










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkColombian Journal of Anestesiology
versión impresa ISSN 0120-3347
Rev. colomb. anestesiol. vol.42 no.3 Bogotá jul./sep. 2014
https://doi.org/10.1016/j.rca.2014.02.005
Scientific and Technological Research
Sensitivity, specificity and predictive values of the Goldman, Detsky and Lee cardiac indices
Sensibilidad, especificidad y valores predictivos de los índices cardíacos de Goldman, Detsky y Lee
Hernán Javier Pantoja Muñoza, Humberto Fernández Ramosb,*, William Leandro Guevara Tovara
a Specialist in Anaesthesiology and Resuscitation, Hospital Universitario Manuel Ascunce Domenech, Carretera Central Oeste km 4½, Camagüey, Cuba
b Specialist in Anaesthesiology and Resuscitation, Masters in Medical Emergencies, Professor and Instructor at Universidad de Ciencias Médicas de Camagüey, Hospital Universitario Manuel Ascunce Domenech, Carretera Central Oeste km 4½, Camagüey, Cuba
* Please cite this article as: Muñoz HJP, Ramos HF, Tovar WLG Sensibilidad, especificidad y valores predictivos de los índices cardiacos de Goldman, Detsky y Lee. Rev Colomb Anestesiol. 2014;42:184-191.
* Corresponding author at: Calle Bellavista No. 322, Entre calles Artola y Fernando de Zayas, Reparto La Vigía, Código Postal, 70200 Camagüey, Cuba.
E-mail address: mrd@finlay.cmw.sld.cu (H.F. Ramos).
Article info
Article history: Received 12 July 2013 Accepted 16 February 2014 Available online 21 May 2014
Abstract
Introduction: Timely recognition of perioperative risk variables helps predict morbidity and mortality frequency, as well as adopt measures to reduce complications. Several risk scores have been developed for this purpose in patients with cardiovascular disease.
Objective: To determine the sensitivity, specificity and predictive values of the Goldman, Detsky and Lee cardiac risk indices for non-cardiac surgery.
Methods: Observational, analytical, longitudinal prospective study of the total number of patients with cardiovascular disease undergoing non-cardiac surgery between January 2011 and January 2013 at Hospital Universitario Manuel Ascunce Domenech in Camagüey. The sample consisted of 88 patients included in the universe of patients who met the inclusion criteria. The variables studied were: age, gender, type of surgery, type of complication, and the presence or absence of complications in relation to the risk assessed on the basis of the Goldman, Detsky and Lee indices. The sensitivity, specificity and predictive value test was applied.
Results: There was a predominance of males in patients over 70 years of age coming for orthopaedic surgery; cardiac arrhythmiawas the main complication. High-risk patientswere a frequent finding and the majority suffered complications.
Conclusions: The Goldman and Detsky indices showed high sensitivity and specificity, while the Lee index showed higher positive predictive value. However, the three predictive indices must be applied in order to optimize cardiac risk stratification in non-cardiac surgery.
Keywords: Preoperative cardiovascular risk; Goldman index; Detsky index; Lee index.
Resumen
Introducción: Reconocer oportunamente las variables de riesgo perioperatorio permite predecir la frecuencia de morbimortalidad, así como tomar medidas a fin de reducir complicaciones. Para ello se han creado varias escalas de riesgo en pacientes portadores de enfermedad cardiovascular.
Objetivo: Determinar la sensibilidad, la especificidad y los valores predictivos de los índices de riesgo cardíaco de Goldman, Detsky y Lee para cirugía no cardíaca.
Método: Se realizó un estudio observacional, analítico, longitudinal y prospectivo del total de pacientes portadores de enfermedad cardiovascular con enfermedad quirúrgica no cardíaca en el período comprendido entre enero de 2011 y enero de 2013 en el Hospital Universitario Manuel Ascunce Domenech de la ciudad de Camagüey. La muestra estuvo constituida por 88 pacientes comprendidos en el universo que cumplieron con los criterios de inclusión. Las variables estudiadas fueron: edad, sexo, tipo de cirugía, tipo de complicación, y la presencia o no de estas en relación con el riesgo catalogado según los índices de Goldman, Detsky y Lee. Se aplicó prueba de sensibilidad, especificidad y valores predictivos.
