Related Quality of Life (SF-36), Hospital Anxiety and Depression Scale, the Plutchik suicide risk scale and numeric pain scale.
Results: It was found that the largest percentage of the population (75%) perceived pain at a moderate-to-severe level; 34% were at risk of suicide and 25% had suicidal ideation. In terms of quality of life, the majority of patients felt that they were limited in their ability to move and perform physically demanding tasks; 75.5% of patients had experienced anxiety symptoms and 61.2% had symptoms of depression. Finally, there was no correlation between the risk of suicide and the perceived levels of pain. Significant associations were found between the risk of suicide and anxiety, depression, mental health, mental component, vitality and emotional role.
Conclusion: There is a need to undertake research designed to determine mediators between pain and emotional status, considering that this understanding appears to be crucial for improving the effectiveness of the interventions in these patients.
© 2012 Sociedad Colombiana de Anestesiología y Reanimación. Published by Elsevier España, S.L. All rights reserved.
Keywords: Quality of life, Anxiety, Depression, Pain, Suicidal Ideation
RESUMEN
Introducción: Esta investigación tiene como objetivo principal determinar la relación entre ansiedad, depresión, calidad de vida y riesgo suicida en pacientes con dolor crónico.
Método:Corresponde a un estudio de tipo descriptivo-correlacional y de corte transversal, con un censo del total de población atendida entre diciembre de 2011 y enero de 2012, bajo un muestreo consecutivo. La muestra estuvo conformada por 49 pacientes de la Clínica de Dolor del Hospital El Tunal de Bogotá (Colombia). Se usaron los siguientes instrumentos de medición: Calidad de vida relacionada con la salud (SF-36), Escala hospitalaria de ansiedad y depresión (HAD), Escala de riesgo de suicidio de Plutchik y Escala analógica numérica de dolor.
Resultados: Se encontró que el mayor porcentaje de la población (75%) percibe un nivel de dolor entre moderado y severo; el 34% presenta riesgo suicida, y el 25% ideación suicida; en cuanto a la calidad de vida, la mayor parte de los pacientes sienten limitaciones en su capacidad de desplazamiento y realización de esfuerzos físicos; el 75,5% de los pacientes presentan síntomas de ansiedad y el 61,2%, de depresión. Finalmente, el riesgo de suicidio no se relacionó con los niveles de dolor percibido. Se encontraron asociaciones significativas entre riesgo de suicidio con ansiedad, depresión, salud mental, componente mental, vitalidad y rol emocional.
Conclusión: Se plantea la necesidad de realizar investigaciones que permitan determinar los mediadores entre el dolor y los estados emocionales, pues este parece ser un aspecto central a comprender para mejorar la efectividad de las intervenciones en estos pacientes.
© 2012 Sociedad Colombiana de Anestesiología y Reanimación. Publicado por Elsevier España, S.L. Todos los derechos reservados.
Palabras clave: Calidad de vida, Ansiedad, Dolor,Ideación suicida
Introduction
According to IASP (International Association for the Study of Pain) pain is defined as an "unpleasant sensory and emotional experience associated with real or potential tissue injury, or described in terms of such damage"1; the experience as perceived by the subject is complex, affecting all dimensions (emotional, cognitive, physical, spiritual, and work, family and social life).2
According to the duration, pain has been classified as acute (less than 3 months) and chronic (more than 3 months).1 Bonica (1990) restated this definition and described chronic pain as that which "lasts for more than one month beyond the normal course for recovery, is associated with a chronic disease process, or reappears at intervals of months or years".3 Pain intensity is determined on the basis of the patient's report on a 1-10 numerical scale, where 1-3 is mild, 4-6 is moderate, and 7-10 is severe.1
Among the consequences of pain, anxiety and depression are some of the most commonly reported emotional responses in patients with chronic pain. They give rise to intense elaboration of catastrophic thoughts, intensifying pain perception.4 Moreover, research reveals that many chronic pain sufferers show reduced mobility and slower movements, usually resulting in greater atrophy of the affected body part and pain intensification.5
Pain experience has been treated mainly from the medical perspective, with a focus on the physiological process, without bearing in mind the importance of intervening on the emotional component and the psychological suffering, which are
significant disruptors of quality of life and recovery, and are even associated with suicidal ideation in certain instances.6
In view of the above, the proposed objective is to determine the relation between anxiety, depression, quality of life perception and risk of suicide in patients with chronic pain coming to the outpatient pain clinic at El Tunal Hospital in Bogotá D.C. The idea is to create awareness about the problems affecting these patients and the impact of chronic pain on this population.
