










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkColombian Journal of Anestesiology
versão impressa ISSN 0120-3347
Rev. colomb. anestesiol. vol.42 no.1 Bogotá jan./mar. 2014
https://doi.org/10.1016/j.rca.2013.09.009
Scientific and technological research
Incidence of neurological complications and post-dural puncture headache after regional anesthesia in obstetric practice: A retrospective study of 2399 patients
Incidencia de complicaciones neurológicas y cefalea pospunción dural luego de anestesia regional en la práctica obstétrica: un estudio retrospectivo de 2399 pacientes
Domingos Dias Cicarelli *, Elke Frerichs, Fábio Ely Martins Benseñor
Anesthesiologist, Anesthesia Division of Hospital Universitario da Universidade de Sào Paulo, Sáo Paulo, Brazil
Corresponding author: Av. Prof. Lineu Prestes, 2565 - Butantã, São Paulo. E-mail address: dcicarelli@uol.com.br (D. Dias Cicarelli).
ARTICLE INFO
Article history: Received 30 November 2012 /Accepted 17 September 2013 / Available
online 4 December 2013
ABSTRACT
Introduction and objectives:Regional anesthesia provides excellent anesthesia and analgesia in obstetric patients, but has potential for complications such as post-dural puncture headache and permanent or transient nerve damage. This study aimed to describe the incidence of post-dural puncture headache and nerve damage in the obstetric population of a university hospital that was submitted to neuraxial blockades, comparing with the world literature, and identify risk factors.
Materials and methods: A retrospective cohort was performed including data collected in the records of post-anesthetic consults conducted during the year 2010. The main analysis was performed on the complaints of peripheral neurological deficits and headaches reported by patients, type of anesthesia and performed surgical procedures. A multiple regression analysis was performed to investigate the association between the onset of lower limb paresthesias and the length of stay of these patients in the gynecological position and other variables.
Results: A total of 2399 pregnant patients who had undergone neuraxial blockade were evaluated. Neurologic complications that occurred in these patients were divided into lower limb paresthesias (0.3%), transient radicular irritation (0.1%), and post-dural puncture headache (3%). The patients who stayed more than 60 min in gynecological position showed an odds ratio of evolution with lower limb paresthesias of 1.75 and patients who stayed more than 120 min showed an odds ratio of 2.1, but without statistical significance.
Conclusions:Patients submitted to neuraxial blockades and placed in gynecological position were more likely to evolve with lower limb paresthesias related to duration of this position.
Keywords: Anesthesia, Obstetrical Anesthesia, Conduction Analgesia, Anesthesia, Epidural Nerve Block.
RESUMEN
Introducción y objetivos: La anestesia regional brinda una excelente anestesia y analgesia en pacientes obstétricas, pero existe el potencial de complicaciones tales como la cefalea pospunción dural y lesión neurológica permanente o transitoria. El presente estudio pretende describir la incidencia de la cefalea pospunción dural y daño neurológico en la población obstétrica de un hospital universitario que fue tratada con bloqueo neuroaxial, en comparacióne con la literatura mundial, e identificar los factores de riesgo.
Material y métodos: Se hizo una cohorte retrospectiva incluyendo los datos recolectados apartir de los registros de consultas posanestesia durante el ano 2010. El análisis central se hizo en función de las quejas de déficit neurológico periférico y cefaleas reportadas porlos pacientes, el tipo de anestesia y el procedimiento quirúrgico realizado. Se aplicó un análisis de regresión múltiple para investigar la relación entre el inicio de parestesias de las extremidades inferiores y el tiempo en que permanecieron estas pacientes en posición ginecológica y otras variables.
Resultados:Se evaluaron en total 2399 pacientes embarazadas tratadas con bloqueo neuroaxial. Las complicaciones neurológicas que se presentaron en estas pacientes se dividieron en parestesias de las extremidades inferiores (0,3%), irritación radicular transitoria (0,1%) y cefalea pospunción dural (3%). Las pacientes que permanecieron más de 60 min en posición ginecológica mostraron un índice de probabilidades (odds ratio) de evolución con parestesia de las extremidades inferiores de 1,75, y las pacientes que estuvieron más de 120 min mostraron un índice de probabilidades de 2,1, pero sin significación estadística.
Conclusiones: Las pacientes que se sometieron a bloqueo neuroaxial y se colocaron en posición ginecológica tenían mayores probabilidades de evolucionar con parestesias de las extremidades inferiores por el tiempo que permanecieron en esta posición.