Resultados: Predominaron los pacientes mayores de 70 años, el sexo masculino, la cirugía ortopédica; la arritmia cardíaca fue la principal complicación. Fue frecuente encontrar pacientes de alto riesgo, en los cuales la mayoría sufrieron complicaciones.
Conclusiones: Los índices de Goldman y Detsky mostraron alta sensibilidad y especificidad, y el índice de Lee, mayor valor predictivo positivo. No obstante, deben aplicarse los 3 índices predictivos para lograr una óptima estratificación del riesgo cardíaco en cirugía no cardíaca.
Palabras clave: Riesgo cardiovascular preoperatorio; Índice de Goldman; Índice de Detsky; Índice de Lee.
Introduction
Cardiovascular disease is the primary cause of death in Cuba and in the world.1 As far as the practice of surgery is concerned, anaesthetists and surgeons alike are faced with an increasing number of elderly patients with underlying cardiovascular disease.2,3 The incidence of myocardial ischaemia in high-risk patients undergoing non-cardiac surgery is close to 40% during the perioperative period.4,5 The incidence of myocardial infarction and death during non-cardiac surgery ranges between 1% and 5%.6-8
These facts have led researchers and physicians to focus on the study of perioperative cardiovascular risk in order to avoid or reduce the occurrence of cardiovascular complications.9,10 In this regard, the American College of Cardiology and the American Heart Association (ACC/AHA) have created the Guidelines for Cardiovascular Assessment and Perioperative Care, which offer a sound basis for the stratification of surgical patients using specific cardiovascular risk factors and functional status assessment. They propose a series of decision-making algorithms related to the workup and preoperative management of these patients.11-13
Timely recognition of the cardiovascular status and identification of risk factors that may adversely affect the patient during surgery help stratify individual risk. This will be taken into consideration for deciding on the convenience or not of the surgery, the diagnostic and therapeutic plan, and other perioperative actions in order to try to avoid the occurrence of any serious cardiovascular complications.14-17
To achieve this goal, several preoperative assessment scales are available to help predict the risk of cardiovascular complications.18-22 Since the 1960s, efforts have been made to establish and unify clinical data that may help predict the risk of coronary events in patients undergoing surgery, using uni-variate and multivariate analyses such as the Goldman23,24, Detsky25 and Lee26,27 indices.
If a multifactorial cardiac risk index with a high predictive power is an effective tool to anticipate complications and adverse events in cardiac patients undergoing urgent non-cardiac surgery, then it can be used to optimize perioperative management and lead to more reassuring postoperative outcomes.
Our objective is to determine the sensitivity, specificity and predictive values of these three multifactorial cardiac risk indices for non-cardiac surgery.
Methods
We conducted an observational, analytical, longitudinal and prospective study of the total number of patients with cardiovascular disease and non-cardiac surgical pathology seen between January 2011 and January 2013 at Hospital Manuel Ascunce Domenech in the city of Camagüey, in order to determine the predictive value of the Goldman, Detsky and Lee multifactorial cardiac risk indices in non-cardiac surgery.
Universe
The total number of patients with cardiovascular disease scheduled for urgent non-cardiac surgery.
Sample
All of the patients in the universe who met the inclusion criteria.
Inclusion criteria for the sample
- Patients over 30 years of age.
- Patients with underlying cardiovascular disease undergoing non-cardiac surgical procedures.
- Urgent surgery.
Exclusion criteria
- Patients in whom the quantitative assessment of each of the risk indices was not performed due to the lack of some clinical or paraclinical information required for scoring.
- Patients in whom it was not possible to determine whether there were any intraoperative or postoperative complications.
Variables studied
Age, gender, type of surgery, incidence and type of complications, risk stratification according to the Goldman, Detsky and Lee indices, relationship between the risk and the complications, sensitivity, specificity, positive and negative predictive values of the three cardiac risk indices.