Considering that suicidal ideation is a precursor to suicide attempts, this research is important because it will shed light on actions that may help prevent self-inflicted death and improve psychological interventions.
Methods
Design
Cross-sectional, descriptive correlational study.
Subject selection and description
Inclusion criteria: Spanish speaking Colombian national adults with a diagnosis of chronic pain non-secondary to an end-stage disease, who came to the outpatient pain clinic of El Tunal Hospital in Bogotá during the study period, and agreed to participate voluntarily in the study.
Exclusion criteria were: being in the process of filing for pension or indemnity payment by an institution due to pain, and inability to respond to the tests due to cognitive impairment or altered sensoryperception. These criteria were established in order to reduce the probability of bias in variable measurements due to potential malingering by this type of patients.
Consecutive sampling was proposed because this method ensures that sample representativeness is similar to that obtained with probabilistic sampling.7
Sample size
Sample size was calculated for the association between the risk of suicide risk and the quality of life, anxiety and depression variables. Considering that the expectation was to perform 12 correlations in data analysis, the stated confidence interval (alpha) was corrected using the Bonferroni correction.8 With the correction, an acceptable margin of error of 0.004 was obtained for each association, thus maintaining the overall confidence level of 0.05 for the study.
A sample size of 38 patients was estimated using the Epidat 4.0® software, for a 99.9% confidence interval, a power of 80%, and a significant association of 0.6. This calculation was corrected taking into consideration that the relative efficiency of the Spearman correlation, compared with Pearson's, is 0.91,9 and it was increased by 10% to account for potential losses. Finally, the suggested minimum sample size calculated for this study was 46 subjects.
A census of the total population seen between December and January 2011 and 2012 that met inclusion and exclusion criteria was used, because the number of patients seen was not very high and a large percentage were diagnosed with endstage disease. Therefore, given the resources available and the time of the study, it was decided to collect the largest amount of data that met the sample size requirement for the correlation analysis. A total of 49 patients were ultimately evaluated.
Tools
Health-Related Quality of Life Questionnaire (SF-36)
The SF-36 is designed to evaluate health-related quality of life (HRQoL), and consists of 36 items grouped in 8 sub-scales. It was found to offer acceptable validity and reliability results for application in Colombia.10 The scoring system is based on T scores with a mean of 50 and a standard deviation of 10 for each sub-scale.
Hospital Anxiety and Depression Scale (HAD)
The HAD is two-dimensional scale that allows to screen for anxiety and depression symptoms in the hospital setting. It consists of 14 items, with Likert-type responses between 0 and 3. In Colombia, this scale was also shown to have acceptable validity and reliability.11 Score classification in the sub-scales (anxiety/depression) are normal from 0 to 7, doubtful from 8 to 10, and clinical problem when the score is 11 or more.
Plutchik Suicide Risk Scale
This scale was designed by Robert Plutchik with the aim of separating suicidal patients from those who are not. It consists of 15 YES or NO questions. The Spanish version was validated by Rubio et al.12 It evaluates prior suicide attempts, the intensity of current suicidal ideation, and feelings of depression and
hopelessness. The original scale showed a consistency of 0.84 (Cronbach's alpha) and in the Spanish validation, Cronbach's alpha reached values of 0.90; and for the Spanish test-retest reliability, it was found that there was a pre- and post-test correlation of 0.89 after 72 hours. In this validation, the cut-off point proposed is 6, for 74% sensitivity and 95% specificity to discriminate between controls and patients (suicidal attempts and personality disorders). With the same cut-off point, sensitivity and specificity are 88% for discrimination between the subjects with a history of suicide attempt and those with no prior attempts. There is no validation of this scale for Colombia.