Palabras clave: Anestesia obstétrica, Anestesia de conducción, Analgesia, Anestesia epidural, Bloqueo nervioso.
Introduction and objectives
The neuraxial blockades (spinal anesthesia, epidural and combined spinal-epidural (CSE) anesthesia) are associated with lower morbidity and mortality compared to general anesthesia.1-5 These advantages are most relevant when the patients in question include obstetric patients. Changes in maternal physiology during pregnancy make neuraxial blockades a more safe technique than general anesthesia for these patients.6-10 However, some complications including neurological injury after regional anesthesia can be distressing to patients and families.11,12 The major neurological complications associated with neuraxial blockades, especially spinal anesthesia, epidural or CSE include: post-dural puncture headache (PDPH), nerve damage, and cardiovascular complications such as hypotension, bradycardia or cardiac arrest.13-40 The incidence of neurological complications caused by neuraxial blockades in our environment is not known. This information is essential to the adequacy of anesthetic teschniques to our patients, thus improving the quality of anesthesia performed, and preventing the possible complications.
This study aimed to describe the incidence of PDPH and other neurological complications in obstetric patients of a university hospital submitted to regional anesthesia and compare it with to the incidence of the world literature,1,6,13,15,17 as well as observing the relationship between neurological complications and identifiable risk factors in these patients.
Materials and methods
After approval by the Research Ethics Committee of our hospital, which waived informed consent, a retrospective cohort was performed with the data records of post-anesthetic consults conducted during the year 2010. These data refer to any symptom reported by obstetric patients submitted to neuraxial blockades on first day after anesthesia and its subsequent evolution and treatment. These patients underwent cesarean-section, forcipes and vaginal deliveries. Patients submitted to local or general anesthesia were excluded from this analysis. The main analysis was performed on the complaints of peripheral neurological deficits and/or headaches reported by patients, type of anesthesia and performed surgical procedure to which they were subjected. Incidence of these complications was calculated and compared with the incidence described in the literature, as well as the treatments described in our service and its efficiency. The association of peripheral neurologic deficits with length of stay of these patients in the gynecological position or other variables was investigated through a multiple regression analysis.
Results
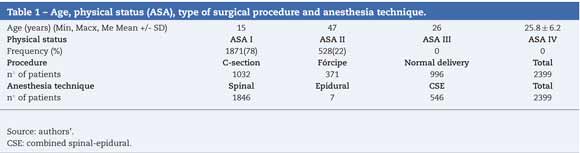
We evaluated 2399 pregnant patients who received neurax-ial blockade, on the first postoperative day. The average age and physical condition of patients are described in Table 1. Patients analyzed were submitted to epidural anesthesia, spinal anesthesia and CSE. The procedures were divided into cesarean section, vaginal deliveries and forcipes deliveries (Table 1).
Neurologic complications found in these patients were divided into lower limb paresthesias, transient radicular irritation, headaches (PDPH and other causes) and are described in Table 2.

The frequency of PDPH was calculated taking into account the total number of spinal anesthesias (PDPHSA) and PDPH frequency was calculated after CSE and epidural anesthesia too (PDPHEPI).
In the postoperative period, we evaluated 38 patients with complaints of headache. Of these, 6 patients had other causes of headache such as migraine,13 2 patients with anemia and 1 patient with sinusitis.
The relationship between the onset of paresthesias in the lower limbs and length of stay of patients in the gynecological position was investigated too. Among patients who stayed longer than 60 min in gynecological position when compared to patients who stayed less than 60 min in this position, we found an odds ratio of evolution with lower limb paresthe-sias of 1.75 (OR = 1.75 95% CI 0.34-9.04). Among the patients who stayed for more than 120 min in gynecological position when compared to patients who remained less than 120 min in this position, we found an odds ratio of evolution with lower limb paresthesias of 2.1 (OR = 2.1 95% CI 0.21-21.26). Other variables such as age, physical status, type of anesthesia (spinal, epidural or CSE) and type of delivery (forcipes, normal delivery) were not related to lower limb paresthesias.
Discussion
The incidence of PDPH after spinal anesthesia (PDPHSA), in our study, was 1.2% (22 patients), and of these, 19 patients (86%) were treated with analgesics and only 3 patients (14%) developed refractory headache to clinical treatment, after which they were submitted to blood-patch therapy. This frequency is higher than the reported incidence of 0.4% in world literature.39 The incidence of PDPH after epidural or CSE anesthesia (PDPHEPI) was 1.8% (10 patients). Of these, 7 patients (70%) responded to medical therapy with analgesics and steroids, and 3 patients (30%) received a blood-patch therapy. The incidence of PDPHEPI in the literature is estimated at around 0.35%,41 reporting efficacy of 96-98% of blood-patch.41-45 All our patients who underwent blood-patch had resolution of symptoms.