Operational definitions
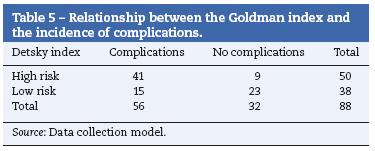
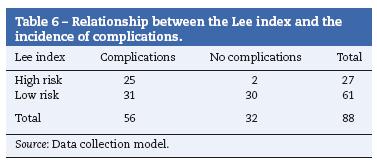
High risk: Patients with a Goldman score greater than 12 points, Detsky greater than 15, and Lee greater than 2 points.
Low risk: Patients with a Goldman score between 0 and 12 points, Detsky lower than or equal to 15, and Lee lower than or equal to 2 points.
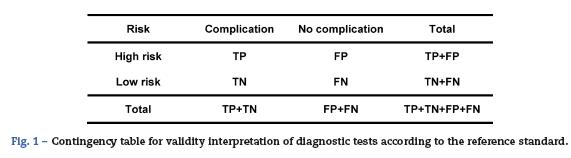
True positive (TP): Set of patients correctly predicted as being high risk.
False positive (FP): Set of patients wrongly predicted as high risk.
True negative (TN): Set of patients wrongly predicted as low risk.
False negative (FN): Set of patients correctly predicted as being low risk.
Sensitivity (S): Number of patients correctly predicted as being high risk (high probability of complications) out of the total high-risk patients (those who actually had complications). Expressed as percentage (S = TP/TP+ TN).
Specificity (Sp): Number of patients correctly predicted as low risk (low probability of complications) out of the total low risk patients (those who actually did not have complications). Expressed as percentage (Sp = FN/FP + FN).
Positive predictive value (PPV): Number of patients correctly predicted as high risk (high probability of complications) out of the total number of patients predicted as high risk. Expressed in percentage (PPV=TP/TP+ FP).
Negative predictive value (NPV): Number of patients correctly predicted as low risk (low probability of complications) out of the total number of patients predicted as low risk. Expressed in percentage (NPV = FN/FN+TN).
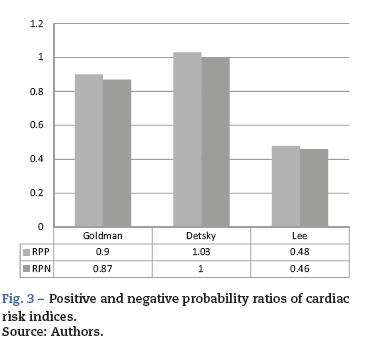
Positive probability ratio (PPR): It is the result of dividing (quotient) the probability of a high cardiovascular risk patient presenting cardiac complications by the probability of a low cardiovascular risk patient presenting cardiac complications (sensitivity/1 - specificity).
Negative probability ratio (NPR): It is the result of dividing (quotient) the probability of a high cardiovascular risk patient not presenting cardiac complications by the probability of a low cardiovascular risk patient not presenting cardiac complications (1 - sensitivity/specificity).
Data collection
Data were obtained using a data collection model. The primary registry model was developed in accordance with criteria from experts in information systems and anaesthe-siology, adapting it according to the proposed objectives. Patients with underlying cardiac disease coming for urgent surgery were identified by means of preoperative assessment, and risk stratification was made using the scales mentioned above, according to the scores. Patients were followed during the postoperative period until their hospital discharge or death, in order to determine if there were any complications, including their severity, and the findings were recorded in the primary registry or survey model. No additional preoperative pharmacological interventions were used, because the goal was to show evidence of the real risk of the underlying cardiac disease and the non-cardiac procedure.
Processing of the information
The collected data were processed using the SPS statistical software package for Windows 10.0; descriptive and inferential statistics were used; the sensitivity, specificity, predictive value and probability ratio tests were applied to the three cardiac risk indices, with a 95% confidence interval (CI). The results were expressed in the form of tables and figures.
Ethical considerations
Research is the main source of evidence on treatment efficacy. Consequently, national and international professional associations have created guidelines for research on healthy and diseased individuals using different deontological and legal codes. We considered the Nuremberg Code, which focuses on the rights of subjects participating in research studies and establishes consent as an essential element in human research; and the Helsinki Declaration approved in 1964 by the World Medical Assembly for the regulation of clinical research ethics on the basis of the physician's moral integrity and responsibility. The protocol for the following research was approved by the Institutional Review Board.