Analog Numeric Pain Scale
A 0-10 numeric scale was used to assess pain intensity, where 0 is no pain and 10 is the worst possible pain. Questions were asked about intermediate, highest and lowest pain level perceived over the previous week and the pain level at the time of assessment.
Ethical considerations
The study was approved by the El Tunal Hospital ethics and research committee. The most important recommendation, actually accomplished, was to refer all patients with a risk of suicide, potential anxiety or depression immediately to the mental health service and to inform the treating physician.
Analysis
Frequencies, central trends and scatter were estimated for the variables measured; associations were also analyzed between the suicide risk variable and the other variables, using the Epidat 4.0® and SPSS 18.0® analytical software packages.
The following calculations were performed in order to determine whether associations existed between the Quality of Life and Suicide Risk variables: Spearman correlations between the scores obtained in each of the sub-scales of the SF-36 and the score on the Plutchick Risk of Suicide scale; the Mann-Whitney U test to determine if there was a significant difference in the sub-scale scores between the groups with or without a risk of suicide, and with or without suicidal ideation.
The Chi square or Fisher's exact test were calculated in order to determine the association between anxiety, depression and suicide risk depending on whether the assumption of a minimum expected frequency of 5 was achieved in 80% of the boxes; additionally, correlations between scale scores were also calculated.
Results
Overall, 49 patients were assessed in a group made up mostly by females (63.3%), the majority of them of the income brackets 1 and 2, predominantly with primary school education, and housewives as their main occupation. The most frequent cause of pain was an underlying disease (46.9%), primarily fibromyalgia, failed back, and post-operative pain mainly from hernia repairs and back surgery. The mean age was 57.8 years (SD 14.3) with a range between 22 and 92, and the majority
were adults or elderly patients (Table 1). Patients failed to answer some items in some of the scales and, therefore, the results exclude the data lost in each case.

It is noteworthy that in all measurements, pain levels were mostly moderate or severe. When the highest level of pain perception was considered, the inter-quartile range showed that 75% of the subjects reported values above 7, considered severe; this means that over the previous week most of the subjects had experienced very high levels of pain (Table 2). Additionally, the frequency for each pain level was calculated (mild, moderate and severe), and the result was that 80% of the population assessed had experienced moderate or severe pain during the previous week (Table 3).

In terms of quality of life, there was an overall decline in work and daily activities. The mean value on the Physical Role scale (25.1) is quite low, and the median indicates that 50% of people perceived a functional decline three standard deviations below the expected mean (50). This indicates that patients had had problems with their work and daily activities over the previous month. In terms of physical functioning, this scale assesses mobility, ability to move and ability for physical exertion, and results show evidence of decline considering that the mean for the population (32.7) is almost two standard deviations below the expected mean. In terms of pain, the degree of limitation for daily activities was assessed in relation to pain intensity, resulting in a mean value of 32.6 and a median of 32.5. This means that these results are almost two standard deviations below the expected mean (50), a low score showing limitations in activities of daily living as a result of pain. The emotional role sub-scale assesses difficulties with work and other activities due to emotional issues, and the mean value was 22.7 (SD: 16), which places this result almost three standard deviations below the expected mean. This indicates that patients perceived that their emotional problems hindered work and other activities. For the physical component, a significant decline in physical function was identified, considering that the average score (33.8 with a SD of 9) is low(Table 4).