The patient population studied showed an incidence of neurological complications of 0.4% (2 patients with transient radicular irritation and 7 patients with lower limb paresthe-sias). In the literature reviewed, we found an incidence of neurological complications of 0.7%19 to 0.01%.1 Most recent data published by Vargas et al.26 described an incidence of neurological complications after spinal anesthesia that varying from 0.005% to 0.13%. Thus, we observed an incidence of neurological complications in our study compared with other studies, but with a trend toward higher incidence. One should take into account that these incidences may vary according to the different neurological complications: paresthesias, motor deficits. In our analysis we include three different types of block (spinal, epidural and CSE). The studies reviewed so far have included neurological complications of epidural or spinal anesthesia, but not CSE.1 This fact is due to these studies were from 1995 to 1998, during which time the CSE was not common practice in obstetric patients.46-49 Additionally, our service has anesthesiology residents in the first year of specialization that perform most of these blocks (under the supervision of attending physicians), and data from studies not analyzed to assess the presence or absence of medical expertise in such services.50 The resident physicians have greater difficulty to realize neuraxial blockades and also conduct an active search of complications in the post-anesthetic consult, being very rare in our service a patient with neurological post-anesthetic complication that was not diagnosed.50
Among the 2399 patients analyzed, 7 patients developed paresthesias, and 1 patient with sciatic nerve praxis and praxis of 6 patients with femoral nerve (all with spontaneous remission or after drug treatment). All patients who developed lower limb paresthesias were subjected to neuraxial blockades and then placed in gynecological position. This fact made us associate the appearance of paresthesias to position of these patients and not to the blockade of neuraxial performed. In our analysis, we found that the risk of paresthesia is greater the longer positioning in leggings, but without statistical significance. This lack of significance may be due to the low prevalence of paresthesias, requiring a larger number of patients analyzed.
Our study had another limitation: given that the follow-up period of patients was one day after anesthesia procedure, neurological complications or post-dural puncture headache that occurred after the second day could not be detected.
Obstetric patients undergoing neuraxial blockades and placed in gynecological position were more likely to evolve with lower limb paresthesias related to positioning time.
Funding: None.
Conflicts of interest: The authors have no conflicts of interest to declare.
Acknowledgement: Our acknowledgements to Dr. Nora Elizabeth Rojas Alvarez and Dr. German Collazos who helped us in the Spanish translation.
1. Brull R, McCartney CJL, Chan VWS, el-Beheiry H. Neurological complications after regional anesthesia: Contemporary estimates of risk. Anesth Analg. 2007;104:965-74. [ Links ]
2. Beattie WS, Badner NH, Choi P. Epidural analgesia reduces postoperative myocardial infarction: A meta-analysis. Anesth Analg. 2001;93:853-8. [ Links ]
3. Rodgers A, Walker N, Schug S, McKee A, Kehlet H, van Zundert A, et al. Reduction of postoperative mortality and morbidity with epidural and spinal anaesthesia: Results from overview of randomized trials. BMJ. 2000;321:1493. [ Links ]
4. Urwin SC, Parker MJ, Griffiths R. General versus regional anaesthesia for hip fracture surgery: A meta-analysis of randomized trials. Br J Anaesth. 2000;84:450-5. [ Links ]
5. Wu CL, Hurley RW, Anderson GF, Herbert R, Rowlingson AJ, Fleisher LA. Effect of postoperative epidural analgesia on morbidity and mortality following surgery in medicare patients. Reg Anesth Pain Med. 2004;29:525-33. [ Links ]