Results
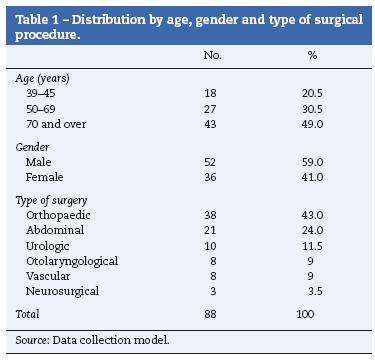
Table 1 shows patient distribution by age, gender and type of surgical procedure, with a predominance of patients over 70 years of age, representing 49%. There was a higher frequency of male patients proposed for non-cardiac procedures (59%), compared to female patients (41%). There was a high frequency of orthopaedic procedures (43%), followed by general abdominal surgery (24%).
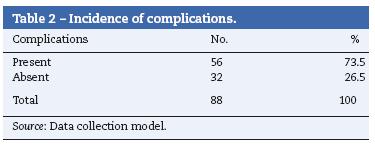
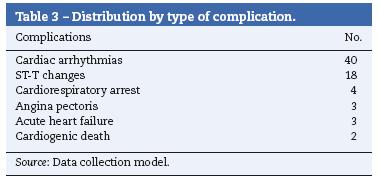
Tables 2 and 3, respectively, show the incidence of complications and the distribution of the study patients according to the type of complication during and after the surgical procedure. There was a predominance of complications in 56 patients, representing 73.5%, and the most frequent were cardiac arrhythmias, followed by ST segment changes.
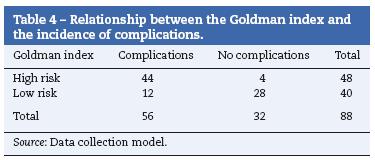
In terms of the relation among the different multifactorial cardiac risk indices and the presence or absence of complications (Tables 4-6), there is consistency with the Goldman and Detsky indices, in such a way that the highest frequency of complications was observed in high risk patients (44 and 41), and the absence of complications was seen in low risk patients (28 and 23), respectively. As for the Lee index, the presence of complications was high in low risk patients compared to the absence of complications (31 and 30), respectively (1:1 ratio), when it was expected to behave similarly to the other two indices, that is to say, that low risk should be consistent with a low frequency of complications and vice versa (Fig. 1).
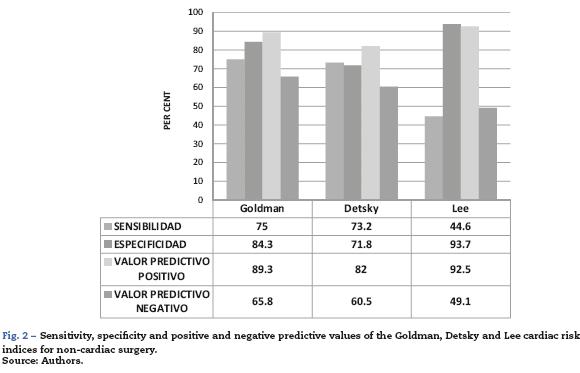
The sensitivity, specificity and positive and negative predictive value analysis is shown in Fig. 2. The Goldman and Detsky multifactorial cardiac risk indices were similar for sensitivity, specificity and negative predictive value, reflecting their ability to predict complications in a high percentage of high risk patients; however, the Lee index showed low sensitivity and negative predictive value, with high specificity and positive predictive value results. We conclude that patients in whom the Lee index is applied may be classified wrongly as low risk and suffer cardiac complications.
The probability or likelihood ratios compare the probability of finding the result of the diagnostic test (positive or negative) in patients with the disease or patients suffering the event of interest with the probability of finding this same result in people without the disease or the event of interest. The results of these tests are shown in Fig. 3.