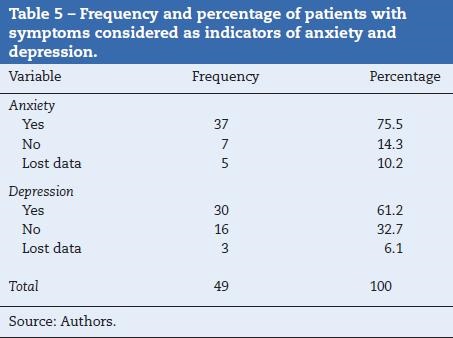
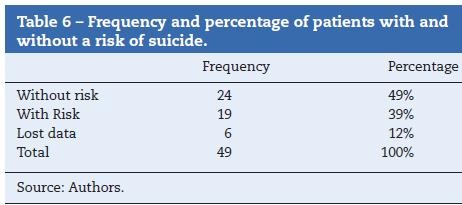
In terms of anxiety and depression symptoms, results show that the largest percentage of people that completed 100% of the test exceeded the cut-off point of 11, meeting the criteria required for suspected anxiety (75.5%) and depression (61.2%) (Table 5). Data analysis for the risk of suicide revealed that 39% of the population had a risk of suicide and 25% had suicide ideation (Table 6).
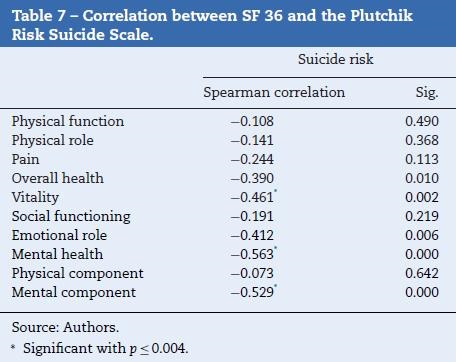
Analyses found significant inverse relationships between the suicide risk scale and the scores obtained for the SF-36 sub-scales of vitality, mental health, and the health component. Of these, a b association was found with mental health and the mental component, and the relationship with vitality was also an important consideration. This result shows that patients with feelings of anxiety and depression and with a greater decline in activity as a result of mental health have higher scores on the suicide risk scale, and this relationship may be similar, although not as b, among those who feel tired and exhausted most of the time (Table 7).
When the dichotomous analysis was applied to the results, a significant association was found between depression and the risk of suicide (Table 8), just like the correlation is high and significant when the direct scores obtained on the correlation scale are considered (Table 9). Regarding the anxiety variable, the dichotomous analysis did not find association between anxiety and the risk of suicide. However, when direct scale scores are considered, the correlation is intermediate and significant (Table 9).

Discussion
The study found a high prevalence of suicide risk and ideation, where 34% of the patients were found to have a risk of suicide, and 25% reported suicidal ideation. These findings are similar to those reported by Smith, Perlis & Haythornthwaite,13 who reported that 24% of their patients had suicidal ideation.
In terms of patient perception of quality of life, it was found that the majority of patients (median = 33.8) feel that they are limited in their ability to engage in physical activities such as long walks, shopping or climbing stairs, i.e. in their ability to move and engage in physical exertion; however they perceive that the compromise is much greater (median = 17.6) when it comes to their work or activities of daily living such as house work. This latter finding is quite significant because 75% had scores under 27, and considering that scores range from 0 to 100, a score of 27 on the Physical Role scale is evidence of significant compromise. The impact on the functional level might be related to the reported levels of pain, since according to the
results from authors like González et al.,14 Padierna et al.15 and Soler et al.,16 pain diminishes normal function ability in pain sufferers, which is consistent with the results of this study.
A high emotional impact was found, showing that most of the subjects assessed had a perception of difficulty with work and other activities of daily living due to emotional problems, and reported experiencing feelings of anxiety and depression most of the time. This result in the SF-36 correlates with scores on the HAD, where 75.5% of patients reported anxiety symptoms, including fear, nervousness and stress. Regarding depressive symptoms, it was found that 61.2% exceeded the cut-off point and could be suffering from this disorder. Authors like Truyols et al.3 assert that depression is one of the emotional responses most commonly associated with pain, and that symptoms may also manifest in the form of depression episodes; in that research, the authors also concluded that anxiety and depression symptoms are associated with a significant increase in pain perception.
Finally, the most important objective of this study was to determine the association between the variables measured and the risk of suicide in the patients. It was found that suicide risk is not related to the levels of perceived pain; however, there was no difference between the levels of pain or disability between depressed patients with our without suicidal intention. In this sense, it could be argued that it is not pain per se that might result in suicidal ideation or suicide risk among the subjects assessed, but rather the emotional impact of pain. In fact, all the significant associations were found between suicide risk and anxiety, depression, emotional role, mental health and mental component. Hence, it could be argued that pain has an emotional impact which, according to patient perception, affects normal functioning, and has an important relation with suicide risk.