6. Loubert C, Hinova A, Fernando R. Update on modern neuraxial analgesia in labour: A review of the literature of the last 5 years. Anaesth. 2011;66:191-217. [ Links ]
7. Blanshard HJ, Cook TM. Use of combined spinal-epidural by obstetric anesthetists. Anaesth. 2004;59:922-3. [ Links ]
8. Rawal N. Combined spinal-epidural anaesthesia. Curr Opin Anaesthesiol. 2005;18:518-21. [ Links ]
9. Preston R. The role of combined spinal epidural analgesia for labour: Is there still a question? Can J Anesth. 2007;54:9-14. [ Links ]
10. Cortes CA, Sanchez CA, Oliveira AS, Sanchez FM. Labor analgesia: A comparative study between combined spinal-epidural anesthesia versus continous epidural anesthesia. Rev Bras Anestesiol. 2007;57:39-51. [ Links ]
11. Abrao KC, Francisco RPV, Miyadahira S, Cicarelli DD, Zugaib M. Elevation of uterine basal tone and fetal heart rate abnormalities after labor analgesia: A randomized controlled trial. Obstet Gynecol. 2009;113:41-7. [ Links ]
12. Cicarelli DD, Silva RV, Frerichs E, Pagnocca ML. Combined spinal-epidural for labor analgesia: Does the addition of sufentanil to the local anesthetic influence Apgar scores of the newborn? Rev Bras Anestesiol. 2007;57:272-9. [ Links ]
13. Jadon A. Complications of regional and general anaesthesia in obstetric practice. Indian J Anaesth. 2010;54: 415-20. [ Links ]
14. Cooper G, McClure J. Maternal deaths from anesthesia. An extract from Why Mothers Die 2000-2002, the Confidential Enquiries into Maternal Deaths in the United Kingdom: Chapter 9: Anaesthesia. Br J Anaesth. 2005;94:417-23. [ Links ]
15. Choi PT, Galinski SE, Takeuchi L, Lucas S, Tamayo C, Jadad AR. PDPH is a common complication of neuraxial blockade in parturients: A meta-analysis of obstetrical studies. Can J Anaesth. 2003;50:460-9. [ Links ]
16. American Society of Anesthesiologists Task Force on Obstetric Anesthesia. Practice guidelines for obstetric anesthesia: An updated report by the American Society of Anesthesiologists Task Force on Obstetric Anesthesia. Anesthesiol. 2007;106:843-63. [ Links ]
17. Tanaka PP, Tanaka MAA. Sintomas neurológicos transitónos após raquianestesia. Rev Bras Anestesiol. 2004;54:108-13. [ Links ]
18. Auroy Y, Benhamou D, Barques L, Ecoffey C, Falissard B, Mercier FJ, et al. Major complications of regional anesthesia in France: The SOS regional anesthesia hotline service. Anaesthesiol. 2002;97:1274-80. [ Links ]
19. Ganem EM, Castiglia YMM, Vianna PTG. Complicares neurológicas determinadas pela anestesia subaracnóidea.Rev Bras Anestesiol. 2002;52:471-80. [ Links ]
20. Reynolds F. Damage to the conus medullaris following spinal anaesthesia. Anaesthesia. 2001;56:235-47. [ Links ]
21. Puolakka R, Haasio J, Pitkanem M, Kallio M, Rosenberg PH. Technical aspects and postoperative sequelae of spinal and epidural anesthesia: A prospective study of 3230 orthopedic patients. Reg Anesth Pain Med. 2000;25:488-97. [ Links ]
22. Imbelloni LE, Sobral MGC, Carneiro ANG. Cefaléia pós-raquianestesia e o desenho das agulhas. Rev Bras Anestesiol. 2001;51:43-52. [ Links ]
23. Horlocker TT, Wedel DJ. Neurologic complications of spinal and epidural anesthesia. Reg Anesth Pain Med. 2000;25:83-98. [ Links ]
24. Mendes FF, Luft A, Gomes LC. Déficit neurológico após bloqueio espinhal. Relato de caso. Rev Bras Anestesiol. 1999;49:38-9. [ Links ]
25. Barbosa JS, Rabello RP, Saraiva RA, Vieira ZEG, Rossi AMC. Lesao de nervo periférico nem sempre é complicacao da anestesia regional. Rev Bras Anestesiol. 1992;42:239-42. [ Links ]
26. Navarro Vargas JRN, Luquetta Berrio JAL, Tejada López ET. Lesión nerviosa periférica secundaria a anestesia regional subaracnoidea en paciente ginecobstétrica. Rev Colomb Anestesiol. 2009;37:71-8. [ Links ]
27. Wlody D. Complications of regional anesthesia in obstetrics. Clin Obstet Gynecol. 2003;46:667-78. [ Links ]