Discussion
Cardiac complications are among the most significant risks for patients taken to non-cardiac surgery.28,29 A prospective study published in 1977 evaluated 1001 patients of this type, older than 40 years of age, and the mean risk of cardiac complications or postoperative cardiac death was 5.8%.23,24,30 In unselected patients with a mean age of 40, acute myocardial infarction (AMI) occurred in 1.4% and cardiac death in 1%.31-33 On the other hand, with the ageing population, surgical complexity in elderly patients has increased.11,34
Atherosclerosis is the etiological factor responsible for coronary artery disease (CAD) in more than 95% ofcases. Sudden death runs parallel with the occurrence of myocardial ischaemia in males after the fourth decade of life, in a proportion, according to different authors, of up to 7:1 with females. This difference is explained by the protective role of menar-che in women. In the seventh decade of life, atherosclerosis affects both sexes in a 2:1 proportion.35,36
The complexity of the surgical procedure may be, in and of itself, the most important predictive factor for postoperative morbidity in many patients.37Cardiac risk may be stratified according to the type of surgical procedure to be performed. The length and type of surgery have a significant influence on the risk of perioperative cardiac complications.38,39 By definition, cardiac death or non-fatal myocardial infarction average is greater than 5% in high risk surgical procedures, between 1 and 5% in intermediate risk procedures, and less than 1% in low risk procedures.11 Most of the studies on postoperative cardiac complications have been conducted in groups of patients selected on the basis of risk. For that reason, it is difficult to generalize the results to the population requiring the majority of the surgical interventions.30,40
Intraoperative arrhythmias are among the most frequent complications in the practice of anaesthesia. Their incidence is close to 70% in non-cardiac surgery and they may reflect a serious event such as myocardial ischaemia, cerebro-vascular alteration or cardiac arrest, although they are more often benign transient disorders that may resolve spontaneously or with simple interventions.41
Sudden electrocardiographic (EKG) ST segment changes may mean, in a myocardium where flow and demand are on the limit, the manifestation of an acute coronary syndrome (infarction, angina) or plaque rupture in a patient with atherosclerotic disease. However, in a good proportion, these changes are transient and do not result in irreversible damage to the cardiac muscle or in low output state.42
In a study in 1977, Goldman et al. developed the first multifactorial risk index specifically related to cardiac complications, including nine independent risk factors.23,24 Detsky et al. updated that index in 1986, adding the CAD pretest probability, angina stratification, and time cycle for AMI and heart failure.25 The preoperative cardiac risk factor index showed a clear correlation with subsequent cardiac events: of the low risk patients, only 0.9% had cardiac events; of the high risk patients, 78% had a life-threatening cardiac event or cardiac death.23,24 The end points used by Detsky et al. in their analysis included events such as unstable angina and left ventricular insufficiency, which could complement the indicative value of preoperative risk factors in CAD assessment. The modified cardiac risk index still needs prospective revalidation.25
The Lee index,26,27 a modification of the original Goldman index, is considered by many physicians and researchers as the best of all indices available for predicting cardiac risk in non-cardiac surgery. At present, this is the model most widely used for risk assessment in non-cardiac surgery. Multifactorial indices that combine and assign relative importance to many clinical parameters are more useful than any isolated factor for determining cardiovascular risk in the individual patient, or for determining the overall morbidity risk.43,44
The Goldman index has a negative predictive value of 96.8% and, therefore, it is an excellent tool for ruling out coronary heart disease. However, with a positive predictive value of 21.6%, it is less adequate for diagnosing patients who have the disease.23,24 This latter value is not consistent with the population in our study, where the positive predictive value of the Goldman index was high (89.3%). In 1999, Lee et al.,26 reviewed the efficacy of several clinical risk factors in patients undergoing elective non-cardiac surgery. They found that the efficacy of the Goldman risk index as well as the Detsky modified cardiac risk index was similar in predicting serious cardiac complications. However, after reviewing and validating the Goldman risk index, its predictive value improved substantially.45
In a retrospective analysis of the Goldman and Detsky cardiac risk indices in elective non-cardiac surgery, an attempt was made to compare the effectiveness of these two cardiac indices when used to predict perioperative cardiovascular events; however, there were no major cardiovascular complications, precluding the comparison.46
The Goldman index showed high specificity (93.7%) and positive predictive value (90.0%) in a sample assessed by Fernández et al.43
Some important considerations about the potential usefulness of preoperative cardiac risk indices are worth noting. A low risk classification index does not exclude a patient from the perioperative cardiac risk but rather points to a low probability of a cardiac event.47 The optimum use of cardiac risk indices may be that of modifying the initial risk and not predicting the absolute risk for complications. Multifac-torial indices used to assess perioperative risk in patients with underlying cardiac disease faced with a non-cardiac intervention take into consideration several clinical and par-aclinical parameters that are assessed differently. Although some risk indicators are overestimated when compared to others, numerous studies have shown that they all have acceptable sensitivity and specificity47-50; however, it is important to recognize that results vary and are subject to the prevalence of cardiac disease in the type of population studied.