Contextualization of findings and conclusions
Bearing in mind that this is an observational cross-sectional study, it is not possible to generalize, and causal factors or directionality of the associations cannot be determined. Despite precluding generalizations due to the particular type of sample, it is generally considered that the findings serve as an initial approach to the problem. The results point to the need of conducting future studies to determine mediators between pain and emotional states, since it appears that this understanding is critical in order to improve the effectiveness of the interventions and reduce risks associated with anxiety and depression, including suicide risk. Finally, we believe that it is important to include assessment and care of the mental component and emotional states in all protocols and care guidelines for chronic pain.
Funding
Universidad Manuela Beltrán, Hospital el Tunal E.S.E.
Conflicts of interest
The authors have no conflicts of interest to declare.
Acknowledgements
Universidad Manuela Beltrán, Faculty of Education, Humanities and Social Sciences, Psychology Program, Bogotá, Colombia. Hospital el Tunal - Empresa Social del Estado, Bogotá,Colombia.
1. Pedrajas J, Molino A. Bases neuromédicas del dolor. Clínica y Salud. 2008;19:277-93. [ Links ]
2. Castel-Bernal B, García-Bardon V, Tornero-Molina J. Evaluación psicológica en el dolor crónico. Reumatología Clínica. 2006;2:44-9. [ Links ]
3. Bonica JJ. Multidisciplinary/interdisciplinary pin programs. En: Bonica JJ, editor. The management of pain. Philadelphia: Lea & Febiger; 1990. p. 197-208. [ Links ]
4. Castro M, Kraychete D, Daltro C, Lopes J, Menezes R, Oliveira I. Comorbid anxiety and depression disorders in patients with chronic pain. Arq Neuropsiquiatr. 2009;67:982-5. [ Links ]
5. Pelechano V. Dolor crónico y trastornos de personalidad. Facultad de Psicología de la Universidad de la Laguna. Boletín de Psicología. 2005;84:59-76. [ Links ]
6. Brennan J, Sullivan M. Suicidal thoughts and behavior among adults with self-reported pain conditions in the national comorbidity survey replication. J Pain. 2008;9:1106-15. [ Links ]
7. Argimón J, Jiménez J. Métodos de investigación clínica y epidemiológica. España: Elsevier; 2004. [ Links ]
8. Balluerka N, Vergara AI. Diseños de investigación experimental en psicología. Madrid: Prentice-Hall; 2002. [ Links ]
9. Bonett DG, Wright TA. Sample size requirements for estimating pearson, kendall and spearma correlations. Psychometrika. 2010;65:23-8. [ Links ]
10. Lugo L, García H, Gómez C. Confiabilidad del Cuestionario de Calidad de Vida en Salud SF-36, 24 Medellín, Colombia:Revista de la Facultad Nacional de Salud Pública; 2006. p. 37-50. [ Links ]
11. Rico J, Restrepo M, Molina M. Adaptación y validación de la Escala Hospitalaria de Ansiedad y Depresión (HAD) en una muestra de pacientes con cáncer del Instituto Nacional de Cancerología de Colombia. Avances en Medición. 2005;3:73-86. [ Links ]
12. Rubio G, Montero I, Jáuregui J, Villanueva R, Casado MA, Marín JJ, et al. Validación de la escala de riesgo suicida de Plutchik en población española. Neurobiol.1998;61:143-52. [ Links ] [ Links ]
14. González A, Fernández C, García G, Soler J, Arce C, Cueto J. Quality of life parameters in terminal oncological patients in a home care unit. Psychology in Spain. 2002;6:68-76. [ Links ]
15. Padierna C, Fernández C, González A. Calidad de vida en pacientes oncológicos terminales, medida con el QL-CA-AFEX. Psicothema. 2002;14:1-8. [ Links ] [ Links ]