28. Greensmith JE. Complications of regional anesthesia. Curr Opin Anaesthesiol. 2006;19:531-7. [ Links ]
29. Turnbull D, Shepherd B. Post-dural puncture headache: Pathogenesis, prevention and treatment. Br J Anaesth. 2003;91:718-29. [ Links ]
30. Lorri AL, Karen LP. Injuries associated with regional anesthesia in the 1980s and 1990s: A closed claims analysis. Anesthesiol. 2004;101:143-52. [ Links ]
31. Quintero IF, Candamil A, Mantilla JHM, Medina H, Cadena FA. Intracranial hypotension syndrome: A post dural puncture headache? Rev Colomb Anestesiol. 2013;41:57-60. [ Links ]
32. Grande PO. Mechanisms behind postspinal headache and brain stem compression following lumbar dural puncture â a physiological approach. Acta Anaesthesiol Scand. 2005;49:619-26. [ Links ]
33. Diaz JH. Epidemiology and outcome of postdural headache management in spontaneous intracranial hypotension. Reg Anesth Pain Med. 2001;26:293-6. [ Links ]
34. Gonzalez CEM, Enriquez LE, Cruz CA. Arachnoiditis following spinal anesthesia for cesarean section. Rev Colomb Anestesiol. 2012;40:150-2. [ Links ]
35. Moen V, Irestedt L. Neurological complications following central neuraxial blockades in obstetrics. Curr Opin Anaesthesiol. 2008;21:275-80. [ Links ]
36. Aldrete JA. Neurologic deficits and arachnoiditis following neuroaxial anesthesia. Acta Anaesthesiol Scand. 2003;47: 3-12. [ Links ]
37. Rice I, Wee MY, Thomson K. Obstetric epidurals and chronic adhesive arachnoiditis. Br J Anaesth. 2004;92:109-20. [ Links ]
38. Wong CA, Scavone BM, Dugan S, Smith JC, Prather H, Ganchiff JN, et al. Incidence of postpartum lumbosacral spine and lower extremity nerve injuries. Obstet Gynecol. 2003;101:279-88. [ Links ]
39. Villar GCP, Roas C, Cappelli EL, Rosa MCR. Incidencia de cefaléia pós-raquianestesia em pacientes obstétricas com o uso de agulha Whitacre calibre 27G. Experiencia com 4570 casos. Rev Bras Anestesiol. 1999;49:110-2. [ Links ]
40. Ben-David B, Rawa R. Complications of neuraxial blockade. Anesthesiol Clin North America. 2002;20:669-93. [ Links ]
41. Neves JFNP, Vieira VLR, Saldanha RM, Vieira FAD, Neto MC, Magalhaes MG, et al. Uso da hidrocortisona no tratamento e na prevencao da cefaléia pós-puncao da dura-máter. Relato de casos. Rev Bras Anestesiol. 2005;55:343-9. [ Links ]
42. Davignon KR, Dennehy KC. Update on postdural puncture headache. Int Anesthesiol Clin. 2002;40:89-102. [ Links ]
43. Safa-Tisseront V, Thormann F, Malassine P, Henry M, Riou B, Coriat P, et al. Effectiveness of epidural blood patch in the management of post-dural puncture headache. Anesthesiol. 2001;95:334-9. [ Links ]
44. Cousins MJ, Brazier D, Cook R. Intracranial hypotension caused by cervical cerebrospinal fluid leak: Treatment with epidural blood patch. Anesth Analg. 2004;98:1794-7. [ Links ]
45. Cicarelli DD, Stábile Jr SL, Guimaraes CM, Nishida MM. Cefaléia pós-puncao de duramáter em paciente HIV positivo: qual o melhor tratamento. Rev Bras Anestesiol. 2000;50:306-8. [ Links ]
46. Kleinman W. Obstetric anesthesia. En: Morgan Jr GE, Mikhail MS, Murray MJ, editores. Clinical Anesthesiology. 3rd ed. New York: McGraw-Hill Companies Inc.; 2002. p. 819. [ Links ]
47. Santos AC, O'Gorman DA, Finster M. Obstetrical Anesthesia, Chapter 43. En: Barach PG, Cullen BF, Stoelting RK, editores. Clinical Anesthesia. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2001. p. 1141. [ Links ]
48. Hall BA, Chantigian RC. Obstetric Physiology and Anesthesia, Chapter 8. En: Hall BA, Chantigian RC, editores. Anesthesia, a Comprehensive Review. 4th ed. Missouri: Mosby Elsevier;2010. p. 208. [ Links ]
49. Martins CEC, Cangiani LM, editores. Tratado de Anestesiologia. 7th ed. Sao Paulo: Atheneu; 2011. p. 2283. [ Links ]
50. Rodrigues FR, Brandao MJN. Anestesia regional para cesariana em gestantes obesas: estudo retrospectivo. Rev Bras Anestesiol. 2011;61:13-20. [ Links ]