In this research, we conclude that the Goldman and Detsky indices showed high sensitivity and specificity, while the Lee index had a higher positive predictive value. However, all three predictive indices must be applied in order to achieve optimal cardiac risk stratification for non-cardiac surgery.
Funding
None.
Conflict of interests
None.
References
1. Seuc AH, Domínguez Alonso E, Torres Vidal RM, Varona Pérez P. Algunas precisiones acerca de la mortalidad por enfermedades cardiovasculares en Cuba. Rev Cubana de Salud Pública. 2011;37:19-33. [ Links ]
2. De la Cruz Pérez C, Foncea ME, Mañas JC, Caparrós AC, Pérez FP, Pardo JS, et al. Morbimortalidad cardiaca postoperatoria en pacientes ancianos de alto riesgo intervenidos de cirugía mayor no cardiaca. Rev Esp Anestesiol Reanim. 1999;46:4. [ Links ]
3. Haldeman GA, Croft JB, Giles WH, Rashidee A. Hospitalization of patients with heart failure: National Hospital Discharge Survey, 1985 to 1995. Am Heart J. 1999;137:352. [ Links ]
4. Hernandez AF, Whellan DJ, Stroud S, Sun JL, O'Connor CM, Jollis JG. Outcomes in heart failure patients after major noncardiac surgery. J Am Coll Cardiol. 2004;44: 1446-53. [ Links ]
5. Mangano DT, Browner WS, Hollenberg M, London MJ, Tubau JF, Tateo IM. Association of perioperative myocardial ischemia with cardiac morbidity and mortality in men undergoing noncardiac surgery. N Engl J Med. 1990;323:1781-8. [ Links ]
6. Cassem Ramos G. Aspectos relevantes de la enfermedad arterial coronaria en candidatos a la cirugía no cardiaca. Rev Bras Anestesiol. 2010;60:366-9. [ Links ]
7. Baena-Díez JM, Vidal-Solsona M, Byram AO, González-Casafont I, Ledesma-Ulloa G, Martí-Sans N. Epidemiología de las enfermedades cardiovasculares en atención primaria. Rev Esp Cardiol. 2010;63:1261-9. [ Links ]
8. Ibacache M, Pedrozo Z, Fernández C, Sánchez G, Lavandero S. Infarto perioperatorio en cirugía no-cardíaca y dexmedetomidina. Rev Chil Cardiol. 2010;29: 100-16. [ Links ]
9. Luna Ortíz P, González Chong O, Molina Méndez FJ, Romero Borja J, Fernández Rivera B, Lesprón Robles MC, et al. Evaluación pre-operatoria del paciente cardiópata para cirugía no cardiaca. Rev Mex Anest. 1996;19:128-45. [ Links ]
10. Morse KJ. Pacientes quirúrgicos con problemas cardíacos. Nursing (ed española). 2009;27:26-31. [ Links ]
11. Fernández J, Litvan H. Guías de la AHA/ACC sobre evaluación y cuidado preoperatorio cardiovascular en cirugía no cardiaca. ¿Qué hay de nuevo? Rev Esp Anestesiol Reanim. 2008;55:595-6. [ Links ]
12. Grupo de Trabajo de la Sociedad Europea de Cardiología. Guía de práctica clínica para la valoración del riesgo cardiaco preoperatorio y el manejo cardiaco perioperatorio en la cirugía no cardiaca. Rev Esp Cardiol. 2009;62:1467-523. [ Links ]
13. Fleisher L. Cardiac risk stratification for non-cardiac surgery: Update from the ACC/AHA 2007 guidelines. Cleve Clin J Med. 2009;76:9-15. [ Links ]
14. Poldermans D, Schouten O, Bax J, Winkel TA. Reducing cardiac risk in non-cardiac surgery: evidence from the decrease studies. Eur Heart J. 2009;11:9-14. [ Links ]
15. Fernández Ramos H, Pozo Romero JA, Correa Borrell M. Prevención de complicaciones perioperatorias en pacientes con enfermedades cardiovasculares. Rev Cubana de Anestesiología y Reanimación. 2012;11:211-9. [ Links ]
16. Fischer S, Bader AM, Sweitzer B. Valoración preoperatoria. En: Miller, editor. Miller Anestesia. 7.a ed. España: Elsevier; 2010. p. 762-829. [ Links ]
17. Poldermans D, Hoeks SE, Feringa HH. Pre-operative risk assessment and risk reduction before surgery. J Am Coll Cardiol. 2008;51:1913-24. [ Links ]
18. Alonso-Mercado JC, Molina-Mendez FJ, Chuquiure-Valenzuela EJ, Ochoa-Pérez V, Soto-Nieto G, Baranda-Tovar FM, et al. Valoración preoperatoria en cirugía cardiovascular. Arch Cardiol Mex. 2011;81:9-15. [ Links ]
19. Chuquiure Valenzuela E. Valoración del riesgo cardiovascular en enfermos cardiópatas, que serán sometidos a cirugía no cardíaca. Rev Mex Anetesiol. 2011;34:44-8. [ Links ]
20. Fong Mata ER, Elguero Pineda E. Valoración prequirúrgica en cirugía no cardiológica. Índice de Eagle versus ASA. Med Interna Méx. 2001;17:18-23. [ Links ]
21. Fuentes Díaz Z. Protocolo preoperatorio para estimar morbilidad y mortalidad quirúrgicas. Un enfoque social. Humanidades Médicas. 2012;1:22-36. [ Links ]
22. Kheterpal S, O'Reilly M, Englesbe MJ, Rosenberg AL, Shanks AM, Zhang L. Preoperative and intraoperative predictors of cardiac adverse events after general, vascular, and urological surgery. Anesthesiology. 2009;110:58-66. [ Links ]
23. Goldman L, Caldera DL, Nussbaum SR. Multifactorial index of cardiac risk in non cardiac surgical procedures. N Engl J Med. 1977;297:845-50. [ Links ]
24. Goldman L, Caldera DL, Southwick FS. Cardiac risk factors and complications in non cardiac surgery. Medicine. 1978;57:357-70. [ Links ]
25. Detsky A, Abrams HB, Forbath N. Cardiac assessment for patients undergoing non cardiac surgery. A multifactorial clinical risk index. Arch Intern Med. 1986;146:2131-4. [ Links ]
26. Lee TH, Marcantonio ER, Mangione CM. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999;100:1043-9. [ Links ]
27. Moran P, Ghidella T, Power G, Jenkins AS, Whittle D. The use of Lee and co-workers index to assist a risk adjusted audit of perioperative cardiac outcome. Anaesth Intensive Care. 2008;36:167-73. [ Links ]
28. Guilabert Sanz P. Eventos cardiovasculares adversos poscirugía no cardiaca de riesgo medio-alto: Estudio retrospectivo del 2009. Barcelona: Universidad Autónoma de Barcelona; 2011. [ Links ]
29. Serrano Valdés X. Valoración preoperatoria del paciente con cardiopatía isquémica. Rev Mex Anetesiol. 2007;30:338-45. [ Links ]
30. Puig-Barberà J, Márquez-Calderón S, Vila-Sánchez M. Complicaciones cardiacas en cirugía mayor programada no cardiaca: incidencia y factores de riesgo. Rev Esp Cardiol. 2006;59:329-37. [ Links ]
31. Eagle K, Brundage B, Chaitman B, Ewy G, Fleisher L, Hertzer N. Guidelines for perioperative cardiovascular evaluation for noncardiac surgery. Circulation. 1996;93:1278-317. [ Links ]
32. Eagle KA, Brundage BH, Chaitman BR. Guidelines for perioperative cardiovascular evaluation for noncardiac surgery. Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Perioperative Cardiovascular Evaluation for Noncardiac Surgery). J Am Coll Cardiol. 1996;27:910-48. [ Links ]
33. Tarhan S, Moffitt EA, Taylor WF, Giuliani ER. Myocardial infarction after general anesthesia. JAMA. 1972;220:1451-4. [ Links ]
34. Falconi M, Barisani JL, Levín R, Sampó E, Vidal L, Amuchástegui LM, et al. Consenso de evaluación del riesgo cardiovascular en cirugía no cardíaca. Rev Argent Cardiol. 2005;73:381-96. [ Links ]
35. Ochoa Montes LA, González Lugo M, Tamayo Vicente ND, Romero del Sol JM, Correa Azahares DP, Miguélez Nodarse R, et al. La lesión aterosclerótica en la muerte súbita cardíaca. Rev Haban Cienc Med. 2010;9:303-12. [ Links ]
36. Schouten O, Bax JJ, Poldermans D. Evaluación del riesgo coronario en el manejo de pacientes sometidos a cirugía vascular no cardiaca. Rev Esp Cardiol. 2007;60:1083-91. [ Links ]
37. Ackland G, Harris S, Ziabari Y, Grocott M, Mythen M. Revised cardiac risk index and postoperative morbidity after elective orthopedic surgery: A prospective cohort study. Br J Anaesth. 2010;105:744-52. [ Links ]
38. Freeman W, Gibbons RJ. Perioperative cardiovascular assessment of patients undergoing non-cardiac surgery. Mayo Clinic Proc. 2009;84:79-90. [ Links ]
39. Troncoso C. Evaluación preoperatoria. Rev Med Clin Condes. 2011;22:340-9. [ Links ]
40. Quénet EH, Trémelot D, Marty LJ. Exploraciones cardíacas preoperatorias en cirugía no cardíaca. EMC-Anestesia-Reanimación. 2011;37:1-9. [ Links ]
41. Rivera Bocanegra JC, Salazar Caicedo J. Arritmias intraoperatorias: nodo sinusal enfermo manifestado durante anestesia general. Rev Colomb Anestesiol. 2011;39:259-65. [ Links ]
42. Villalba JC. Cambios en el segmento ST del EKG durante la anestesia: en qué pensar. Rev Colomb Anestesiol. 2012;40:175. [ Links ]
43. Fernández Ramos H, Pantoja Muñoz HJ, Pozo Romero JA, Correa Borrell M. Valor predictivo del índice multifactorial de riesgo cardiaco de Goldman para cirugía no cardiaca. Rev Cubana de Anestesiología y Reanimación. 2011;10:91-100. [ Links ]
44. Williams F, Bergin J. Evaluación cardiaca antes de la cirugía no cardiaca. Surg Clin North Am. 2009;89:747-62. [ Links ]
45. Turkstra T, Jones PM. Simplifying the non-cardiac surgery evaluation pathway. Anesth Analg. 2009;108:383-4. [ Links ]
46. Magdaleno Maldonado GE, Páez Lizárraga LM. Análisis retrospectivo de los índices de riesgo cardiaco de Goldman y Detsky utilizados en la cirugía electiva no cardiaca. Rev Sanid Milit Mex. 2010;64:224-32. [ Links ]
47. Junker G. Valoración del riesgo operatorio en cirugía no cardíaca. Rev Urug Cardiol. 2011;26:173-8. [ Links ]
48. Poldermans D, Bax JJ, Boersma E, de Hert S, Eeckhout E, Fowkes G, et al. Guía de práctica clínica para la valoración del riesgo cardiaco preoperatorio y el manejo cardiaco perioperatorio en la cirugía no cardiaca. Rev Esp Cardiol. 2010;63:502. [ Links ]
49. Grover FL, Edwards FH. Objective assessment of cardiac risk for noncardiac surgical patients an up-to-date simplified approach. Circulation. 2011;124:376-7. [ Links ]
50. Gupta PK, Gupta H, Sundaram A, Kaushik M, Fang X, Miller WJ, et al. Development and validation of a risk calculator for prediction of cardiac risk after surgery clinical perspective. Circulation. 2011;124:381-7. [ Links ]
